

Abstract
Background:
The quality of life (QOL) has emerged as an important parameter for evaluating the quality of health-care for patients with renal failure. The literature suggests that many factors impact QOL. The QOL of dialysis patients in the United Arab Emirates (UAE) has not been studied before. This research examined the QOL of patients in the UAE on dialysis using two QOL tools.
Materials and Methods:
A descriptive comparative survey design was used to study 161 dialysis patients. The participants completed the 36-Item Short Form Health Survey (SF-36) and the QOL index dialysis version tool. Comparative analyses of the results for both tools were done using descriptive statistics. Multiple linear regression analysis determines the effect of the variables on the QOL scores.
Results:
The questionnaires return rate was 93%. The overall QOL for dialysis patients was rated low when self-assessed using the SF-36 (58.9) compared to QOL index (77.2). The multiple regression analysis revealed that having a chronic illness had the strongest impact on the total scores of both tools. The comparison between the statistically significant variables for both samples revealed contradictory results from the two tools used. This meant that the two tools measured QOL differently.
Conclusion:
The two QOL tools scores impacted very differently on most socio-demographic variables on the two samples. More studies are required to explore the concept of QOL in the Arab dialysis population.
Keywords: Dialysis, Islamic religion, quality of life, United Arab Emirates
INTRODUCTION
Interest in measuring quality of life (QOL) in both clinical trials and everyday clinical practice is on the increase. In addition, to mortality and morbidity as key indicators for performance, QOL is an important factor for evaluating the quality and outcome of healthcare for patients with chronic illnesses. The acknowledgment that the burden of chronic kidney failure extends beyond its impact on the biological structure of the body is reflected in the initiatives of the National Kidney Foundation in the United States of America (USA) to support efforts aimed at improving QOL in patients with kidney failure.[1]
Patients who have dialysis for survival live with a great deal of uncertainty about the future. They do not deal only with treatment-related complications such as left ventricular hypertrophy, arthrosclerosis and hyperparathyroidism,[2,3] but also with the changes in their perception of their own self-worth. The major psychological and physiological stresses experienced by patients on dialysis are pain, restriction of fluids, itching, discomfort, limitations in physical activity, fatigue, weaknesses, high cost of care, feelings of inadequacy, and negative moods.[4,5,6] Therefore, a dialysis schedule can significantly interfere with both professional and personal lifestyles.[7,8] These factors may contribute to the diminished QOL reported by patients on regular dialysis.[7,8,9]
The survey design was the most common approach used to study QOL in dialysis patients.[10,11,12,13] This study is one of the few that has compared two QOL tools on the same population and is also the first known study on QOL in the United Arab Emirates (UAE). Given what is known about the culture, religion and other social characteristics of this population, it was important not to assume the appropriateness of a particular tool. So, this study used the 36-Item Short Form Health Survey (SF-36) and QOL Index tools. The aims were to establish the QOL of patients on dialysis in the UAE, explore the impact of the physical, psycho-social, religious, cultural, and other demographic variables.
MATERIALS AND METHODS
Design and sample
This research used a descriptive survey design. All eligible hemodialysis (HEMO) patients (161) at Sheikh Khalifa Medical City (SKMC) in the UAE were recruited to participate in the study. Three inclusion criteria were used to ensure accurate data collection. The first criterion restricted participation to patients who had been on HEMO therapy for more than 3 months, to exclude the influence of metabolic factors such as uremic encephalopathy on the level of consciousness. The second criterion required that patients should have no apparent cerebro-vascular disease or serious intellectual impairment, to avoid miss-interpretation of the questions. The third criterion required participants to be over 18 years old, the legal age for informed consent.
Instruments
This research used the SF-36 and the dialysis version of the QOL Index tools. The SF-36 is a general tool, developed for use on all populations irrespective of health or illness. In contrast, the QOL Index is a disease-specific tool. It measures satisfaction and importance of determinants of QOL. Both tools have well established reliability and validity studies.[14,15,16]
Ethical consideration
Prior to the commencement of the study, approvals were obtained from the Human Ethics Committee at Victoria University of Wellington and SKMC Ethics Committee in 2007. Also, the authors were granted approval to use the QOL tools. Participants were given full privacy when answering the survey questions and were reassured of the maintenance of confidentiality.
Data collection
An independent nurse went to the potential participants and gave them the invitation letter which explained the purpose of the research. Those willing to participate were asked to sign a consent form. They were then given the survey package containing the demographic survey, QOL Index dialysis version, SF-36 tools and an addressed envelope for the return of the surveys.
