

Abstract
The complications of long-term levodopa therapy for Parkinson’s disease (PD) include motor fluctuations, dyskinesias, and also nonmotor fluctuations—at least equally common, but less well appreciated—in autonomic, cognitive/psychiatric, and sensory symptoms. In seeking the pathophysiologic mechanisms, the leading hypothesis is that in the parkinsonian brain, intermittent, nonphysiological stimulation of striatal dopamine receptors destabilizes an already unstable system. Accordingly, a major goal of PD treatment in recent years has been the attainment of continuous dopaminergic stimulation (CDS)—or, less theoretically (and more clinically verifiable), continuous drug delivery (CDD). Improvements in the steadiness of the plasma profiles of various dopaminergic therapies may be a signal of progress. However, improvements in plasma profile do not necessarily translate into CDS, or even into CDD to the brain. Still, it is reassuring that clinical studies of approaches to CDD have generally been positive. Head-to-head comparative trials have often failed to uncover evidence favoring such approaches over an intermittent therapy. Nevertheless, the findings among recipients of subcutaneous apomorphine infusion or intrajejunal levodopa/carbidopa intestinal gel suggest that nonmotor PD symptoms or complications may improve in tandem with motor improvement. In vivo receptor binding studies may help to determine the degree of CDS that a dopaminergic therapy can confer. This may be a necessary first step toward establishing whether CDS is, in fact, an important determinant of clinical efficacy. Certainly, the complexities of optimal PD management, and the rationale for an underlying strategy such as CDS or CDD, have not yet been thoroughly elucidated.
Keywords: Parkinson’s disease, Motor complications, Nonmotor fluctuations, Continuous drug delivery
Introduction
In patients with Parkinson’s disease (PD), both motor and nonmotor complications are common, burdensome sequelae of long-term levodopa treatment. The motor complications are well recognized. In broad terms, they consist of motor fluctuations and dyskinesias, although within each of these categories varied patterns have been described (Olanow et al. 2009). By some estimates, more than 50 % of PD patients report one or another such problem after 5 years of levodopa use; and after 10 years, up to 80 % of patients report them (Obeso et al. 2000). Their impact can be substantial, reducing the patient’s mobility and the ability to perform activities of daily living (ADL). In addition, emotional well-being and health-related quality of life (HRQoL) can be severely impaired (Chapuis et al. 2005; Damiano et al. 2000).
The nonmotor complications are fluctuations resulting in symptoms such as mood disturbance, cognitive dysfunction, dysautonomia, and pain (Witjas et al. 2002). Considered together (Chaudhuri et al. 2011), they may be at least as common as motor complications (Gunal et al. 2002), but they appear to be under-reported (Chaudhuri et al. 2010). In a survey of PD patients with motor fluctuations (Witjas et al. 2002), 100 % of participants reported nonmotor fluctuations, which 28 % rated as being more disabling than the motor problems. Anxiety, excessive sweating, slowed cognition, fatigue, and akathisia were the most frequent nonmotor fluctuations reported. The burdens imposed by such fluctuations are hard to differentiate from those imposed by PD itself. Still, in a recent large-scale study of the overall nonmotor burden (Martinez-Martin et al. 2011), total score on the nonmotor symptoms scale (NMSS) (Martinez-Martin et al. 2009) showed a high correlation with HRQoL (r = 0.70), as measured by the 39-item PD questionnaire (PDQ-39) (Jenkinson et al. 1997a). Remarkably, the correlation exceeded that for motor dysfunction (r = 0.58), as measured by scales for outcomes in PD (SCOPA) motor score (Martínez-Martín et al. 2005).
Numerous studies have investigated the predictors and potential pathophysiologic mechanisms of levodopa complications in PD patients, in hope of developing clinical strategies to avoid them. For motor complications, especially dyskinesia, the reported risk factors include higher dosage and longer duration of levodopa treatment, longer duration and severity of a patient’s PD, and younger age at PD onset (Grandas et al. 1999). Although nonmotor PD manifestations may be related to nondopaminergic brain changes concomitant with or secondary to the striatal dopaminergic deafferentation considered to be a PD hallmark (Simuni and Sethi 2008), at least some nonmotor fluctuations (e.g., in autonomic function) have likewise been associated with higher dosage and longer duration of levodopa treatment and with younger age at PD onset (Chaudhuri and Schapira 2009; Gunal et al. 2002). In a survey of patients with motor fluctuations, all 50 subjects reported nonmotor fluctuations, most of which occurred in the patients’ “OFF” state, thereby exhibiting correlation with their motor dysfunction (and with time spans of levodopa inefficacy) (Witjas et al. 2002). However, nonmotor fluctuations of all types (e.g., autonomic, cognitive/psychiatric, or sensory) are also seen during “ON” time (Gunal et al. 2002).
Extensive preclinical research, e.g., in primate PD models (Jenner 2009), has been advancing the hypothesis that the motor complications of chronic levodopa therapy may derive from the therapy’s intermittent, nonphysiological stimulation of the parkinsonian brain’s striatal dopamine receptors (Chase et al. 1989; Grace 2008; Jenner 2008; Nutt et al. 2000; Olanow et al. 2006). On this basis, a major goal of PD treatment in recent years has been the attainment of continuous dopaminergic stimulation (CDS)—or, less theoretically (and more clinically verifiable), continuous drug delivery (CDD). Pharmacologically, CDD has been attempted by strategies including a variety of levodopa formulations and delivery methods, as well as by dopamine agonists with differing pharmacokinetic properties and receptor-affinity profiles. This review will survey the key therapeutic advances.
Defining the complications
Among the complications of chronic levodopa therapy in PD, motor fluctuations (Olanow et al. 2009) are defined as alterations between periods of clinical response of motor symptoms to levodopa, during which the patient’s mobility and motor function are relatively good (i.e., during “ON” time), and periods when motor response deteriorates (“OFF” time). In early PD, such oscillations are not expected to occur. At this stage of the disease, the motor response to a single levodopa dose is typically long-lasting (>4 h), despite the drug’s plasma half-life of only 60–90 min, yielding a span of “ON” time sufficient to bridge the interval between successive doses throughout the patient’s waking day. Indeed, response is often stable even if one or more doses are missed (“long-duration response”). With advancing PD, however, the duration of motor-symptom control conferred by a levodopa dose progressively shortens toward an approximate matching of the drug’s plasma half-life (“short-duration response”). Patients may then begin to experience a predictable “wearing-off” effect. Patients may also have rapid, unpredictable fluctuations between “ON” and “OFF” states (“ON–OFF phenomenon”) (Marsden and Parkes 1976), and some doses may take longer to become effective (“delayed-ON”) or may not be effective at all (“no-ON”) (Obeso et al. 2008). Although it has been hypothesized that motor fluctuations might arise in advanced PD because loss of dopaminergic presynaptic terminals may decrease striatal capacity to store dopamine, “wearing-off” has also been seen in PD treated with apomorphine and other dopamine agonists not stored in dopaminergic terminals (Bravi et al. 1994). The implication is that the pathophysiology of motor fluctuations must have postsynaptic facets (Verhagen Metman et al. 1997).
Dyskinesias in PD patients reliant on chronic levodopa (Olanow et al. 2009) are involuntary movements most typically coinciding with maximum levodopa plasma level and maximum motor-symptom response (“peak-dose dyskinesia”). In such patients, the dyskinesia is typically choreiform, involving any part of the body, but may be dystonic or myoclonic. Dyskinesia can also occur when an “ON” state begins and again as it ends (“diphasic dyskinesia”). In such patients, the abnormal movements tend to be rhythmic, stereotypic, and asymmetric, and to affect the legs. In either case, the dyskinesia has long been viewed as the expression of a disruption of the normal ability of the basal ganglia to select and execute motor programs (Marsden 1982).
With increasing appreciation of the complexity of the dopaminergic influence on basal ganglia function, there has come a more specific suspicion that dyskinesia may be the eventual outcome of a fundamental inadequacy of standard levodopa as an exogenous replacement for endogenous dopamine, namely the treatment’s abnormally pulsatile stimulation of striatal dopamine receptors (Jenner 2008; Olanow and Obeso 2000). The physiologic stimulation of these receptors appears to be a tonic process with phasic fine-tuning (Goto et al. 2007; Schultz 1994), requiring that the striatum maintain a steady baseline supply of endogenous dopamine (Venton et al. 2003). Hence, the institution of abnormally pulsatile stimulation is thought to lead to dysregulation of genes and proteins in striatal neurons, in turn, producing an enduring alteration of firing patterns in basal ganglia output neurons (Jenner 2008; Olanow and Obeso 2000). In brief, the intermittency of standard levodopa therapy does not achieve the desired normalization of the parkinsonian basal ganglia but instead destabilizes the already unstable system (Olanow et al. 2009). Indeed, in PD models such as the primate models induced by the dopamine-neuron-specific neurotoxin 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), intermittent administration of short-acting dopaminergic agents (e.g., levodopa) has been found notably apt to induce dyskinesia (Pearce et al. 1998); yet even the short-acting agents have been found not to do so if they are given continuously (Bibbiani et al. 2005).
