

Abstract
Background:
Heart failure is one of the chronic heart diseases and a debilitating condition of increased prevalence in the elderly. One of the important and non-pharmacological strategies for improving clinical outcomes in these patients is promotion of the self-care. Background and social environment in which a patient is trying to control his disease is an important factor in the self-care. The aim of this study was to evaluate the effects of family support intervention on the self-care behaviors in patients with heart failure.
Materials and Methods:
This study was a randomized clinical trial conducted in university hospitals in Isfahan, Iran, in 2012. A total of 62 patients with heart failure were randomly assigned to experimental (n = 32) and control (n = 32) groups. Supportive intervention including three educational sessions with the delivery of educational booklet and follow-up by telephone was performed for caregivers of patients in the experimental group. Data were collected using the questionnaire of self-care behaviors, which was completed before and 1 month after the intervention in both the groups, and the questionnaires were analyzed using descriptive statistics and independent and paired t-tests.
Results:
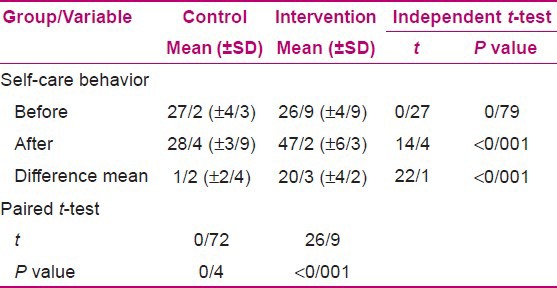
The results indicate that after the intervention, self-care behavior scores in the experimental group and control group were 47.2 and 28.4, respectively, and independent t-test revealed that the difference was statistically significant.
Conclusion:
Family-focused supportive interventions can be used as an effective method for improving the self-care behaviors in patients with heart failure.
Keywords: Behavior, family support, heart failure, Iran, self-care
INTRODUCTION
Cardiovascular problems are one of the important reasons for diseases and mortality in the world.[1] One of the most common cardiac diseases is congestive heart failure, with the highest incidence, mortality, and hospitalization.[2] This is the only cardiac disease with a progressive incidence and mortality, in which almost 10% of the individuals over 75 years of age are involved.[3] The reported statistics reveal an increase in its mortality by six times in the last 40 years, indicating that about 300,000 people expired yearly directly or indirectly due to heart failure.[4] On the other hand, this disease is so disabling and costly that over 70% of the patients are readmitted in a hospital 3 months after their initial discharge,[5] imposing a high financial burden to health care systems.[6] One of the important strategies to promote clinical outcomes in these patients is promotion of self-care behaviors.[7] Self-care in heart failure contributes to issues such as medical and food diet, limitation of intake of sodium and fluids, daily weighing, level of permitted activities, and a decision for appropriate therapeutic interventions when the disease gets worse.[8]
Various researches show that self-care behavior can significantly diminish the number of hospitalizations, mortality, and care cost burdens.[8,9,10,11] In patients with heart failure, administration of self-care is difficult as a result of the complicated medical diet, the chronic nature of the disease, as well as the complications in various systems of the body which result in lower self-care. Therefore, provision of an efficient support for self-care is essential and important.[12]
Family as the most important source of social support is tightly related with self-care activities.[9] Since most of the patients with heart failure live with other family members at their home, participation and support of family members can play a key role in self-care behaviors and efficiency of disease control.[13] Therefore, family can influence a patient's success and stability of their behavior change in self-care programs.[14] Several studies revealed the association between family support and heart failure patients’ self-care.[8,9] Earlier studies showed that the patients with more support had better compliance of self-care health behaviors.
Gallager et al. showed the self-care behaviors such as restricting fluid intake, regular medication, sports, and referring to physicians in case of observed overweight among the patients who had received more support.[15] Sayers et al. showed that the level of family support was directly associated with medical and food diets and other dimensions of self-care in heart failure patients.[16]
Meanwhile, most of the families, especially the caregivers, have low knowledge about the disease and its signs and treatment, and do not know what is beneficial for the patients or how they can support and encourage the patients to follow self-care behaviors.[13] Nurses, with their unique position in family members,[17] can play a key role in support, education, counseling, and taking care of heart failure patients and their caregivers.[18] They can familiarize the family members, especially caregivers, with these behaviors, which act as a knowledgeable and capable source of family-focused nursing interventions to give a better support to these patients.[19,20]
Despite evidences proving the important role of family support in heart failure patients’ self-care, family-focused supportive interventions with goal of their clinical outcomes’ promotion have been less conducted among these patients.[8] On the other hand, the researcher, despite searching thoroughly, did not find any studies on family-focused supportive care in heart failure patients in Iran. Therefore, the present study aimed to define the effect of family supportive intervention on heart failure self-care behaviors.