Data analysis
Data were analyzed using the SPSS software for Windows version 13.0 (SPSS Inc., Chicago, IL, U.S.A.). Descriptive statistics such as frequencies presented as percentages, mean, range and standard deviation were used. Following this descriptive analysis, several variables were regrouped to enable the planned regression analyses to be completed.
RESULTS
Return rates
A total of 161 patients signed the consent form and received the survey package during their regular dialysis schedule. Two patients declined to participate after they had looked at the survey, and five did not return the survey packages. Of the 154 packages returned, four were blank. The sample, therefore, consisted of 150 respondents, which is equivalent to a 93% return rate.
Demographic of the samples
The sample covered a wide range of ages from 19 years to 86 years. Over half (53.4%) of the respondents were over 50 years. The demographic data of the sample is summarized in Table 1.
Table 1.
Demographics of the sample
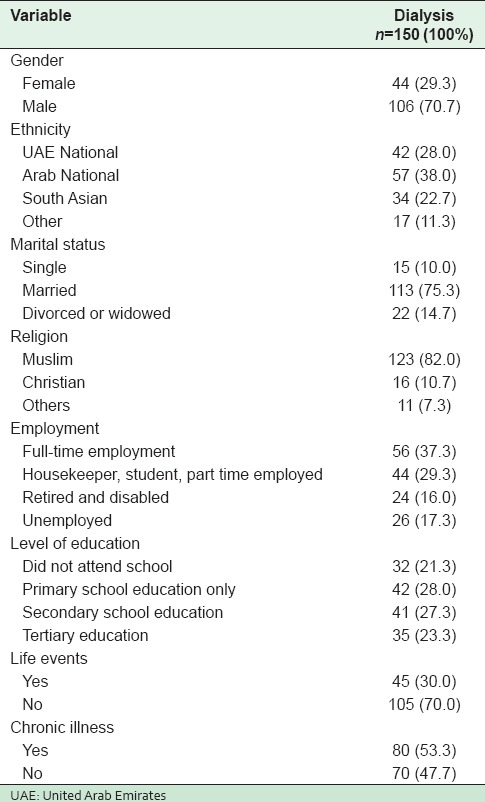
The above table shows that males predominated. The distribution of the ethnicities within the sample varied: UAE nationals accounted for approximately a quarter of the respondents. Over a third of the respondents (38%) were Arab. The majority of the respondents (82%) were Muslims. More than half of the sample suffered from chronic illnesses other than kidney failure. However, no data were collected on the types of chronic illnesses the patients had. Approximately, one-third did not know the cause of their kidney failure. Further results are summarized in the above table.
Findings from QOL tools and their subscales analyses
Descriptive statistics was used to calculate the mean and the standard deviation of the total scores and the subscales of the SF-36 tool. Table 2 presents the findings.
Table 2.
Total scores of SF-36 subscales
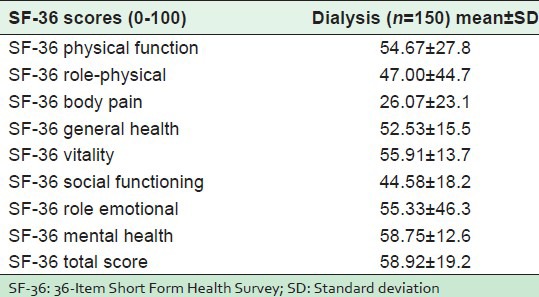
The Physical Health Component (PHC) of the SF-36 includes physical function, role-physical, body pain and general health subscales. The Mental Health Component (MHC) includes vitality, social functioning, emotional role and mental health subscales. The mean total score of the PHC was 45.1, and the MHC was 53.6. The highest mean scores with regard to the SF-36 were in the mental health subscale (58.8) and the lowest scores were in body pain subscale (26.1). Table 3 presents the findings from the QOL Index tool.
Table 3.
Total scores of QOL index subscales
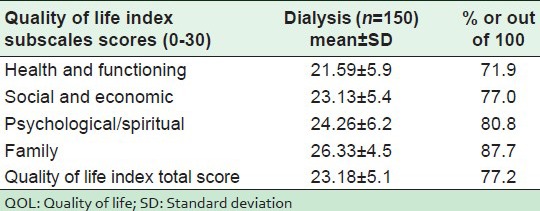
The QOL Index scores ranged from 0 to 30, with 0 as the lowest score and 30 as the highest score. For an accurate and easy comparison of the two tools, the QOL Index scores were transformed to 0-100. On this scale, 0 is the lowest score while 100 is the highest score. Findings on the QOL Index were all well above the midpoint of the scale and subscales. The highest score was in the family subscale followed by the psychological/spiritual subscale, and the lowest in the health and functioning subscale.