The nonmotor fluctuations seen during long-term levodopa usage in PD have been categorized as dysautonomic, cognitive/psychiatric, and sensory (Witjas et al. 2007). Although their causes remain obscure, dopaminergic dysfunction would appear to be involved, acting either directly or through the unbalancing effects of dopaminergic dysfunction on other neurotransmitter systems (Witjas et al. 2007). As a possible example of a direct link, neuroimaging data have identified dopaminergic dysfunction (reduced receptor availability) in the hypothalamus of the parkinsonian brain (Politis et al. 2008), an abnormality conceivably influencing dysautonomia. As a possible example of an indirect link, neuroanatomic and neurophysiologic data have combined in suggesting that in the normal brain, dopaminergic and serotonergic systems interact via reciprocal connections between the substantia nigra (and ventral tegmental area) and the brainstem raphé nuclei (Di Giovanni et al. 2008), conceivably affecting sleep homeostasis. For either direct or indirect linkage of dopaminergic dysfunction to nonmotor fluctuations, the fluctuations might be responsive to CDD. However, it may be instructive that in advanced PD, deep brain stimulation of the subthalamic nucleus appears to best alleviate nonmotor fluctuations affecting sensory, autonomic, and cognitive function, while neuropsychiatric fluctuations respond less consistently (Witjas et al. 2007).
The evolution of CDD strategies
Because of a number of pharmacokinetic factors, intermittent oral dosing of levodopa does not provide stable plasma drug levels. The most significant problems are the short half-life of levodopa (~60 min) (Deleu et al. 2002) and the pulsatile and unpredictable absorption of levodopa from the small intestine due to erratic gastric emptying (Kurlan et al. 1988; Nyholm et al. 2003). As efforts to improve the agent’s solubility so as to enhance its absorption, levodopa has been studied as an orally administered liquid or methyl ester (Antonini et al. 2010a). Brain levodopa levels also vary owing to competition of levodopa with amino acids for transport across the intestinal wall and the blood–brain barrier (Frankel et al. 1989), but these perturbations are relatively minor and in most patients appear not to have a clinically relevant impact (Nutt et al. 1989).
Efforts to achieve a steady level of levodopa, or of dopaminergic PD therapies in general, began almost at the inception of the treatments themselves (Tolosa et al. 1998). Inhibition of levodopa metabolism was first attempted in the 1960s, using the peripheral dopa decarboxylase inhibitor (DDI) benserazide or subsequently, carbidopa. Then, in the early 1970s, a sustained-release oral formulation of levodopa was developed. Dopamine-receptor agonist therapies were tested as early as 1951 but did not become an option in routine PD treatment until the 1970s, when an oral formulation of bromocriptine was introduced. Continuous infusion of a dopaminergic therapy was first attempted in the mid 1970s, using intravenous delivery. All of these broad strategies continue to be developed.
Oral levodopa in combination with metabolic inhibitors
Dopamine does not cross the blood–brain barrier. By contrast, levodopa does cross the barrier, provided that it has not been converted to dopamine in the periphery. Within the central nervous system (CNS), dopaminergic neurons can perform this conversion. In view of these circumstances, the CNS bioavailability of levodopa, and of dopamine as its desired CNS metabolite, can be enhanced by a number of strategies (Deleu et al. 2002): (1) blocking the peripheral conversion of levodopa into dopamine or another metabolite, (2) blocking the central metabolism of levodopa along pathways that do not produce dopamine, and (3) blocking the central metabolism of dopamine.
Dopa decarboxylase inhibitors, such as carbidopa or benserazide, are given to implement the first of these strategies, i.e., they block the peripheral conversion of levodopa into dopamine, allowing a larger influx of levodopa into the brain. By doing so, they permit reduction of total daily levodopa dosage (Cedarbaum 1987). They also reduce levodopa side effects arising from peripheral dopamine-receptor stimulation (e.g., nausea and vomiting) (Kaakkola et al. 1985; Markham et al. 1974). Pharmacokinetically, they increase the peak plasma levodopa concentration (C max), increase overall levodopa exposure [area under the concentration–time curve (AUC)], and prolong levodopa plasma half-life (Cedarbaum 1987; Robertson et al. 1989). In clinical practice, levodopa is invariably combined with carbidopa or benserazide, regardless of other strategies that may also be employed to enhance levodopa availability.
Catechol-O-methyltransferase (COMT) inhibitors implement the first and perhaps also the second and third strategy, depending on whether the drug can enter the brain. Via COMT inhibition, each such drug blocks the conversion of levodopa into 3-O-methyldopa or 4-O-methyldopa and also of dopamine to 3-methoxytyramine (Deleu et al. 2002). However, entacapone acts only in the periphery, while tolcapone may have some central effect. On the other hand, tolcapone is associated with liver toxicity and is recommended only for motor complications not responsive to other levodopa adjuncts (and even then only with regular monitoring of liver function) (Tasmar® 2009). Pharmacokinetically, single-dose entacapone has been found to increase the AUC and prolong the plasma half-life of levodopa administered as an immediate-release (IR) formulation, without affecting levodopa C max (Nutt 1996, 2000). With repeated entacapone dosing, both peaks and troughs in levodopa plasma level become higher, with diminished difference between them (Fig. 1) (Nutt 1996). This leveling, however, is not as pronounced as may be achieved by levodopa administered as a controlled-release (CR) formulation (LeWitt et al. 2009). Pharmacokinetic-pharmacodynamic studies (Merello et al. 1994; Piccini et al. 2000; Ruottinen and Rinne 1996a, b) have shown that an increase in the AUC of levodopa administered with entacapone is temporally associated with improved motor function. This benefit, however, may be achieved at a cost of increased dyskinesia (Stocchi et al. 2010).
Fig. 1.
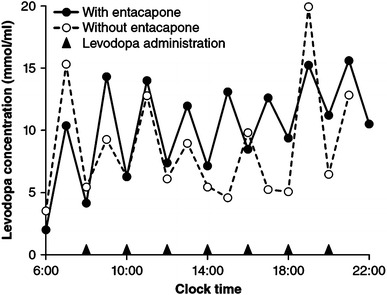
Plasma levels of immediate-release oral levodopa with versus without entacapone in a PD patient receiving treatment (arrowheads) every 2 h (data adapted from Nutt 1996)
Monoamine oxidase (MAO) inhibitors implement the third strategy: i.e., they block the conversion of CNS dopamine into 3,4-dihydroxyphenylacetic acid (Deleu et al. 2002). Of the two known MAO isoforms, MAO-A predominates in the intestinal tract while MAO-B is prominent in brain areas including the basal ganglia (Youdim and Bakhle 2006). Two drugs, rasagiline and selegiline (Azilect® 2009; Eldepryl® 2011), are currently marketed as irreversible MAO-B-selective inhibitors. Both are approved as adjunctive therapy to levodopa, and rasagiline is also approved as monotherapy in early PD. In general, MAO-B inhibitors improve “ON” time only modestly (Rascol et al. 2005), suggesting that patients may continue to experience motor and nonmotor fluctuations.
Controlled-release levodopa
Slow-release formulations of orally administered levodopa are available only in combination with a DDI (carbidopa in the United States and benserazide or carbidopa in the European Union). Madopar® HBS (hydrodynamically balanced system; Roche Products, Ltd, Hertfordshire, UK) combines levodopa and benserazide in a capsule that forms a mucoid body, which in turn remains in the stomach for a prolonged period, allowing slow diffusion of its contents (Erni and Held 1987). Sinemet® CR (Merck & Co., Inc., Whitehouse Station, NJ; Bristol-Myers Squibb Company, Princeton, NJ) combines levodopa and carbidopa in a monolithic-matrix tablet that releases the drugs gastrointestinally, via surface dissolution and erosion (Dempski et al. 1989; Wilding et al. 1991). In general, slow-release formulations may permit a decrease in dosing frequency and may reduce the temporal variability in levodopa plasma level (Fig. 2a), compared with levodopa in its standard IR form (Cedarbaum et al. 1989; Pahwa et al. 1997). Moreover, pharmacodynamic studies in advanced PD have reported clinical benefits (Fig. 2b), including an increase in “ON” time (Cedarbaum et al. 1989; Pahwa et al. 1997). However, slow-release formulations also delay the levodopa plasma C max (~2 h vs. 30–45 min for IR formulations) and may exhibit a lower level at the maximum, necessitating an increase in total daily levodopa dosage (Pahwa et al. 1997; Sage and Mark 1994). A major problem is that erratic pharmacokinetics may result in unpredictable clinical response. Moreover, patients on slow-release formulations often require a morning dose of an IR formulation. A new oral levodopa–carbidopa formulation combining the pharmacokinetics of IR and CR formulations has shown promise in clinical trials (Hauser 2012) and awaits FDA approval.
Fig. 2.
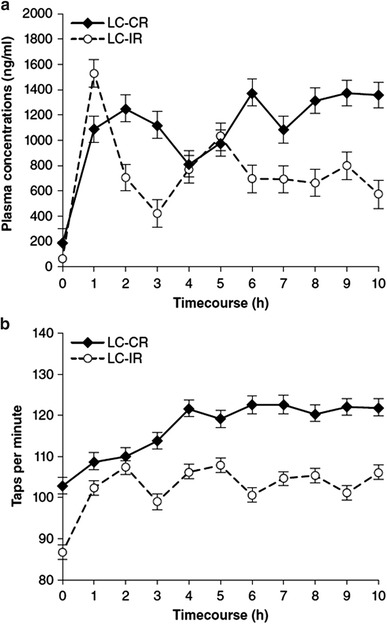
Plasma levels (a) and motor-function (tapping total) profiles (b) for slow- versus immediate-release oral levodopa/carbidopa in 18 PD patients with motor fluctuations (data adapted from Pahwa et al. 1997). LC-CR (slow) controlled-release levodopa/carbidopa, LC-IR immediate-release levodopa/carbidopa
Dopamine-receptor agonists
Dopamine-receptor agonists are indicated as monotherapy in early PD and as adjunctive therapy to levodopa at all stages of PD. Despite the gold-standard status of levodopa for controlling motor symptoms, the agonists have potential advantages, including the pharmacokinetic advantage of their longer half-lives (Kvernmo et al. 2006). In addition, dopamine-receptor agonists exhibit selectivity in their binding to dopamine receptors, conceivably permitting a reduction in the expression of dyskinesias, e.g., by use of agonists selective for D2-like receptors (Jenner 2008). Several first-generation agonists (e.g., pergolide, cabergoline, and bromocriptine) are ergotamine derivatives associated with fibrotic heart disease (Zanettini et al. 2007) perhaps related to 5-HT(2B) serotonin-receptor agonism (Antonini and Poewe 2007). In consequence, pergolide has been withdrawn from the US market; and in the European Union, the first-generation agents are now restricted to second-line use (of pergolide and cabergoline) or now carry warning labels. Despite being ergoline, lisuride lacks 5-HT(2B) agonism and is not known to cause cardiac valvular fibrosis (Hofmann et al. 2006). Lisuride has been formulated for transdermal delivery from a skin patch (which, however, is not widely used, owing to neuropsychiatric complications).