MATERIALS AND METHODS
The present study was a pre- and post-test case and control clinical trial conducted in the selective university hospitals in Isfahan, Iran, in 2012. It aimed to study the effect of family support intervention on self-care behavior in heart failure patients. The study population comprised the patients diagnosed with heart failure referring to selected hospitals. Inclusion criteria were: Confirmation of heart failure diagnosis by a cardiologist, being in grade II, III, or IV of heart failure based on American Heart Association Classification, having history of at least one time hospitalization due to cardiac failure, at least 1 year of experience of heart failure, being over 21 years of age, complete consciousness, no history of myocardial infarction (MI) or heart surgery in the past 6 months, no history of other chronic or disabling diseases except cardiovascular risk factors (diabetes, hypertension, and hyperlipidemia), having a family, not living alone and the caregiver being from the family members, being over 18 years of age, and being literate.
The sample size was calculated to be 36 heart failure patients in each group of study and control. A total of 62 patients with heart failure were initially selected by convenient sampling, and then randomly assigned to experimental and control groups equally.
The data collection tool was a two-section questionnaire. The first section of the questionnaire contained demographic characteristics, the existing data in patients’ medical profile (ejection fraction, disease grade, and consumed drugs), as well as some information about patients’ caregiver (age, sex, relation to the patient, length of care, and education level). The second section of the questionnaire inquired self-care behaviors. This questionnaire was designed by Shoji Fard et al., and its face and content validity and reliability were confirmed by experts’ panel, and Cronbach's alpha was 0.8. In this tool, 15 self-care activities were listed and investigated using a Likert's 5-point scale (from zero = never to 4 = always). Based on this scale, the obtained score can vary from 0 to 60. Scores of 0-20 were assigned to “poor,” 21-40 to “moderate,” and 41-60 to “good.”
After obtaining an informed written consent from the subjects and filling the self-care behaviors questionnaire, the subjects were assigned to study and control groups, and then family support intervention was conducted in the study group. Control group received conventional care and underwent no intervention in the present study.
The intervention program included three group educational sessions. As the subjects in the study group were from three medical centers, the patients’ caregivers in each center were considered as a control group and three sessions with 8-12 attendees were held for each group. These sessions were held weekly for 1-1.5 h in an appropriate classroom in the same medical educational center.
In the first session, the caregivers were familiarized with the definition and heart failure disease process, its etiology and treatment, importance and manner of self-care behaviors, and related skills such as reading food labels and taking strategies to lower food salt intake. At the end of the first session, a booklet of heart failure self-care guidelines was distributed among the caregivers, not only to read but also to discuss the points with the other family members in order to be able to answer the questions related to the disease and administration of self-care indicated at the end of the booklet, with the cooperation of the patients. They were also asked to write down their possible questions and deliver them to the researcher in the following session.
In the second session, patients’ and caregivers’ responses to the questions in the booklet were collected and their learning and practical administration of the learned issues were evaluated, and the required guides were given to the caregivers. Then, the importance and role of family in disease control and patients’ care was explained. The caregivers held group discussions about living with heart failure patients and the way of supporting them. In order to increase emotional and affective support toward these patients, efficient communication skills were also explained. Case scenario, role play of suggested strategies, and supportive discussion were adopted to empower and practice learned skills. At the end of the second session, the caregivers were given a booklet about the importance and manner of patients’ practical and emotional support, and they were asked to pass it among the other family members.
In the third session, caregivers gave examples of the patient supportive strategies taken, and communication as well as prohibiting and facilitating factors they faced during the latest week. Then, some indications about the manner of self-care as well as other related points were explained to finalize the subject and get a conclusion during the sessions. At the end of the third session, a contact number was given to the caregivers in order to get answers for their disease-related and self-care-related questions. Phone call follow-ups were carried out for 2 weeks to guide the subjects and answer their questions.