Given that none of the subscale components of the two tools are directly comparable, a comparison of scores of the two instruments can only be made on the total scores. This comparison indicates that dialysis respondent's overall mean QOL is rated higher when self-assessed using the QOL Index (77.2 vs. 58.92) than the SF-36.
The relationship between the SF-36 total scores and the independent variables
This phase of the analysis involved a series of statistical tests to establish what socio-demographics and life factors correlated with or had an impact on the SF-36 scores. Pearson's correlations were used for continuous variables, Spearman's correlation for ordinal data and t test or one way ANOVA for nominal variables. Table 4 summarizes the findings from the comparison between the demographic variables and SF-36.
Table 4.
The relationship between the demographic variables and SF-36 total scores
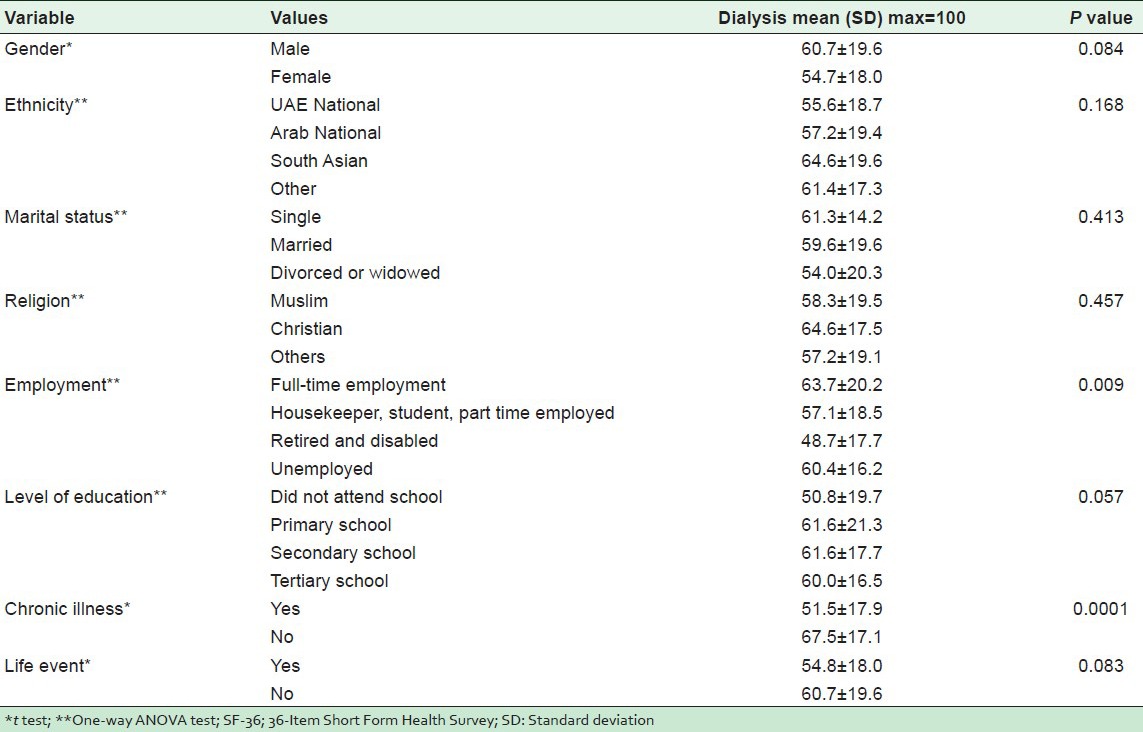
The t-test comparison of the total SF-36 scores with the nominal demographic variables found that respondents with another chronic illness had a statistically significant lower QOL scores (P = 0.0001). The respondents who had full-time employment had significantly higher mean total scores. The one-way ANOVA test comparison on the SF-36 total scores with the categorical demographic variables found that the employment variable had a statistically significant impact on the total scores (P = 0.009). Moreover, respondents who had full-time employment had on average 6.6 points higher than housekeepers, students, and those with part time employment. Further results are summarized in the above table.
The relationship between the QOL Index total scores and the independent variables
Table 5 presents the findings from the comparison of the demographic variables and the QOL Index total scores.
Table 5.