Ropinirole and pramipexole are second-generation, nonergoline, D2-like-receptor preferring agonists widely prescribed for oral administration in PD. In their IR forms, the half-life of ropinirole is ~6 h and that of pramipexole is 8–12 h (Kvernmo et al. 2006). Both drugs are also available as slow-release formulations. Prolonged-release (PR) ropinirole is a tablet based on matrix technology. Compared with the IR formulation given three times daily (Tompson and Vearer 2007), its once-daily dosing provided a similar dose-normalized AUC0–24 h, a C max 12 % lower, and a median t max of approximately 6 versus 2 h for the IR formulation (Fig. 3a). In a double-blind study in early PD (Stocchi et al. 2008), it exhibited noninferiority to ropinirole IR, as judged by unified Parkinson’s disease rating scale (UPDRS) (Fahn et al. 1987) motor score. Extended-release (ER) pramipexole is also a matrix tablet. At steady-state for once-daily dosing (Jenner et al. 2009b), its C max and AUC0–24 h resembled those of the IR formulation given three times daily, but the geometric mean t max was more than 5 h versus approximately 1 h for the IR formulation (Fig. 3b). In a double-blind study in early PD (Hauser et al. 2010), improvements in UPDRS motor plus ADL scores resembled those for the IR formulation.
Fig. 3.
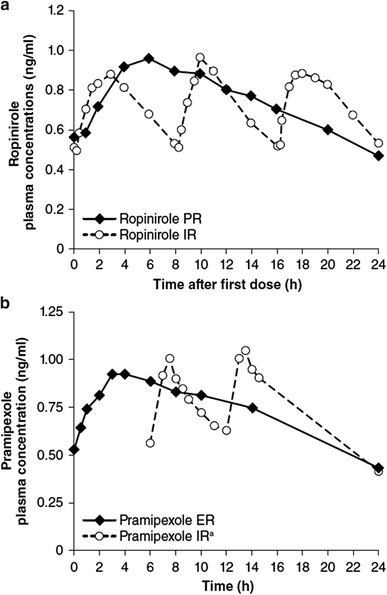
Plasma levels for PR (a)/ER (b) versus IR formulations of oral dopamine agonists: Ropinirole (a) in 20 patients with early PD (data adapted from Tompson and Vearer 2007), and pramipexole (b) in 14 healthy volunteers (data adapted from Jenner et al. 2009). ER extended-release, IR immediate-release, PR prolonged-release. aOnly the last two doses are graphed for pramipexole IR
Rotigotine is a nonergoline dopamine agonist selective for D2-like receptors, but also showing affinity for D1-like receptors (Scheller et al. 2009). Formulated for transdermal delivery from skin patches each to be worn for 1 day (Cawello et al. 2007, 2009; Pfieffer 2005), its availability has been impeded by problems with crystallization. Nevertheless, a recent large-scale study (Trenkwalder et al. 2011a) in patients selected for having unsatisfactory early morning motor-symptom control at any PD stage, with or without levodopa, constitutes the first double-blind, placebo-controlled investigation of the effects of a CDD strategy on both motor and nonmotor deficits. At 12 weeks, mean early morning motor dysfunction, mean sleep disturbance, and depressive symptomatology [as measured by UPDRS (Fahn et al. 1987), the PD sleep scale (PDSS) (Trenkwalder et al. 2011b), and the Beck depression inventory (BDI) (Visser et al. 2006), respectively] showed significantly greater improvements in the active-treatment group. Rotigotine has been re-introduced in the US market as a new formulation that may be more stable than the original.
Impulse control disorders such as compulsive gambling, shopping, or hypersexuality are being increasingly recognized in PD patients as adverse effects of dopamine agonist therapy (Weintraub and Nirenberg 2013). The degree of risk associated with long-acting dopamine agonists or infusional dopaminergic therapies is currently under investigation. A recent post-marketing survey conducted in Europe has suggested that the risk may be lower for the rotigotine patch and for pramipexole ER than for shorter-acting agonists (Rizos et al. 2012).
Continuous drug infusion
Apomorphine and levodopa/carbidopa intestinal gel (LCIG) are the two dopaminergic therapies currently available as a continuous infusion for patients with severe motor fluctuations in advanced PD. Typically, each is administered during waking hours only. (A third therapy, lisuride infusion, is not widely used.)
Apomorphine (Apokyn® (2012) is a nonergoline dopamine-receptor agonist with less receptor selectivity than that of other available agonists, although it does demonstrate some D2-receptor preference (Deleu et al. 2004). After subcutaneous injection, it is notably short-acting: in one study, its elimination half-life was 33 min (Gancher et al. 1989). A portable pump permits its continuous infusion into subcutaneous fatty tissue of the abdomen, thighs, or arms (LeWitt 2004); a delivery method available in Europe. After long-term usage, however, inflammatory skin nodules may form and may interfere with drug absorption (Nicolle et al. 1993). In a small study of PD patients switched from subcutaneous to intravenous apomorphine (delivered by indwelling venous catheter) for refractory motor fluctuations (Manson et al. 2001), dyskinesia showed substantial decrease, and “OFF” time was reported to be virtually eliminated (a mean reduction from 5.4 to 0.5 h; p < 0.05), although plasma apomorphine levels did not correlate well with dosage level or with motor function (Fig. 4a–d), and complication rates were high. In another small study, of two PD patients, plasma apomorphine levels likewise showed weak correlation with motor function, but for cerebrospinal-fluid apomorphine levels, the correlation with motor function was strong (Hofstee et al. 1994).
Fig. 4.
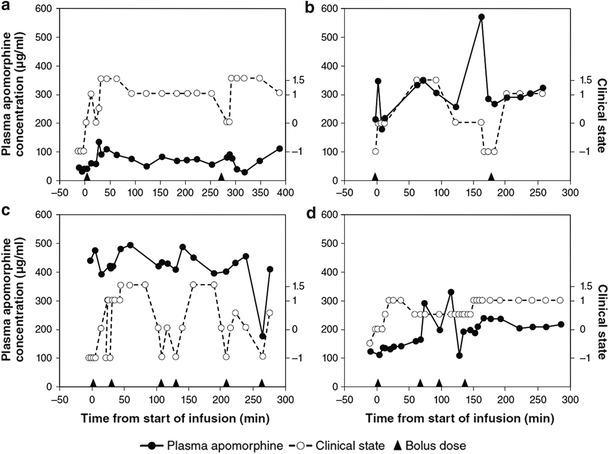
Plasma apomorphine levels (left y-axis scale) and simultaneous clinical-state scores (right y-axis scale) for each of four recipients of continuous subcutaneous apomorphine infusion. Arrowheads on x-axis mark bolus doses. Clinical state was a global objective/subjective rating in half-point increments, including ratings of −1 for fully “OFF”, 0 for threshold of “ON”, +1 for fully “ON”, and +1.5 for dyskinesia or subjectively overdosed (e.g., light-headed, confused) (data adapted from Manson et al. 2001)
Levodopa/carbidopa intestinal gel (Duodopa®; Abbott, Abbott Park, IL) is a methylcellulose gel suspension of levodopa/carbidopa formulated for continuous enteral infusion from a portable pump and medication cassette worn attached to the waist or over the shoulder (Nyholm et al. 2003). To complete the delivery system, jejunal or duodenal tubing is emplaced by a percutaneous endoscopic gastrostomy procedure. In a small crossover trial (Nyholm et al. 2003) comparing nasoduodenal LCIG infusion with optimized sustained-release oral levodopa/carbidopa, the mean steady-state plasma levodopa concentration was the same for both the treatments, but the mean C max was lower for LCIG (Fig. 5a, b); and on motor tasks performed at hourly intervals, a higher proportion of observations were considered near-normal [at 80 % for LCIG versus 61 % levodopa/carbidopa CR; estimated mean difference, 19%; 95 % confidence interval (CI): 12, 26 %; p < 0.01]. LCIG is currently available in Europe, Canada, and Australia and is under investigation in the United States.
Fig. 5.