One month after the group sessions and 1 month after the introductory test in control group, self-care behavior questionnaire was again filled up for the subjects in both the groups. The data were analyzed by descriptive and analytical statistics through SPSS version 12. In analytical statistical tests, P < 0.05 was considered significant.
In the present study, letter of introduction issued by Isfahan Nursing and Midwifery School was delivered to the authorities of research environment. Research goals were explained to the subjects and their written informed consent was obtained. The subjects were also assured that their personal information would be kept confidential by the researcher, and the subjects were free to leave the research any time they wanted to.
RESULTS
In the present study, 81 heart failure patients entered and filled the initial questionnaire. Before the subjects’ random allocation, nine subjects were excluded from the study (three patients died and six were not interested to attend). During the study, four subjects dropped out of control group (two died and two were not available). In the study group, four subjects dropped out (two did not participate in all stages of the research and two died). Finally, the data of 64 scores were investigated.
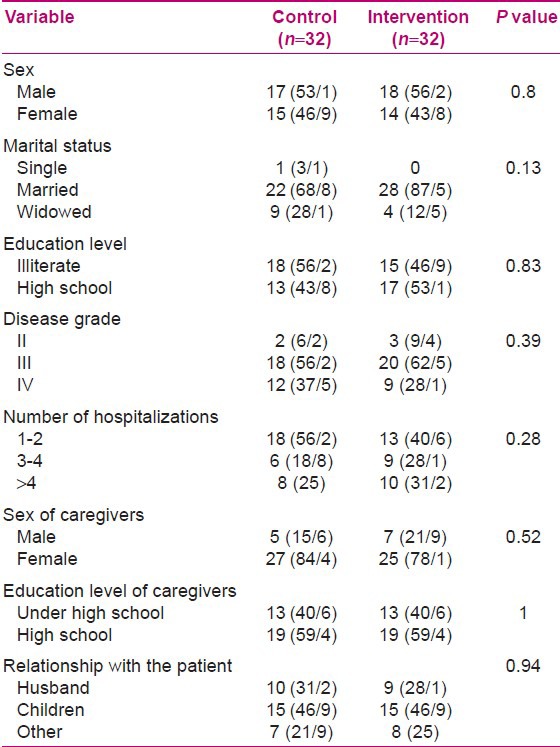
Research findings showed that the subjects were identical in both groups concerning age; sex; marital status; education level; grade of disease; hospitalization history; sex, age, and education level of caregivers; relationship of the caregiver with the patient; and length of care. Most of the subjects in both groups were males (54.6%), married (87.15%), illiterate (51.55%), and in grade III of the disease (59.35%). They had one to two times history of hospitalization due to heart failure. Most of the caregivers were females (81.2%), had education level of high school and lower (81.2%), and were the children of the patients (46.9%). Demographic characteristics of the subjects in each group are presented and compared in Table 1.
Table 1.
Demographic characteristics of patients and caregivers
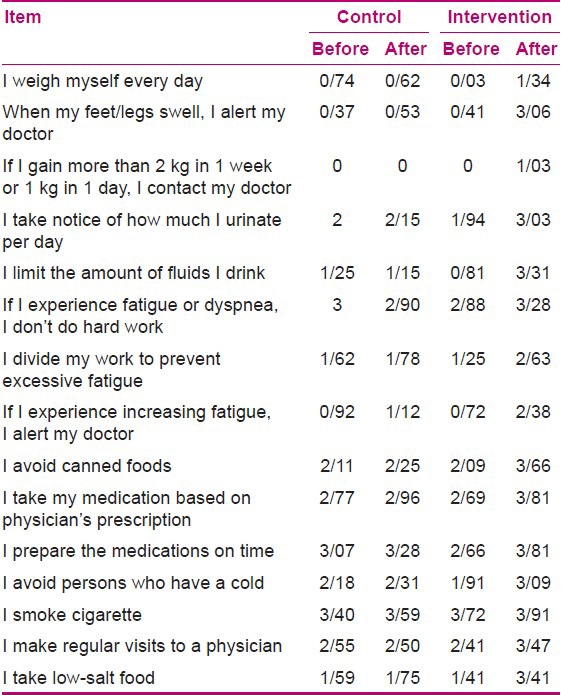
In Table 2, it is observed that the highest mean scores of each self-care behavior before intervention in both the study and control groups were for not smoking, drug consumption based on doctor's prescription, time of preparation of the medications, regular visits to a physician, and avoiding canned foods, respectively. Meanwhile, the lowest self-care behavior mean scores were for visiting a physician due to an observed overweight, daily weighing, and fluid restriction compliance and intake of low-salt food.