Comparison of the findings between the demographic variables and QOL index total scores
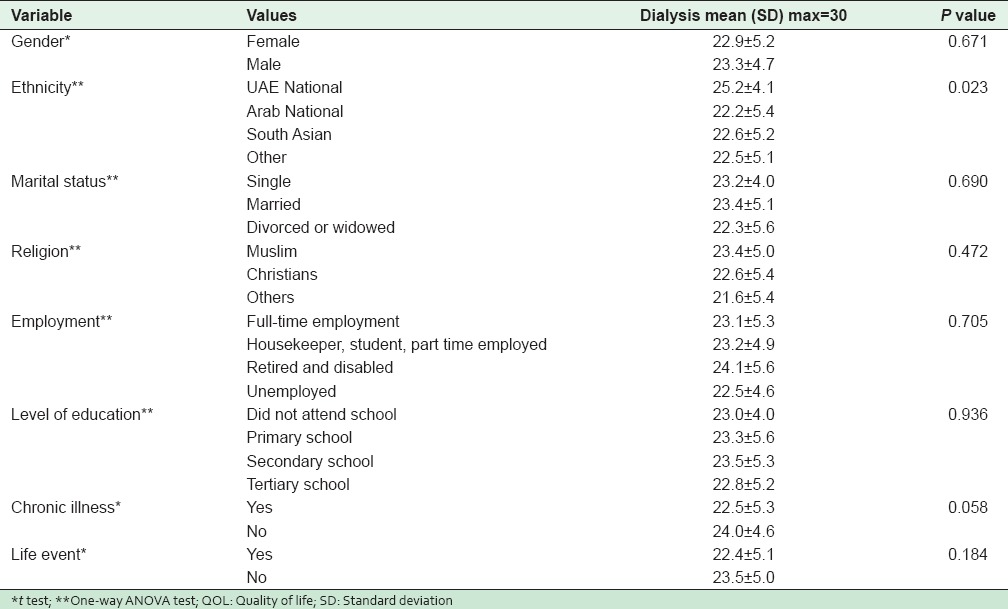
The t-test comparison of average QOL Index total scores with the nominal demographic variables found that the chronic illness variable was statistically significant (P = 0.058). The one-way ANOVA test found that the ethnicity variable had a statistically significant impact on the total scores (P = 0.023). The above table shows that on the average patients on dialysis who were UAE nationals had 3.0 points higher than other Arab nationals, 2.6 point higher than South East Asians and 2.7 points higher than respondents of other nationalities. Further results are summarized in the above table.
To identify factors with possible significant influence on QOL tools, standard multiple regression analyses were undertaken. They were done separately using both QOL tools to examine the effect of the predictor variables on the outcome variables. The multiple regression results on the demographic variables using SF-36 showed that the chronic health problems variables were statistically significant determinants of QOL. On the other hand, the multiple regression results on the demographic variables using QOL Index showed that variables on years on dialysis, chronic health problems and living in the UAE were statistically significant determinants of QOL.
DISCUSSION
The findings from the SF-36
Gender is a significant predictor of pain perceptions because women are more likely to report pain than men.[17] The reported mean scores of the body pain subscale in males were less than the females (24.34 vs. 30.23 respectively). These findings contradict several studies that have documented that women had a higher prevalence of most pain related conditions.[18,19] Women cope more actively with pain by speaking about it, and seeking help.[17]
The respondents had on average lower scores on the physical role and the physical function subscales than expected because the dialysis respondents have at least one chronic illness (kidney failure). Living with a chronic disease impacts negatively on education, employment, caregivers and everyday life.[20,21]
A comparison of this research finding with a study done on dialysis patients in Taiwan,[22] showed that the respondents on dialysis who come from the UAE scored higher in all subscales except the body pain, social functioning and mental health subscales. These findings also support the argument that people from different cultures and ethnicities perceive and respond to pain differently. The mean total score of the PHC was 45.1, and the MHC was 53.6. These findings were lower than what was reported from the Brazilian study on 140 dialysis patients that found the PHC scale at 57.5 and MHC at 73.6.[23] In contrast, the findings from the UAE study are considered relatively higher than the Iranian study on 250 Iranian patients on dialysis which reported the lower scores of 41.2 on the PHC and 47.5 on the MHC.[24]
The findings from the QOL index
The health and functioning subscale scores were relatively low, but the family subscale scores were relatively high. The total scores of the QOL index (23.18) were high in contrast to another study,[25] that used the QOL index to study 16 HEMO patients and eight pre-dialysis patients and reported lower scores except on the family subscale (22.5, 18.4 respectively).