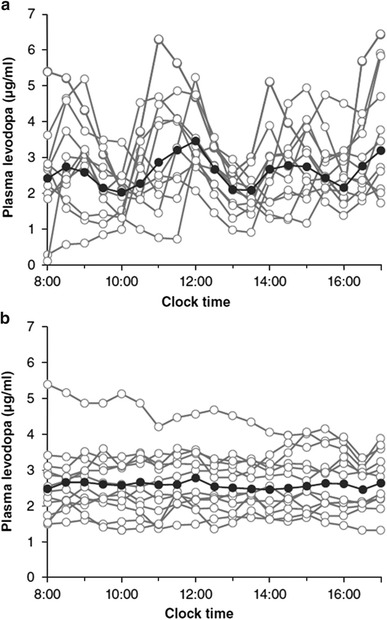
Plasma levodopa levels for sustained- (slow-) release oral levodopa/carbidopa (a) versus continuous intraduodenal infusion of LCIG (b) in each of 12 patients with advanced PD. In each graph, the solid black curve with solid black circles for its data points displays the mean for all curves (data adapted from Nyholm et al. 2003)
Clinical correlates of CDD
For dopaminergic therapies formulated and/or delivered in efforts to approach or attain CDD, numerous studies have evaluated the impact on motor fluctuations and dyskinesia. Both acute effects and the ability to delay the onset of such complications have been assessed. The impact on nonmotor function has not yet been evaluated extensively.
Prevention of motor complications in early PD
The most recent practice guidelines for treating early PD are those of a consensus document published jointly in 2006 by the European Federation of Neurological Societies (EFNS) and the Movement Disorder Society (MDS) European Section (Horstink et al. 2006). Based on available evidence, this panel judged ropinirole and pramipexole, in their IR formulations, to be effective as monotherapy both for motor-symptom control and for prevention of levodopa-associated motor complications, especially among younger patients, in whom such complications are thought to be more likely. For other dopaminergic therapies, data either were lacking, as in the case of COMT inhibitors and the MAO-B inhibitor rasagiline, or did not support efficacy for motor-complication prevention, as in the case of levodopa CR and the MAO-B inhibitor selegiline.
Since then, long-term (6-year) data from the CALM-PD study of levodopa versus pramipexole IR as initial PD pharmacotherapy have found dopaminergic motor complications (encompassing “wearing-off”, “ON–OFF” effects, or dyskinesias) to be more likely for levodopa than for the dopamine agonist (Parkinson Study Group CALM Cohort Investigators 2009). However, disabling dyskinesias were uncommon in both treatment groups. Long-term (6.5-year) data from an open-label extension (Hauser et al. 2009a) of the TEMPO study (Parkinson Study Group 2004) of early- versus delayed-start rasagiline have failed to demonstrate a difference in the median time to development of motor complications (or time to addition of levodopa) in patients who started receiving rasagiline 6 months earlier in their PD than did the delayed-start group. Data have also been reported concerning the efficacy of COMT inhibitors in early PD. In the 39-week, double-blind FIRST-STEP study (Hauser et al. 2009b), the incidence of “wearing-off” and dyskinesia did not differentiate between groups receiving levodopa/carbidopa/entacapone (LCE) or only levodopa/carbidopa three times daily, despite the superiority of LCE on efficacy measures including the study’s primary outcome, the sum of motor and ADL scores in the UPDRS (but not on measures including the motor score alone). STRIDE-PD (Stocchi et al. 2010), a large-scale, double-blind study designed specifically to evaluate the capacity of LCE to delay dyskinesia, has also failed to find such benefit. For treatment lasting up to 208 weeks, the risk of dyskinesia was actually higher in the study’s LCE group than in its levodopa/carbidopa group. Although the mean dosage of levodopa was highly similar across these groups, the estimated bioavailability of levodopa was significantly heightened by the entacapone in LCE, conceivably hastening dyskinesia (p < 0.001). The investigators also hypothesized that the study’s four-times-daily dosing of LCE (at 3.5-h intervals) might not have achieved CDS.
Two recent meta-analyses (Baker et al. 2009; Stowe et al. 2008) support the 2006 EFNS/MDS recommendations on dopamine agonists for prevention of motor complications. For oral IR dopamine-agonist treatment compared with levodopa, one study (Stowe et al. 2008) reported an odds ratio (OR) of 0.51 (95 % CI: 0.43, 0.59; p < 0.00001) for risk of dyskinesia and 0.75 (95 % CI: 0.63, 0.90; p = 0.002) for risk of motor fluctuations. In the other study (Baker et al. 2009),while the UPDRS motor scores demonstrated that patients receiving dopamine agonists had a significantly inferior response compared with patients receiving levodopa, based on a >4-point higher ADL score (weighted mean difference, 4.69; 95 % CI: 3.76, 5.61; p < 0.0001), the ORs for risk of dyskinesia and “wearing off” were 0.36 (95 % CI: 0.22, 0.60; p < 0.0001) and 0.52 (95 % CI: 0.40, 0.66; p < 0.0001), respectively. Both meta-analyses found that dopamine agonists conferred an increased risk for somnolence, dizziness, nausea, and hallucinations. In a recent double-blind study of adding ropinirole PR in levodopa-treated patients with early PD (Watts et al. 2010), onset of dyskinesia was significantly delayed in the ropinirole PR group compared with a group receiving additional levodopa (hazard ratio, 6.46; p < 0.001). In a head-to-head comparison between transdermal rotigotine and oral ropinirole IR in early PD (Giladi et al. 2007), the patch failed to demonstrate noninferiority on UPDRS motor plus ADL scores. Differences in rates of motor complications were not assessed.
Treatment of motor complications in advanced PD
In a literature review published in 2006 (Pahwa et al. 2006), a subcommittee of the American Academy of Neurology (AAN) concluded that entacapone and rasagiline had established their efficacy, and that pramipexole, ropinirole, and tolcapone were “probably” effective, for reducing “OFF” time in PD patients with motor fluctuations. For “OFF” time reduction, levodopa/carbidopa CR was not considered to be more effective than the IR formulation. Continuous-infusion therapies (i.e., apomorphine or LCIG) were not included in the analyses.
More recent meta-analyses of treatments adjunctive to levodopa in advanced PD have confirmed the capacities of oral IR dopamine agonists, COMT inhibitors, and MAO-B inhibitors to reduce “OFF” time and UPDRS scores. For all three drug classes, the improvements were at the expense of an increase in dyskinesia, compared with placebo (Stowe et al. 2010; Talati et al. 2009). By indirect comparisons of the three classes, IR dopamine agonists appeared to be the most effective for reducing “OFF” time (at −1.54 h/day vs. −0.83 for COMT inhibitors and −0.93 for MAO-B inhibitors), but the agonists (and the COMT inhibitors) carried a higher risk for dyskinesias than did the MAO-B inhibitors (Stowe et al. 2010).
In recent studies with placebo control (Pahwa et al. 2007; Schapira et al. 2011), slow-release oral formulations of ropinirole and pramipexole, taken adjunctive to levodopa, have also shown efficacy for reducing “OFF” time and UPDRS scores. For both agents, “ON” time without troublesome dyskinesia was significantly increased. However, the incidence of dyskinesia as an adverse event was higher (at 13 % for ropinirole PR vs. 3 % for placebo; and at 17 % for pramipexole ER vs. 8 % for placebo, a difference not tested statistically in either trial). In a recent 24-week study comparing ropinirole formulations (Stocchi et al. 2011), the slow-release form had a response rate (defined by ≥20 % reduction in “OFF” time; adjusted OR, 1.82; 95 % CI: 1.16, 2.86; p = 0.009) and a capacity to reduce UPDRS motor scores (adjusted mean change from baseline for ropinirole PR vs IR, −10.2 vs. −7.9, respectively; p = 0.022) significantly greater than those for the IR form. The incidence of adverse events was numerically higher among recipients of the slow-release form (who also reached higher agonist dosage, but lower levodopa dosage, than in the IR arm). In an analogous comparison (Schapira et al. 2011), pramipexole ER showed capacities to reduce “OFF” time and UPDRS motor plus ADL scores resembling those of pramipexole IR. The incidence of adverse events was numerically lower for the ER form (at similar agonist dosage and lower levodopa dosage than in the IR arm).
In each of two studies with placebo control (LeWitt et al. 2007; Poewe et al. 2007), transdermal rotigotine, adjunctive to levodopa, has shown efficacy for motor complications in advanced PD, as evidenced by significant reductions in “OFF” time (p ≤ 0.0031) and increases in “ON” time without troublesome dyskinesia (p ≤ 0.0078). Incidence rates for dyskinesia as an adverse event were higher for rotigotine than for placebo (but were not tested statistically). In one of these studies (Poewe et al. 2007), a third treatment arm permitted head-to-head comparisons between the rotigotine patch and pramipexole IR. Improvements in “OFF” time, “ON” time without troublesome dyskinesias, and other outcomes showed no significant differences between these two treatments.
No double-blind studies have yet been reported for chronic treatment with apomorphine. However, in 2004 a review of 11 long-term, uncontrolled, open-label studies of subcutaneous apomorphine infusion (Deleu et al. 2004) reported a 60 % mean reduction in “OFF” time (range 50–80 % across studies) and also improvement in dyskinesia, which, however, required a mean of 12 months (range 0.5–50 months) to reach its maximum. Two further studies of subcutaneous apomorphine infusion have since been reported. In a prospective study (Katzenschlager et al. 2005), 12 patients with motor fluctuations and disabling dyskinesias received apomorphine infusion for 6 months. “OFF” time was reduced from baseline by 38 % (p < 0.05) and dyskinesia duration by 40 % (p < 0.01). In four of the 12 patients, oral medication could be discontinued, and within this apomorphine monotherapy group, there was a significantly greater decrease in “OFF” time and dyskinesia severity and duration than in the polytherapy group (for “OFF” time, 64 vs. 18 %, respectively, p < 0.05; for dyskinesia severity and duration expressed as centimeters on a visual analogue scale, 8.6 vs. 19.8, respectively, p < 0.05). Skin nodules were reported in 11 of 12 patients, including two patients with skin changes and inflammatory reactions requiring rotation of the infusion site. A retrospective analysis (García-Ruiz et al. 2008) of 82 patients who tolerated subcutaneous apomorphine infusion for at least 3 months (mean, 20 months) also identified significant decreases from baseline in “OFF” time (mean baseline vs. last follow-up visit, 6.64 vs. 1.36 h/waking day, p < 0.0001) and dyskinesia severity score (1.65 vs. 1.15, respectively, p < 0.0006). In this study, 68 % of patients reported treatment-related skin nodules.