Table 2.
The comparison between each self-care behavior's mean score of the subjects in the intervention and control groups before and after the intervention
In Table 3, it is seen that there was no significant difference between self-care behavior mean scores in the two groups of study and control before intervention (P = 0.79), but there was a significant difference between self-care behavior mean scores in the two groups of study and control after intervention (P < 0.001).
Table 3.
The comparison between self-care behavior mean scores of the subjects in the intervention and control groups before and after the intervention
DISCUSSION
The results of the present study show that administration of supportive intervention and promotion of family support led to promotion of self-care behavior in heart failure patients.
The results show that subjects had a moderate level of self-care behavior before intervention. Shoja Fard et al. and Gallager et al. reported subjects’ self-care behavior mean scores in the range of the present study, which is consistent with our findings.
The results obtained show that not smoking, taking the medications based on physician's prescription, preparation of the medications in time, regular visits to physicians, and avoiding canned foods were among the self-care behaviors, and were in a moderate level. Meanwhile, subjects’ function in the other behaviors such as daily weighing, intake of less salt, referring to a physician when observing the signs, and fluid restriction compliance were found to be poor. Gallager et al. also reported that medication intake based on physician's prescription was the most frequent self-care behavior practiced by the subjects, while daily weighing was the least.[15] In Sayers et al.'s report, 80% of the subjects mentioned intake of salty food.[16] Jaarsma et al. reported that lack of daily weighing in heart failure patients was as a result of the following factors: Either the subjects did not find it helpful or they did not have an appropriate tool for weighing or they could not interpret the results.[22] In the present study, the subjects mentioned being illiterate, not having scales available for daily weighing, and consideration of low importance as the reasons for lack of daily weighing.
The results of the present study showed that self-care behaviors in heart failure patients were promoted after supportive intervention and promotion of family support toward the patients. Dunbar et al. showed that supportive intervention and conducting group sessions with heart failure patients’ caregivers and counseling regarding the manner of positive and supportive communication of the family with the patients led to better compliance concerning following a low-salt diet.[23] Piette et al. showed that supportive strategies promoted self-care behaviors in the subjects.[24] The results of other researches also showed an association between social support from family side and self-care, as well as a positive association between family support and self-care,[15,16] which is consistent with the present study.
Contrary to the results obtained in the present study, Agren et al. argue that this finding may be due to the long time of follow-up and the inadequate interventions administered, and recommend further studies in this regard.[25] In the present study, the process of skills administration and use of supportive strategies was followed up, evaluated, and checked through phone calls and filling checklists in sessions’ intervals. On other hand, Lofvemark et al. showed that administration of a mere educational program for heart failure patients concerning care does not affect their level of re-hospitalization despite promotion of their caring knowledge.[26] Lack of an educational effect on clinical outcomes and self-care behaviors in the aforementioned study can show that knowledge alone is not adequate for a behavior change and promotion of self-care. In addition, Clark et al. reported a poor relationship between heart failure knowledge and self-care.[12]
In the present study, the goal was not just promotion of caregivers’ knowledge, but their familiarization with strategies and supportive communication in the direction of patients’ emotional support promotion. The researchers believe the observed patients’ self-care promotion may be as a result of caregivers’ participation in efficient communication skills’ education sessions, accompanied with the patients, and application of supportive communication and strategies by them leading to promotion of patients’ motivation toward conducting self-care.