The relationship between the socio-demographic variables and the total scores of both tools
Gender
The finding that the gender variable did not show any statistically significant relationship with the total scores of SF-36 and the QOL Index tools was similar to a study in the USA on 339 HEMO outpatients, 181 of whom men aged 54.7 ± 14.5 years, selected from seven dialysis units in Los Angeles South/East Bay area.[26] Other studies[27,28,29] found that male patients on dialysis had higher SF-36 scores. The reason for this gender difference in different studies remains speculative. Possible explanations could include biological factors and biases in the provision of care according to gender.[30] Other explanations could be differences in the clinician's attitudes towards female patients.[31]
Ethnicity
Ethnicity made a statistically significant difference in the total scores of the QOL index favoring people with a UAE nationality (P = 0.023), thus contradicting the finding in the SF-36 tool. No studies were found in the literature that compared the QOL of UAE Nationals, Arab Nationals, South East Asia Nationals and other nationalities. Several studies involving patients who receive HEMO in the USA found that African Americans reported higher SF-36 total scores than white Americans.[28,32,33,34] Variation across cultures may illustrate disparities in the management of disease in different countries.[24] The differences in the findings with regard to the ethnicity variable could stem from possible inadequate sensitivity of SF-36 to the effect of differences on QOL.
Marital status
Marital status did not have any statistically significant influence on the total scores of two tools. This result was similar to other studies that measured the QOL of dialysis patients using SF-36.[9,22,23] In contrast, the finding differs from another study which argued that the quality of the marital relationship is a stronger predictor of health outcomes than just being married, especially when people face great life challenges resulting from complications of disease and associated physical and psychological stresses.[35]
Employment
This study showed that having full-time employment had a statistically significant positive influence on the SF-36 total scores (P = 0.009) but did not have any statistically significant influence on the QOL index total scores (P = 0.705). The possible explanation may be that the tools measure QOL differently and that one of them may be more sensitive than the other in measuring the impact of employment on QOL. Another study reported that status of work was associated with higher QOL scores.[22] In contrast, other studies have reported lower scores on the SF-36 on dialysis patients who were employed.[23] In the Middle East, employers are usually reluctant to hire workers on dialysis because of frequent absence from work to go for a medical follow-up.
Education
The variable on educational level had no effect on the total scores of both tools. This finding differs from findings from other studies that have linked a higher educational level with better QOL.[22,34,36,37] Acaray and Pinar,[10] reported that most of QOL dimensions in the SF-36 increased as the educational status rose. Another study that examined the differences in QOL on 680 HEMO patients at seven medical centers in USA using QOL Index tool linked a higher level of educational and acquired skills with the ability to adjust to physical incapability.[38]
Religion
The variable on religion did not have any impact on the total scores of both tools. No studies were found in the literature that had similar religious groupings as the UAE study. However, spirituality has been examined in a few studies that explored the QOL of dialysis patients. These studies suggest that there was a positive relationship between the score on a spiritual beliefs scale and global QOL measures, satisfaction with life and perception of depression.[7,39]
Age
The study found that age did not have any statistically significant correlation with the total scores of the SF-36, which is contradictory to the finding by another study that found an association between higher SF-36 scores and younger age.[23] Advanced age has been linked with the deterioration of physical activity, thus giving lower SF-36 total scores in dialysis patients. In contrast, another study reported that older patients were more satisfied with their life on dialysis and accepted their limitations better than younger patients.[40] The absence of any statistically significant correlation of age with the total scores of the QOL index for the sample differs from the finding by another study that used the same tool and found that some of the QOL index scores increased with age. They suggested that older chronically ill patients tended to exhibit a greater level of contentment with their health and social status.[41]
Chronic health problems
Chronic illnesses are considered important contributing factors to clinical outcomes and QOL.[26] This study found that those who had another chronic illness had lower scores in both tools. This is expected because kidney failure impacts negatively on patients’ physical, psycho-social and economic well-being.[6] Associated diseases, especially diabetes mellitus, are strongly related to the worst QOL scores in ESRD patients on dialysis.[42]
Regression analysis
The variable on having another chronic health problem was a statistically significant determinant of the QOL scores for dialysis respondents on both tools. These findings are supported by an Iranian study that performed a logistic regression analysis on the SF-36 Persian version on a sample of 250 Iranian hemodialysis patients.[24] Another study found that the presence of other co-morbid medical conditions were common in patients on dialysis, and were the main contributing factors to clinical outcomes and the QOL.[26] The HEMO Study, which is a 15-centre randomized clinical trial on the effects of HEMO dose and membrane flux on mortality and morbidity in HEMO patients, showed that the strongest predictor of QOL was coexisting medical conditions by a 37% increase in risk per 1-unit increment in the score on the index of a coexisting disease.[43]
CONCLUSION
This study reported slightly lower scores in all subscales of the SF-36 compared with several studies done in other countries. There are differences in the results from the two tools, indicating that the tools measured QOL differently. Respondents who had ongoing chronic health problems had lower QOL scores. This finding was supported by other international studies. Ethnicity had statistically significant differences in the total scores of the QOL Index in favor of UAE nationals. The chronic health problems variable had a statistically significant influence on the total scores of both tools.