For LCIG, findings of a double-blind, double-dummy trial comparing intrajejunal gel infusion and oral administration of levodopa-carbidopa in IR form have now been presented. For 12 weeks, PD patients selected for having motor complications underwent active LCIG infusion and took placebo IR capsules or took active IR capsules and underwent placebo gel infusion (Olanow et al. 2011). Among 66 study completers (93 % of the 71 randomized subjects), decrease in “OFF” time and increase in “ON” time without troublesome dyskinesia favored LCIG by means of −1.91 and +1.86 h/d, respectively, while “ON” time with troublesome dyskinesia showed no significant change (Olanow et al. 2012). Significant global, functional (ADL), and quality-of-life LCIG benefits were also identified (Kieburtz et al. 2012).
Several previous, open-label studies had already evaluated LCIG during chronic treatment lasting up to 7 years (Table 1) (Antonini et al. 2007, 2008, 2010b; Eggert et al. 2008; Isacson et al. 2008; Nilsson et al. 2001). Although variations in trial design preclude any summarization of the numerical findings, measures of “OFF” time improved in all six studies, with significance achieved in all five studies in which statistical testing was performed; dyskinesia measures also improved in all six studies, with statistical significance in four of the five studies with statistical testing. In addition, a randomized crossover trial (Nyholm et al. 2005) has compared 3 weeks of individually optimized conventional treatment with 3 weeks of nasoduodenal LCIG infusion. The conventional treatment was oral levodopa/carbidopa in optional combinations with oral dopamine agonists, COMT-inhibitors, MAO-B inhibitors, amantadine, or subcutaneous apomorphine (by injections or infusion). Motor tasks were videotaped every 30 min for 8 h on 2 days during the second and third week of each treatment for rating of motor function by neurologists blinded to treatment identity. (To blind the conventional therapies, a dummy nasogastric tube was emplaced.) Of 24 enrolled patients, 20 completed conventional therapy and 21 completed LCIG. The mean percentage of ratings falling within the predefined range for a clinically desirable “ON” state was significantly greater during LCIG than during conventional therapy (at 90.7 vs. 74.5 %, respectively, p < 0.01), and the mean percentage of ratings of “OFF” state was significantly lower (at 1.8 vs. 19.2 %, respectively, p < 0.01). For ratings of “ON” with moderate-to-severe dyskinesia, LCIG and conventional therapy showed no significant difference. Of the four patients who received subcutaneous apomorphine infusion as part of their conventional therapy, two were rated as being in an “ON” state all or nearly all of the time on both conventional treatment and LCIG, but the other two had substantial improvements on LCIG. In one patient, the proportion of “ON” ratings improved from 56 to 94 %, and in the other from 68 to 100 %.
Table 1.
“OFF” time and dyskinesia outcomes in prospective studies of long-term LCIG therapy
| Study | N enrolled/n completed | Maximum duration | Outcome versus conventional treatment |
|---|---|---|---|
| Nilsson et al. (2001) | 9/6a | 7 years | “OFF” time duration decreased at 3–8 months and at 4–7 yearsb. Dyskinesia duration decreased at 3–8 months and further decreased at 4–7 years |
| Antonini et al. (2007) | 9/7 | 1 year | “OFF” time and disabling-dyskinesia duration significantly decreased |
| Antonini et al. (2008) | 22/17 | 2 years | “OFF”-time duration and severity (by UPDRS part IV) significantly decreased |
| Eggert et al. (2008) | 13/11 | 6 monthsc | “OFF” time and “ON” time with disabling dyskinesia significantly reduced as percent of patient’s day |
| Isacson et al. (2008)d | 14/12 | 6 months | Proportion of patients with reduced “OFF” time significantly greater; proportion with reduced dyskinesia numerically greater |
| Antonini et al. (2010b) | 15/4 | 3 years | “OFF” time duration and dyskinesia severity (by UPDRS part IV) significantly decreased |
LCIG levodopa/carbidopa intestinal gel, UPDRS unified Parkinson’s disease rating scale
aSix patients had video scoring of motor state at both of two time points. Changes were not tested statistically
bExcludes one patient at the final time point, who was considered “OFF” at all video recordings
cSome patients continued for up to 12 months
dExtension of Nyholm et al. (2005) crossover trial
The most common adverse events leading to discontinuation of chronic LCIG treatment have been related to medication delivery, including problems with tubing displacement or occlusion, the pump system, and stoma infections (Antonini et al. 2007, 2008, 2010b; Eggert et al. 2008; Nilsson et al. 2001). To monitor long-term safety, close observation is warranted, as guided by recent reports of neuropathy associated with homocysteine elevation and at least functional vitamin B12 and/or B6 deficiency (Klostermann et al. 2012).
Treatment of nonmotor symptoms
In general, published management recommendations for nonmotor PD symptoms have not attempted to differentiate between symptoms intrinsic to PD and those arising as complications of PD therapy. A contributory problem may be that in clinical studies of dopaminergic options, improvement of nonmotor PD symptoms, levodopa-related or not, has seldom been either a primary endpoint or a means for comparing treatments with potentially different abilities to produce CDD. In a double-blind, 12-week, parallel-group study of patients with early PD (Fung et al. 2009), oral LCE was superior to levodopa/carbidopa for improving quality of life, as rated by total score on the eight-item PDQ (PDQ-8) (Jenkinson et al. 1997b) and by subscores for the PDQ-8 nonmotor domains of depression, personal relationships, communication, and stigma. In a small single-dose, crossover study of oral levodopa/carbidopa CR versus IR (Kulisevsky et al. 2007), the seven PD patients with “wearing-off” showed significant mood improvement after IR treatment, while the seven nonfluctuating patients showed no mood improvement after receiving either drug. Plasma levodopa concentration correlated with anxiety level but not with mood.
Transdermal rotigotine has recently been assessed versus placebo in a large, double-blind trial (Trenkwalder et al. 2011a) in PD patients with unsatisfactory early morning motor-symptom control. On the PDSS-2 (Trenkwalder et al. 2011b), the mean 12-week change in total score (a coprimary outcome) was significantly improved in the rotigotine group compared with placebo from baseline to end of maintenance [least squares (LS) mean treatment difference, −4.26; 95 % CI: −6.08, −2.45; p < 0.0001]. Difficulty in falling asleep and feeling tired and sleepy in the morning were among the ten items showing significant improvement (among the instrument’s total of 15). Significant improvement versus placebo was also documented for mean change in total score on the NMSS (Martinez-Martin et al. 2009) from baseline to end of treatment (LS mean treatment difference, −6.65; 95 % CI: −11.99, −1.31; p = 0.015), with significant changes on the sleep/fatigue and the mood/cognition domains (LS mean treatment differences of −2.03; 95 % CI: −3.31, −0.75; p = 0.002 and −3.40; 95 % CI: −5.22, −1.58; p = 0.0003, respectively), and on the BDI-II depressive-symptomatology scale (Visser et al. 2006) from baseline to end of treatment (LS mean treatment difference, −2.01; 95 % CI: −3.55, −0.47; p = 0.011).
Improvement of nonmotor PD symptoms by subcutaneous apomorphine infusion has been a primary endpoint in two small prospective trials (Martinez-Martin et al. 2010; Reuter et al. 1999). In six patients with refractory nocturnal symptoms (Reuter et al. 1999), continuous overnight infusion (with placebo control in three of the subjects) was associated with decreases in awakenings, dystonia, pain, and nocturia. In an open-label trial (Martinez-Martin et al. 2010), 17 patients with advanced PD received subcutaneous apomorphine infusion and 17 received conventional therapy. At approximately 6 months, NMSS and PDQ-8 total scores showed significant improvement from baseline in the apomorphine group but did not change in the conventional-therapy group.
Improvement of nonmotor PD symptoms by intraduodenal LCIG infusion was the primary endpoint in a prospective, open-label trial conducted in 22 patients with daily motor fluctuations and dyskinesia refractory to optimized conventional therapy with oral medications, transdermal rotigotine, or subcutaneous apomorphine infusion (Honig et al. 2009). After discontinuation of the conventional therapy (except for nighttime oral dosing with levodopa CR or a long-acting dopamine agonist) and its replacement by LCIG for a mean of 6.7 months, mean change in NMSS total score showed significant improvement from baseline (−50.5, p = 0.0001). Of the nine NMSS domains, six were significantly improved [cardiovascular (−2.41, p = 0.0004), sleep/fatigue (−11.32, p = 0.0001), attention/memory (−3.27, p = 0.002), gastrointestinal (−6.23, p = 0.0003), urinary (−6.64, p = 0.002), and miscellaneous (−7.73, p = 0.0004)]. The change in total NMSS score was correlated with changes on measures of motor function [UPDRS motor-complication score (−5.91, p = 0.0000), UPDRS dyskinesia subscore (−3.7, p = 0.0001), and “OFF” time as a proportion of the waking day (r = 0.54, p < 0.01)]. On the PDSS and PDQ-8, mean improvement in total score was also significant (+28.51; p = 0.002 and −23.4; p = 0.0003, respectively).