In the present study, the highest promotion of self-care behavior was observed after administration of family supportive intervention in dimensions such as compliance to a low salt-diet, fluid restriction, and referring to a physician after observing the signs of disease. Heart failure patient's family plays a vital role in the control of signs and symptoms, and can help the patients to diagnose the symptoms of the disease getting worse earlier, encourage their compliance to a medical food diet, and support them through changes in their lifestyle. Gallager et al. showed that the patients who received more support by their spouses had better compliance to fluid restriction and referring to a physician.[15] Dunbar et al. also observed a significant reduction in daily sodium intake after family supportive interventions.[23]
One of the most important challenges in heart failure patients’ self-care is compliance to a low-salt diet. Since the self-care concerning compliance to a diet often occurs at home, family members can play a specific role in compliance to diet restrictions.[23] Therefore, making the family members familiar with the need for compliance to this behavior and patients’ encouragement to do it is of great importance.
CONCLUSION
The findings of the present study reveal the major and important role of family members’ support in self-care among congestive heart failure patients. Nurses, as the professionals in the field of health and with regard to their important role in support, education, and care of these patients and their caregivers, can support, educate, and guide these patients through family members’ education and designing appropriate care programs in order to take steps toward promotion of self-care. Designing, administration, and application of these supportive educational programs by family's participation can reveal the role of nurses in promotion of patients’ and community health behavior and self-care. Based on the findings of the present study, it is suggested to design and conduct more family-focused interventions and studies for promotion of self-care in other chronic diseases.
ACKNOWLEDGMENT
The authors would also like to acknowledge the Nursing and Midwifery Faculty, Isfahan University of Medical Sciences, for supporting this work. They would also like to thank all the people who made this study possible. This research article is derived from MSc thesis in the Isfahan University of Medical science No. 390458.
Footnotes
Source of Support: Nursing and Midwifery Faculty, Isfahan University of Medical Sciences
Conflict of Interest: None
REFERENCES
- 1.Attarchi MS, Boroumand M, Asghari Roudsari E. Return to work after cardiovascular diseases. J Legal Med Islamic Republic Iran. 2006;11:207–13. [Google Scholar]
- 2.Ghahramani A, Kamrani F, Mohamadzadeh SH. Effect of self care education on knowledge, performance and readmission in patient with heart failure. J Health Care. 2010;12:11–20. [Google Scholar]
- 3.Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. 12th ed. Philadelphia: Lippincott Williams and Wilkins; 2010. Brunner and Suddarth's text book of medical-surgical nursing; p. 825. [Google Scholar]
- 4.Black GM, Hawks GH. 8th ed. Philadelphia: Elsevier Saunders; 2009. Medical-surgical nursing clinical management for positive outcomes; p. 1431. [Google Scholar]
- 5.Woods SL, Froelicher ES, Motzer SU, Bridges EJ. 5th ed. Philadelphia: Lippincott Williams and Wilkins; 2010. Cardiac nursing; p. 555. [Google Scholar]
- 6.Urden LD, Stacy KM, Lough ME, Thelan S. 6th ed. Missouri: Mosby Elsevier; 2010. Critical care nursing diagnosis and management; p. 456. [Google Scholar]
- 7.Chriss P, Sheposh J, Carlson B, Riegel B. Predictors of successful heart failure self-care maintenance in the first three months after Hospitalization. Heart Lung. 2004;33:345–53. doi: 10.1016/j.hrtlng.2004.03.004. [DOI] [PubMed] [Google Scholar]
- 8.Riegel B, Moser DK, Anker SD, Lawrence JB, Dunbar SB, Kathleen L, et al. State of the science: Promoting self-care in persons with heart failure: A scientific statement from the American heart Association. Circulation. 2009;120:1141–63. doi: 10.1161/CIRCULATIONAHA.109.192628. [DOI] [PubMed] [Google Scholar]