The multiple regression analyses showed that the variable on chronic health problems is a statistically significant determinant of the total scores of SF-36. Furthermore, variables such as chronic health problems, living in the UAE, and ethnicity variables were statistically significant determinants of the QOL Index.
ACKNOWLEDGMENTS
The researcher would like to thank the medical administrations of SKMC, the renal unit dialysis patients, medical, and nursing colleagues for their unlimited support during data collection.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am J Kidney Dis. 2002;39:S1–266. [PubMed] [Google Scholar]
- 2.Drüeke TB, Eckardt KU. Role of secondary hyperparathyroidism in erythropoietin resistance of chronic renal failure patients. Nephrol Dial Transplant. 2002;17:28–31. doi: 10.1093/ndt/17.suppl_5.28. [DOI] [PubMed] [Google Scholar]
- 3.London GM, Pannier B, Guerin AP, Blacher J, Marchais SJ, Darne B, et al. Alterations of left ventricular hypertrophy in and survival of patients receiving hemodialysis: Follow-up of an interventional study. J Am Soc Nephrol. 2001;12:2759–67. doi: 10.1681/ASN.V12122759. [DOI] [PubMed] [Google Scholar]
- 4.Lok P. Stressors, coping mechanisms and quality of life among dialysis patients in Australia. J Adv Nurs. 1996;23:873–81. doi: 10.1046/j.1365-2648.1996.00893.x. [DOI] [PubMed] [Google Scholar]
- 5.Mok E, Tam B. Stressors and coping methods among chronic haemodialysis patients in Hong Kong. J Clin Nurs. 2001;10:503–11. doi: 10.1046/j.1365-2702.2001.00500.x. [DOI] [PubMed] [Google Scholar]
- 6.Welch JL, Austin JK. Stressors, coping and depression in haemodialysis patients. J Adv Nurs. 2001;33:200–7. doi: 10.1046/j.1365-2648.2001.01654.x. [DOI] [PubMed] [Google Scholar]
- 7.Kimmel PL, Emont SL, Newmann JM, Danko H, Moss AH. ESRD patient quality of life: Symptoms, spiritual beliefs, psychosocial factors, and ethnicity. Am J Kidney Dis. 2003;42:713–21. doi: 10.1016/s0272-6386(03)00907-7. [DOI] [PubMed] [Google Scholar]
- 8.Valderrábano F, Jofre R, López-Gómez JM. Quality of life in end-stage renal disease patients. Am J Kidney Dis. 2001;38:443–64. doi: 10.1053/ajkd.2001.26824. [DOI] [PubMed] [Google Scholar]
- 9.Merkus MP, Jager KJ, Dekker FW, de Haan RJ, Boeschoten EW, Krediet RT. Physical symptoms and quality of life in patients on chronic dialysis: Results of the Netherlands cooperative study on adequacy of dialysis (NECOSAD) Nephrol Dial Transplant. 1999;14:1163–70. doi: 10.1093/ndt/14.5.1163. [DOI] [PubMed] [Google Scholar]
- 10.Acaray A, Pinar R. Quality of life in Turkish haemodialysis patients. Int Urol Nephrol. 2005;37:595–602. doi: 10.1007/s11255-005-0397-8. [DOI] [PubMed] [Google Scholar]
- 11.Hicks LS, Cleary PD, Epstein AM, Ayanian JZ. Differences in health-related quality of life and treatment preferences among black and white patients with end-stage renal disease. Qual Life Res. 2004;13:1129–37. doi: 10.1023/B:QURE.0000031350.56924.cc. [DOI] [PubMed] [Google Scholar]
- 12.Merkus MP, Jager KJ, Dekker FW, Boeschoten EW, Stevens P, Krediet RT. Quality of life in patients on chronic dialysis: Self-assessment 3 months after the start of treatment. The Necosad study group. Am J Kidney Dis. 1997;29:584–92. doi: 10.1016/s0272-6386(97)90342-5. [DOI] [PubMed] [Google Scholar]
- 13.Neto JF, Ferraz MB, Cendoroglo M, Draibe S, Yu L, Sesso R. Quality of life at the initiation of maintenance dialysis treatment – A comparison between the SF-36 and the KDQ questionnaires. Qual Life Res. 2000;9:101–7. doi: 10.1023/a:1008918609281. [DOI] [PubMed] [Google Scholar]