Conclusions
For several decades, the pharmacologic treatment of PD has been evolving, most recently in a quest to achieve CDS or, more verifiably, CDD. Improvements in the steadiness of the plasma concentration-versus-time profiles of various dopaminergic therapies (Fig. 6) may be a signal of progress. However, improvements in plasma profile do not necessarily translate into a more continuous stimulation of central dopamine receptors. To directly evaluate the degree of CDS that a dopaminergic drug may confer, studies assessing dopamine-receptor occupancy (as measured, e.g. by brain imaging) will be necessary (Brooks et al. 2010).
Fig. 6.
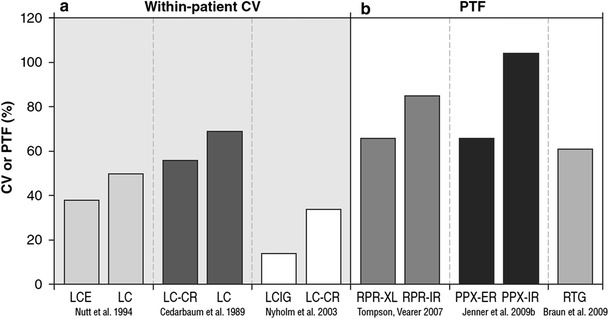
Variability in the plasma level of various formulations of dopaminergic therapies. Coefficient of variation (CV) (a)—the standard deviation in plasma level, expressed as a percentage of group geometric mean plasma level—for oral immediate-release levodopa/carbidopa/entacapone versus levodopa/carbidopa (LCE vs. LC), oral slow- versus immediate-release levodopa/carbidopa (LC-CR vs. LC), and intraduodenal levodopa/carbidopa intestinal gel versus oral slow-release levodopa/carbidopa (LCIG vs. LC-CR). Peak-to-trough fluctuation (PTF) (b)—C max − C min, expressed as a percentage of group geometric mean plasma level—for oral slow- versus immediate-release ropinirole (RPR-XL vs. RPR-IR), oral slow- versus immediate-release pramipexole (PPX-ER vs. PPX-IR), and transdermal rotigotine (RTG). CR controlled-release, ER and XL extended-release
So far, clinical studies of efforts to improve PD motor symptoms using therapies expected to provide more CDS have generally been positive, including double-blind, randomized trials with placebo control. However, the findings of studies comparing differing active treatments have often failed to find evidence favoring these approaches over an intermittent therapy. In such trials, levodopa/carbidopa CR, for example, was not superior to levodopa/carbidopa IR in advanced PD (Pahwa et al. 2006); LCE was not superior to levodopa/carbidopa, at least for delaying motor complications in early PD (Stocchi et al. 2010); pramipexole ER was not superior to pramipexole IR as an adjunct to levodopa in advanced PD (Schapira et al. 2011); and transdermal rotigotine was not superior either to IR ropinirole as monotherapy in early PD (Giladi et al. 2007) or to IR pramipexole as an adjunct to levodopa in advanced PD (Poewe et al. 2007). A conceivable explanation for the lack of substantial difference may be that the so-called standard-release dopamine agonists in fact have “longish” half-lives compared with levodopa IR and even with levodopa CR. By a similar argument, continuous agonist delivery using transdermal rotigotine would lack superiority to IR ropinirole because the half-life of the oral IR agent is already fairly long. However, transdermal rotigotine is not as effective as the infusional dopaminergic therapies (apomorphine or levodopa), suggesting that the inherent potency of each agent is also determinative. In studies of differing formulations of the same agent, i.e., levodopa, the longer-acting formulation has shown superior benefit (Hauser 2012). For their part, the infusional therapies presumably gain from accessing the blood stream without need for gastric transit. Currently, apomorphine is the only dopamine agonist rivaling levodopa in potency, and its half-life is shorter. In the MPTP primate PD model, its intermittent administration shares with levodopa a capacity to induce dyskinesia, but in the same model, animals undergoing continuous subcutaneous apomorphine infusion for up to 6 months did not become dyskinetic (Bibbiani et al. 2005). In PD patients, moreover, continuous apomorphine infusion has been found to downregulate preexisting dyskinesia (Colzi et al. 1998; Katzenschlager et al. 2005).
Clinical studies focusing on improving nonmotor PD symptoms are becoming more common. These trials, too, have not yet clarified any potential differences across therapies with differing capacities for CDD. Nevertheless, the findings of nonmotor improvement among recipients of subcutaneous apomorphine (Martinez-Martin et al. 2010) or intrajejunal LCIG (Honig et al. 2009) suggest that nonmotor PD symptoms or complications may improve in tandem with the expected motor improvements. For more persistent nonmotor problems, nondopaminergic treatments seem likely to remain key (Zesiewicz et al. 2010). Here, too, future research should explore drug activity at dopaminergic synapses, so as to determine whether CDS is, in fact, an important determinant of clinical efficacy. Certainly, the complexities of optimal PD management, and the rationale for an underlying strategy such as CDS or CDD, have not yet been thoroughly elucidated.
Acknowledgments
The authors would like to thank Michael Feirtag for his editorial assistance in the preparation of this manuscript and The Curry Rockefeller Group, LLC, Tarrytown, NY, for providing editorial support. Funding for this support was provided by Abbott. Abbott provided a medical accuracy review of the final manuscript but had no input on the development of the manuscript or presentation of the content. The authors are solely responsible for the content of the manuscript and also had final responsibility for the decision to submit for publication.
Conflict of interest
K. Ray Chaudhuri has received honoraria for lectures, travel expenses for conferences from UCB, Teva, Britannia Pharmaceuticals Ltd., Hospira, Abbott, GSK and unrestricted educational grants from Abbott, Boehringer Ingelheim, Britannia Pharmaceuticals Ltd., GlaxoSmithKline, and UCB. A. Rizos has served as a consultant for a training course for Britannia Pharmaceuticals Ltd. K. Sethi has served as a consultant for Novartis, GlaxoSmithKline, Boehringer Ingelheim, Schering Plough, Biogen, Teva, Solvay, Valeant, and Ipsen; received personal compensation for activities with Abbott, Synosia, Veloxis, and Teva; and received research support from GlaxoSmithKline, Teva, Acadia, Allergan, and Impax. He is employed part-time as a senior medical expert at Merz Pharmaceuticals.
References
- Antonini A, Poewe W. Fibrotic heart-valve reactions to dopamine-agonist treatment in Parkinson’s disease. Lancet Neurol. 2007;6:826–829. doi: 10.1016/S1474-4422(07)70218-1. [DOI] [PubMed] [Google Scholar]
- Antonini A, Isaias IU, Canesi M, Zibetti M, Mancini F, Manfredi L, et al. Duodenal levodopa infusion for advanced Parkinson’s disease: 12-month treatment outcome. Mov Disord. 2007;22:1145–1149. doi: 10.1002/mds.21500. [DOI] [PubMed] [Google Scholar]
- Antonini A, Mancini F, Canesi M, Zangaglia R, Isaias IU, Manfredi L, et al. Duodenal levodopa infusion improves quality of life in advanced Parkinson’s disease. Neurodegener Dis. 2008;5:244–246. doi: 10.1159/000113714. [DOI] [PubMed] [Google Scholar]
- Antonini A, Chaudhuri KR, Martinez-Martin P, Odin P. Oral and infusion levodopa-based strategies for managing motor complications in patients with Parkinson’s disease. CNS Drugs. 2010;24:119–129. doi: 10.2165/11310940-000000000-00000. [DOI] [PubMed] [Google Scholar]
- Antonini A, Bondiolotti G, Natuzzi F, Bareggi SR. Levodopa and 3-OMD levels in Parkinson patients treated with duodena. Eur Neuropsychopharmacol. 2010;20:683–687. doi: 10.1016/j.euroneuro.2010.04.010. [DOI] [PubMed] [Google Scholar]
- Apokyn® (2012) Apomorphine hydrochloride injection (package insert). Ravensburg, Germany: Vetter Pharma-Fertigung GmbH & Co. KG; Brisbane, CA: Tercica, Inc., a subsidiary of Ipsen Group, Feb 2012
- Azilect® (2009) Rasagiline mesylate tablets (package insert). Kansas City, MO: Teva Neuroscience, Inc., Dec 2009
- Baker WL, Silver D, White CM, Kluger J, Aberle J, Patel AA, Coleman CI. Dopamine agonists in the treatment of early Parkinson’s disease: a meta-analysis. Parkinsonism Relat Disord. 2009;15:287–294. doi: 10.1016/j.parkreldis.2008.07.004. [DOI] [PubMed] [Google Scholar]
- Bibbiani F, Costantini LC, Patel R, Chase TN. Continuous dopaminergic stimulation reduces risk of motor complications in parkinsonian primates. Exp Neurol. 2005;192:73–78. doi: 10.1016/j.expneurol.2004.11.013. [DOI] [PubMed] [Google Scholar]