- 9.Dunbar SB, Clark P, Quinn C, Gary R. Family influences on heart failure self-care and outcomes. J Cardiovasc Nurs. 2008;23:258–65. doi: 10.1097/01.JCN.0000305093.20012.b8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vander Wal MH, Jaarsma T, van V, Dirk J. Non-compliance in patients with heart failure; how can we manage it? Eur J Heart Failure. 2005;7:5–17. doi: 10.1016/j.ejheart.2004.04.007. [DOI] [PubMed] [Google Scholar]
- 11.Lee CS, Moser DK, Lennie TA, Riegel B. Event-free survival in adults with heart failure who engage in self-care management. Heart Lung. 2011;40:12–20. doi: 10.1016/j.hrtlng.2009.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Clark AM, Freydberg NM, Finlay A, Tsuyuki RT, Armstrong PW, Strain LA. Patient and informal caregivers’ knowledge of heart failure: Necessary but insufficient for effective self-care. Eur J Heart Failure. 2009;11:617–21. doi: 10.1093/eurjhf/hfp058. [DOI] [PubMed] [Google Scholar]
- 13.Clark AM, Margaret ER, Caroline EM, Simon C, Murdoch DL, John J. The complex nature of informal care in home based heart failure management. J Adv Nurs. 2007;61:373–83. doi: 10.1111/j.1365-2648.2007.04527.x. [DOI] [PubMed] [Google Scholar]
- 14.Molloy GJ, Johnston DW, Witham MD. Family care giving and congestive heart failure: Review and analysis. Eur J Heart Fail. 2005;7:592–603. doi: 10.1016/j.ejheart.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 15.Gallager R, Luttik ML, Jaarsma T. Social support and self-care in heart failure. J Cardiovasc Nurs. 2011:1–7. doi: 10.1097/JCN.0b013e31820984e1. [DOI] [PubMed] [Google Scholar]
- 16.Sayers SL, Riegel B, Pawlowsk IS, Coyne J. Social support and self-care of patients with heart failure. Ann Behav Med. 2008;35:70–9. doi: 10.1007/s12160-007-9003-x. [DOI] [PubMed] [Google Scholar]
- 17.Masoodi R, Alhani F, Moghadassi J, Ghorbani M. The effect of family-centered empowerment model on skill, attitude, and knowledge of multiple sclerosis caregivers. J Birjand Univ Med Sci. 2010;17:87–97. [Google Scholar]
- 18.Kang X, Zheng Li, Nolan MT. Informal caregivers’ experiences of caring for patients with chronic heart failure systematic review and meta synthesis of qualitative studies. J Cardiovasc Nurs. 2011:1–9. doi: 10.1097/JCN.0b013e3182076a69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Daugherty J, Saarmmann L, Riegel B, Sornborger K, Moser D. Can we talk? Developing a social support nursing intervention for couples? Clin Nurse Specialist. 2002;16:211–8. doi: 10.1097/00002800-200207000-00011. [DOI] [PubMed] [Google Scholar]
- 20.Saunders M. Family caregivers need support with heart failure patients. Holistic Nursing Pract. 2003;17:136–42. doi: 10.1097/00004650-200305000-00004. [DOI] [PubMed] [Google Scholar]
- 21.Shojae Fard J, Nadrian H, Baghiani Moghadam MH, Mazloomi SS, Sanati HR, Askarshahi M. Effect of education on self care of patient with heart failure. Payavard Salamat. 2009;2:43–55. [Google Scholar]
- 22.Jaarsma T, Halfen R, Abusaad H, Dracup K, Diederiks J. Self care and quality of life in patient with advanced heart failure: The effect of a supportive educational intervention. Heart Lung. 2000;29:319–30. doi: 10.1067/mhl.2000.108323. [DOI] [PubMed] [Google Scholar]
- 23.Dunbar SB, Clark PC, Deaton C, Smith AL, De AK, O’Brien MC. Family education and support interventions in heart failure: A pilot study. Nurs Res. 2005;54:158–66. doi: 10.1097/00006199-200505000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Piette JD, Gregor MA, Share D, Heisler M, Bernstein SJ, Koelling T, et al. Improving heart failure self-management support by actively engaging out-of-home caregivers: Results of a feasibility study. Congestion Heart Fail. 2008;14:12–8. doi: 10.1111/j.1751-7133.2008.07474.x. [DOI] [PubMed] [Google Scholar]
- 25.Agren S, Evangelista LS, Hjelm C, Stromberg A. Dyads affected by chronic heart failure: A randomized study evaluating effects of education and psychosocial support to patients with heart failure and their partners. J Cardiac Fail. 2012:1–8. doi: 10.1016/j.cardfail.2012.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lofvenmark C, Karlsson MR, Edner M, Billing E, Mattiasson AC. A group-based multi-professional education program for family members of patients with chronic heart failure: Effects on knowledge and patients’ health care utilization. Patient Educ Counseling. 2011;85:162–8. doi: 10.1016/j.pec.2010.09.026. [DOI] [PubMed] [Google Scholar]