- 14.Ferrans CE, Powers MJ. Psychometric assessment of the quality of life index. Res Nurs Health. 1992;15:29–38. doi: 10.1002/nur.4770150106. [DOI] [PubMed] [Google Scholar]
- 15.Halabi JO. Psychometric properties of the Arabic version of quality of life index. J Adv Nurs. 2006;55:604–10. doi: 10.1111/j.1365-2648.2006.03952_1.x. [DOI] [PubMed] [Google Scholar]
- 16.Hemingway H, Stafford M, Stansfeld S, Shipley M, Marmot M. Is the SF-36 a valid measure of change in population health? Results from the Whitehall II study. BMJ. 1997;315:1273–9. doi: 10.1136/bmj.315.7118.1273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Affleck G, Tennen H, Keefe FJ, Lefebvre JC, Kashikar-Zuck S, Wright K, et al. Everyday life with osteoarthritis or rheumatoid arthritis: Independent effects of disease and gender on daily pain, mood, and coping. Pain. 1999;83:601–9. doi: 10.1016/S0304-3959(99)00167-0. [DOI] [PubMed] [Google Scholar]
- 18.Ghezeljeh TN, Momtahen M, Tessma MK, Nikravesh MY, Ekman I, Emami A. Gender specific variations in the description, intensity and location of angina pectoris: A cross-sectional study. Int J Nurs Stud. 2010;47:965–74. doi: 10.1016/j.ijnurstu.2009.12.021. [DOI] [PubMed] [Google Scholar]
- 19.Lund I, Lundeberg T. Is it all about sex? Acupuncture for the treatment of pain from a biological and gender perspective. Acupunct Med. 2008;26:33–45. doi: 10.1136/aim.26.1.33. [DOI] [PubMed] [Google Scholar]
- 20.Belasco A, Barbosa D, Bettencourt AR, Diccini S, Sesso R. Quality of life of family caregivers of elderly patients on hemodialysis and peritoneal dialysis. Am J Kidney Dis. 2006;48:955–63. doi: 10.1053/j.ajkd.2006.08.017. [DOI] [PubMed] [Google Scholar]
- 21.Liem YS, Bosch JL, Arends LR, Heijenbrok-Kal MH, Hunink MG. Quality of life assessed with the medical outcomes study short form 36-Item health survey of patients on renal replacement therapy: A systematic review and meta-analysis. Value Health. 2007;10:390–7. doi: 10.1111/j.1524-4733.2007.00193.x. [DOI] [PubMed] [Google Scholar]
- 22.Kao TW, Lai MS, Tsai TJ, Jan CF, Chie WC, Chen WY. Economic, social, and psychological factors associated with health-related quality of life of chronic hemodialysis patients in northern Taiwan: A multicenter study. Artif Organs. 2009;33:61–8. doi: 10.1111/j.1525-1594.2008.00675.x. [DOI] [PubMed] [Google Scholar]
- 23.Bohlke M, Nunes DL, Marini SS, Kitamura C, Andrade M, Von-Gysel MP. Predictors of quality of life among patients on dialysis in southern Brazil. Sao Paulo Med J. 2008;126:252–6. doi: 10.1590/S1516-31802008000500002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pakpour AH, Saffari M, Yekaninejad MS, Panahi D, Harrison AP, Molsted S. Health-related quality of life in a sample of Iranian patients on hemodialysis. Iran J Kidney Dis. 2010;4:50–9. [PubMed] [Google Scholar]
- 25.Parker KP, Bliwise DL, Bailey JL, Rye DB. Polysomnographic measures of nocturnal sleep in patients on chronic, intermittent daytime haemodialysis vs those with chronic kidney disease. Nephrol Dial Transplant. 2005;20:1422–8. doi: 10.1093/ndt/gfh816. [DOI] [PubMed] [Google Scholar]
- 26.Kalantar-Zadeh K, Kopple JD, Block G, Humphreys MH. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J Am Soc Nephrol. 2001;12:2797–806. doi: 10.1681/ASN.V12122797. [DOI] [PubMed] [Google Scholar]
- 27.Covic A, Seica A, Gusbeth-Tatomir P, Gavrilovici O, Goldsmith DJ. Illness representations and quality of life scores in haemodialysis patients. Nephrol Dial Transplant. 2004;19:2078–83. doi: 10.1093/ndt/gfh254. [DOI] [PubMed] [Google Scholar]
- 28.Kutner NG, Zhang R, Brogan D. Race, gender, and incident dialysis patients’ reported health status and quality of life. J Am Soc Nephrol. 2005;16:1440–8. doi: 10.1681/ASN.2004080639. [DOI] [PubMed] [Google Scholar]