- Braun M, Cawello W, Boekens H, Horstmann R. Influence of domperidone on pharmacokinetics, safety and tolerability of the dopamine agonist rotigotine. Br J Clin Pharmacol. 2009;67:209–215. doi: 10.1111/j.1365-2125.2008.03334.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bravi D, Mouradian MM, Roberts JW, Davis TL, Sohn YH, Chase TN. Wearing-off fluctuations in Parkinson’s disease: contribution of postsynaptic mechanisms. Ann Neurol. 1994;36:27–31. doi: 10.1002/ana.410360108. [DOI] [PubMed] [Google Scholar]
- Brooks DJ, Papapetropoulos S, Vandenhende F, Tomic D, He P, Coppell A, O’Neill G. An open-label, positron emission tomography study to assess adenosine A2A brain receptor occupancy of vipadenant (BIIB014) at steady-state levels in healthy male volunteers. Clin Neuropharmacol. 2010;33:55–60. doi: 10.1097/WNF.0b013e3181d137d2. [DOI] [PubMed] [Google Scholar]
- Cawello W, Wolff HM, Meuling WJ, Horstmann R, Braun M. Transdermal administration of radiolabelled (14C) rotigotine by a patch formulation: a mass balance trial. Clin Pharmacokinet. 2007;46:851–857. doi: 10.2165/00003088-200746100-00003. [DOI] [PubMed] [Google Scholar]
- Cawello W, Braun M, Boekens H. Absorption, disposition, metabolic fate, and elimination of the dopamine agonist rotigotine in man: administration by intravenous infusion or transdermal delivery. Drug Metab Dispos. 2009;37:2055–2060. doi: 10.1124/dmd.109.027383. [DOI] [PubMed] [Google Scholar]
- Cedarbaum JM. Clinical pharmacokinetics of anti-parkinsonian drugs. Clin Pharmacokinet. 1987;13:141–178. doi: 10.2165/00003088-198713030-00002. [DOI] [PubMed] [Google Scholar]
- Cedarbaum JM, Kutt H, McDowell FH. A pharmacokinetic and pharmacodynamic comparison of Sinemet CR (50/200) and standard Sinemet (25/100) Neurology. 1989;39(11 Suppl 2):38–44. [PubMed] [Google Scholar]
- Chapuis S, Ouchchane L, Metz O, Gerbaud L, Durif F. Impact of the motor complications of Parkinson’s disease on the quality of life. Mov Disord. 2005;20:224–230. doi: 10.1002/mds.20279. [DOI] [PubMed] [Google Scholar]
- Chase TN, Baronti F, Fabbrini G, Heuser IJ, Juncos JL, Mouradian MM. Rationale for continuous dopaminomimetic therapy of Parkinson’s disease. Neurology. 1989;39(11 Suppl 2):7–10. [PubMed] [Google Scholar]
- Chaudhuri KR, Schapira AH. Non-motor symptoms of Parkinson’s disease: dopaminergic pathophysiology and treatment. Lancet Neurol. 2009;8:464–474. doi: 10.1016/S1474-4422(09)70068-7. [DOI] [PubMed] [Google Scholar]
- Chaudhuri KR, Prieto-Jurcynska C, Naidu Y, Mitra T, Frades-Pavo B, Tluk S, et al. The nondeclaration of nonmotor symptoms of Parkinson’s disease to health care professionals: an international study using the nonmotor symptoms questionnaire. Mov Disord. 2010;25:704–709. doi: 10.1002/mds.22868. [DOI] [PubMed] [Google Scholar]
- Chaudhuri KR, Odin P, Antonini A, Martinez-Martin P. Parkinson’s disease: the non-motor issues. Parkinsonism Relat Disord. 2011;17:717–723. doi: 10.1016/j.parkreldis.2011.02.018. [DOI] [PubMed] [Google Scholar]
- Colzi A, Turner K, Lees AJ. Continuous subcutaneous waking day apomorphine in the long term treatment of levodopa induced interdose dyskinesias in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1998;64:573–576. doi: 10.1136/jnnp.64.5.573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Damiano AM, McGrath MM, Willian MK, Snyder CF, LeWitt PA, Reyes PF, et al. Evaluation of a measurement strategy for Parkinson’s disease: assessing patient health-related quality of life. Qual Life Res. 2000;9:87–100. doi: 10.1023/A:1008928321652. [DOI] [PubMed] [Google Scholar]
- Deleu D, Northway MG, Hanssens Y. Clinical pharmacokinetic and pharmacodynamic properties of drugs used in the treatment of Parkinson’s disease. Clin Pharmacokinet. 2002;41:261–309. doi: 10.2165/00003088-200241040-00003. [DOI] [PubMed] [Google Scholar]
- Deleu D, Hanssens Y, Northway MG. Subcutaneous apomorphine: an evidence-based review of its use in Parkinson’s disease. Drugs Aging. 2004;21:687–709. doi: 10.2165/00002512-200421110-00001. [DOI] [PubMed] [Google Scholar]
- Dempski RE, Scholtz EC, Oberholtzer ER, Yeh KC. Pharmaceutical design and development of a Sinemet controlled-release formulation. Neurology. 1989;39(11 Suppl 2):20–24. [PubMed] [Google Scholar]
- Di Giovanni G, Di Matteo V, Pierucci M, Esposito E. Serotonin-dopamine interaction: electrophysiological evidence. Prog Brain Res. 2008;172:45–71. doi: 10.1016/S0079-6123(08)00903-5. [DOI] [PubMed] [Google Scholar]
- Eggert K, Schrader C, Hahn M, Stamelou M, Rüssmann A, Dengler R, et al. Continuous jejunal levodopa infusion in patients with advanced Parkinson disease: practical aspects and outcome of motor and non-motor complications. Clin Neuropharmacol. 2008;31:151–166. doi: 10.1097/wnf.0b013e31814b113e. [DOI] [PubMed] [Google Scholar]
- Eldepryl® (2011) Selegiline hydrochloride (package insert). Morgantown, WV: Somerset Pharmaceuticals, Inc., Aug 2011
- Erni W, Held K. The hydrodynamically balanced system: a novel principle of controlled drug release. Eur Neurol. 1987;27(Suppl 1):21–27. doi: 10.1159/000116171. [DOI] [PubMed] [Google Scholar]
- Fahn S, Elton RL, UPDRS Development Committee . Unified Parkinson’s disease rating scale. In: Fahn S, Marsden CD, Calne DB, Goldstein M, editors. Recent developments in Parkinson’s disease. Florham Park: Macmillan; 1987. pp. 153–163. [Google Scholar]
- Frankel JP, Kempster PA, Bovingdon M, Webster R, Lees AJ, Stern GM. The effects of oral protein on the absorption of intraduodenal levodopa and motor performance. J Neurol Neurosurg Psychiatry. 1989;52:1063–1067. doi: 10.1136/jnnp.52.9.1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fung VS, Herawati L, Wan Y, Movement Disorder Society of Australia Clinical Research and Trials Group. QUEST-AP Study Group Quality of life in early Parkinson’s disease treated with levodopa/carbidopa/entacapone. Mov Disord. 2009;24:25–31. doi: 10.1002/mds.21878. [DOI] [PubMed] [Google Scholar]
- Gancher ST, Woodward WR, Boucher B, Nutt JG. Peripheral pharmacokinetics of apomorphine in humans. Ann Neurol. 1989;26:232–238. doi: 10.1002/ana.410260209. [DOI] [PubMed] [Google Scholar]
- García-Ruiz PJ, Sesar Ignacio A, Ares Pensado B, Castro García A, Alonso Frech F, Alvarez López M, et al. Efficacy of long-term continuous subcutaneous apomorphine infusion in advanced Parkinson’s disease with motor fluctuations: a multicenter study. Mov Disord. 2008;23:1130–1136. doi: 10.1002/mds.22063. [DOI] [PubMed] [Google Scholar]
- Giladi N, Boroojerdi B, Korczyn AD, Burn DJ, Clarke CE, Schapira AH, SP513 Investigators Rotigotine transdermal patch in early Parkinson’s disease: a randomized, double-blind, controlled study versus placebo and ropinirole. Mov Disord. 2007;22:2398–2404. doi: 10.1002/mds.21741. [DOI] [PubMed] [Google Scholar]
- Goto Y, Otani S, Grace AA. The Yin and Yang of dopamine release: a new perspective. Neuropharmacology. 2007;53:583–587. doi: 10.1016/j.neuropharm.2007.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grace AA. Physiology of the normal and dopamine-depleted basal ganglia: insights into levodopa pharmacotherapy. Mov Disord. 2008;23(Suppl 3):S560–S569. doi: 10.1002/mds.22020. [DOI] [PubMed] [Google Scholar]
- Grandas F, Galiano ML, Tabernero C. Risk factors for levodopa-induced dyskinesias in Parkinson’s disease. J Neurol. 1999;246:1127–1133. doi: 10.1007/s004150050530. [DOI] [PubMed] [Google Scholar]
- Gunal DI, Nurichalichi K, Tuncer N, Bekiroglu N, Aktan S. The clinical profile of nonmotor fluctuations in Parkinson’s disease patients. Can J Neurol Sci. 2002;29:61–64. doi: 10.1140/epjb/e2002-00262-2. [DOI] [PubMed] [Google Scholar]
- Hauser RA. IPX066: a novel carbidopa-levodopa extended-release formulation. Expert Rev Neurother. 2012;12:133–140. doi: 10.1586/ern.11.195. [DOI] [PubMed] [Google Scholar]
- Hauser RA, Lew MF, Hurtig HI, Wojcieszek J, Fitzer-Attas CJ, TEMPO Open-label Study Group Long-term outcome of early versus delayed rasagiline treatment in early Parkinson’s disease. Mov Disord. 2009;24:564–573. doi: 10.1002/mds.22402. [DOI] [PubMed] [Google Scholar]