- 29.Morsch CM, Gonçalves LF, Barros E. Health-related quality of life among haemodialysis patients – Relationship with clinical indicators, morbidity and mortality. J Clin Nurs. 2006;15:498–504. doi: 10.1111/j.1365-2702.2006.01349.x. [DOI] [PubMed] [Google Scholar]
- 30.Mustard CA, Kaufert P, Kozyrskyj A, Mayer T. Sex differences in the use of health care services. N Engl J Med. 1998;338:1678–83. doi: 10.1056/NEJM199806043382307. [DOI] [PubMed] [Google Scholar]
- 31.Safran DG, Rogers WH, Tarlov AR, McHorney CA, Ware JE., Jr Gender differences in medical treatment: The case of physician-prescribed activity restrictions. Soc Sci Med. 1997;45:711–22. doi: 10.1016/s0277-9536(96)00405-4. [DOI] [PubMed] [Google Scholar]
- 32.Kutner NG, Devins GM. A comparison of the quality of life reported by elderly whites and elderly blacks on dialysis. Geriatr Nephrol Urol. 1998;8:77–83. doi: 10.1023/a:1008384814079. [DOI] [PubMed] [Google Scholar]
- 33.Kutner NG, Brogan D, Fielding B, Hall WD. Black/white differences in symptoms and health satisfaction reported by older hemodialysis patients. Ethn Dis. 2000;10:328–33. [PubMed] [Google Scholar]
- 34.Lopes AA, Bragg-Gresham JL, Goodkin DA, Fukuhara S, Mapes DL, Young EW, et al. Factors associated with health-related quality of life among hemodialysis patients in the DOPPS. Qual Life Res. 2007;16:545–57. doi: 10.1007/s11136-006-9143-7. [DOI] [PubMed] [Google Scholar]
- 35.Morgan MA. Considering the patient-partner relationship in cancer care: Coping strategies for couples. Clin J Oncol Nurs. 2009;13:65–72. doi: 10.1188/09.CJON.65-72. [DOI] [PubMed] [Google Scholar]
- 36.Manns B, Johnson JA, Taub K, Mortis G, Ghali WA, Donaldson C. Quality of life in patients treated with hemodialysis or peritoneal dialysis: What are the important determinants? Clin Nephrol. 2003;60:341–51. doi: 10.5414/cnp60341. [DOI] [PubMed] [Google Scholar]
- 37.Moreno F, López Gomez JM, Sanz-Guajardo D, Jofre R, Valderrábano F. Quality of life in dialysis patients. A Spanish multicentre study. Spanish cooperative renal patients quality of life study group. Nephrol Dial Transplant. 1996;11:125–9. doi: 10.1093/ndt/11.supp2.125. [DOI] [PubMed] [Google Scholar]
- 38.Mozes B, Shabtai E, Zucker D. Differences in quality of life among patients receiving dialysis replacement therapy at seven medical centers. J Clin Epidemiol. 1997;50:1035–43. doi: 10.1016/s0895-4356(97)00127-3. [DOI] [PubMed] [Google Scholar]
- 39.Patel SS, Shah VS, Peterson RA, Kimmel PL. Psychosocial variables, quality of life, and religious beliefs in ESRD patients treated with hemodialysis. Am J Kidney Dis. 2002;40:1013–22. doi: 10.1053/ajkd.2002.36336. [DOI] [PubMed] [Google Scholar]
- 40.Valderrábano F. Erythropoietin in chronic renal failure. Kidney Int. 1996;50:1373–91. doi: 10.1038/ki.1996.452. [DOI] [PubMed] [Google Scholar]
- 41.Greene R. Using the ferrans and powers quality of life index of dialysis: A comparison of quality of life in older and younger African Americans receiving hemodialysis. Top Geriatr Rehabil. 2005;21:230–2. [Google Scholar]
- 42.Bakewell AB, Higgins RM, Edmunds ME. Quality of life in peritoneal dialysis patients: Decline over time and association with clinical outcomes. Kidney Int. 2002;61:239–48. doi: 10.1046/j.1523-1755.2002.00096.x. [DOI] [PubMed] [Google Scholar]
- 43.Unruh M, Benz R, Greene T, Yan G, Beddhu S, DeVita M, et al. Effects of hemodialysis dose and membrane flux on health-related quality of life in the HEMO study. Kidney Int. 2004;66:355–66. doi: 10.1111/j.1523-1755.2004.00738.x. [DOI] [PubMed] [Google Scholar]