- Hauser RA, Panisset M, Abbruzzese G, Mancione L, Dronamraju N, Kakarieka A, FIRST-STEP Study Group Double-blind trial of levodopa/carbidopa/entacapone versus levodopa/carbidopa in early Parkinson’s disease. Mov Disord. 2009;24:541–550. doi: 10.1002/mds.22343. [DOI] [PubMed] [Google Scholar]
- Hauser RA, Schapira AH, Rascol O, Barone P, Mizuno Y, Salin L, et al. Randomized, double-blind, multicenter evaluation of pramipexole extended release once daily in early Parkinson’s disease. Mov Disord. 2010;25:2542–2549. doi: 10.1002/mds.23317. [DOI] [PubMed] [Google Scholar]
- Hofmann C, Penner U, Dorow R, Pertz HH, Jähnichen S, Horowski R, Latté KP, Palla D, Schurad B. Lisuride, a dopamine receptor agonist with 5-HT2B receptor antagonist properties: absence of cardiac valvulopathy adverse drug reaction reports supports the concept of a crucial role for 5-HT2B receptor agonism in cardiac valvular fibrosis. Clin Neuropharmacol. 2006;29:80–86. doi: 10.1097/00002826-200603000-00005. [DOI] [PubMed] [Google Scholar]
- Hofstee DJ, Neef C, van Laar T, Jansen EN. Pharmacokinetics of apomorphine in Parkinson’s disease: plasma and cerebrospinal fluid levels in relation to motor responses. Clin Neuropharmacol. 1994;17:45–52. doi: 10.1097/00002826-199402000-00005. [DOI] [PubMed] [Google Scholar]
- Honig H, Antonini A, Martinez-Martin P, Forgacs I, Faye GC, Fox T, et al. Intrajejunal levodopa infusion in Parkinson’s disease: a pilot multicenter study of effects on nonmotor symptoms and quality of life. Mov Disord. 2009;24:1468–1474. doi: 10.1002/mds.22596. [DOI] [PubMed] [Google Scholar]
- Horstink M, Tolosa E, Bonuccelli U, Deuschl G, Friedman A, Kanovsky P, European Federation of Neurological Societies. Movement Disorder Society-European Section et al. Review of the therapeutic management of Parkinson’s disease: report of a joint task force of the European Federation of Neurological Societies and the Movement Disorder Society-European Section: part I: early (uncomplicated) Parkinson’s disease. Eur J Neurol. 2006;13:1170–1185. doi: 10.1111/j.1468-1331.2006.01547.x. [DOI] [PubMed] [Google Scholar]
- Isacson D, Bingefors K, Kristiansen IS, Nyholm D. Fluctuating functions related to quality of life in advanced Parkinson disease: effects of duodenal levodopa infusion. Acta Neurol Scand. 2008;118:379–386. doi: 10.1111/j.1600-0404.2008.01049.x. [DOI] [PubMed] [Google Scholar]
- Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson’s disease questionnaire (PDQ-39): development and validation of a Parkinson’s disease summary index score. Age Ageing. 1997;26:353–357. doi: 10.1093/ageing/26.5.353. [DOI] [PubMed] [Google Scholar]
- Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The PDQ-8: development and validation of a short-form Parkinson’s disease questionnaire. Psychol Health. 1997;12:805–814. doi: 10.1080/08870449708406741. [DOI] [Google Scholar]
- Jenner P. Preventing and controlling dyskinesia in Parkinson’s disease—a view of current knowledge and future opportunities. Mov Disord. 2008;23(Suppl 3):S585–S598. doi: 10.1002/mds.22022. [DOI] [PubMed] [Google Scholar]
- Jenner P. From the MPTP-treated primate to the treatment of motor complications in Parkinson’s disease. Parkinsonism Relat Disord. 2009;15(Suppl 4):S18–S23. doi: 10.1016/S1353-8020(09)70829-6. [DOI] [PubMed] [Google Scholar]
- Jenner P, Könen-Bergmann M, Schepers C, Haertter S. Pharmacokinetics of a once-daily extended-release formulation of pramipexole in healthy male volunteers: three studies. Clin Ther. 2009;31:2698–2711. doi: 10.1016/j.clinthera.2009.10.018. [DOI] [PubMed] [Google Scholar]
- Kaakkola S, Männistö PT, Nissinen E, Vuorela A, Mäntylä R. The effect of an increased ratio of carbidopa to levodopa on the pharmacokinetics of levodopa. Acta Neurol Scand. 1985;72:385–391. doi: 10.1111/j.1600-0404.1985.tb00888.x. [DOI] [PubMed] [Google Scholar]
- Katzenschlager R, Hughes A, Evans A, Manson AJ, Hoffman M, Swinn L, et al. Continuous subcutaneous apomorphine therapy improves dyskinesias in Parkinson’s disease: a prospective study using single-dose challenges. Mov Disord. 2005;20:151–157. doi: 10.1002/mds.20276. [DOI] [PubMed] [Google Scholar]
- Kieburtz K, Antonini A, Olanow CW, Fernandez HH, Espay AJ, Standaert DG, Hass S. Randomized, phase 3, double-blind, double-dummy study of levodopa-carbidopa intestinal gel in patients with advanced Parkinson’s disease: functional and quality-of-life outcomes (abstract) Mov Disord. 2012;27(Suppl 1):385. [Google Scholar]
- Klostermann F, Jugel C, Müller T, Marzinzik F. Malnutritional neuropathy under intestinal levodopa infusion. J Neural Transm. 2012;119:369–372. doi: 10.1007/s00702-011-0689-3. [DOI] [PubMed] [Google Scholar]
- Kulisevsky J, Pascual-Sedano B, Barbanoj M, Gironell A, Pagonabarraga J, García-Sánchez C. Acute effects of immediate and controlled-release levodopa on mood in Parkinson’s disease: a double-blind study. Mov Disord. 2007;22:62–67. doi: 10.1002/mds.21205. [DOI] [PubMed] [Google Scholar]
- Kurlan R, Rothfield KP, Woodward WR, Nutt JG, Miller C, Lichter D, Shoulson I. Erratic gastric emptying of levodopa may cause “random” fluctuations of parkinsonian mobility. Neurology. 1988;38:419–421. doi: 10.1212/WNL.38.3.419. [DOI] [PubMed] [Google Scholar]
- Kvernmo T, Härtter S, Burger E. A review of the receptor-binding and pharmacokinetic properties of dopamine agonists. Clin Ther. 2006;28:1065–1078. doi: 10.1016/j.clinthera.2006.08.004. [DOI] [PubMed] [Google Scholar]
- LeWitt PA. Subcutaneously administered apomorphine: pharmacokinetics and metabolism. Neurology. 2004;62(6 Suppl 4):S8–S11. doi: 10.1212/WNL.62.6_suppl_4.S8. [DOI] [PubMed] [Google Scholar]
- LeWitt PA, Lyons KE, Pahwa R, SP 650 Study Group Advanced Parkinson disease treated with rotigotine transdermal system: PREFER study. Neurology. 2007;68:1262–1267. doi: 10.1212/01.wnl.0000259516.61938.bb. [DOI] [PubMed] [Google Scholar]
- LeWitt PA, Jennings D, Lyons KE, Pahwa R, Rabinowicz AL, Wang J, et al. Pharmacokinetic-pharmacodynamic crossover comparison of two levodopa extension strategies. Mov Disord. 2009;24:1319–1324. doi: 10.1002/mds.22587. [DOI] [PubMed] [Google Scholar]
- Manson AJ, Hanagasi H, Turner K, Patsalos PN, Carey P, Ratnaraj N, Lees AJ. Intravenous apomorphine therapy in Parkinson’s disease: clinical and pharmacokinetic observations. Brain. 2001;124:331–340. doi: 10.1093/brain/124.2.331. [DOI] [PubMed] [Google Scholar]
- Markham C, Diamond SG, Treciokas LJ. Carbidopa in Parkinson disease and in nausea and vomiting of levodopa. Arch Neurol. 1974;31:128–133. doi: 10.1001/archneur.1974.00490380076010. [DOI] [PubMed] [Google Scholar]
- Marsden CD. The mysterious motor function of the basal ganglia: the Robert Wartenberg lecture. Neurology. 1982;32:514–539. doi: 10.1212/WNL.32.5.514. [DOI] [PubMed] [Google Scholar]
- Marsden CD, Parkes JD. “On–off” effects in patients with Parkinson’s disease on chronic levodopa therapy. Lancet. 1976;1:292–296. doi: 10.1016/S0140-6736(76)91416-1. [DOI] [PubMed] [Google Scholar]
- Martinez-Martin P, Rodriguez-Blazquez C, Abe K, Bhattacharyya KB, Bloem BR, Carod-Artal FJ, et al. International study on the psychometric attributes of the non-motor symptoms scale in Parkinson disease. Neurology. 2009;73:1584–1591. doi: 10.1212/WNL.0b013e3181c0d416. [DOI] [PubMed] [Google Scholar]
- Martinez-Martin P, Todorova A, Odin P, Odin T, Henriksen Y, Naidu S, et al. Motor and non motor efficacy of subcutaneous apomorphine infusion in advanced PD compared to Parkinson’s patients on conventional therapy (MDS abstract 711) Mov Disord. 2010;25(7 Suppl 2):S421. [Google Scholar]
- Martinez-Martin P, Rodriguez-Blazquez C, Kurtis MM, Chaudhuri KR, NMSS Validation Group The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Mov Disord. 2011;26:399–406. doi: 10.1002/mds.23462. [DOI] [PubMed] [Google Scholar]
- Martínez-Martín P, Benito-León J, Burguera JA, Castro A, Linazasoro G, Martínez-Castrillo JC, et al. The SCOPA-motor scale for assessment of Parkinson’s disease is a consistent and valid measure. J Clin Epidemiol. 2005;58:674–679. doi: 10.1016/j.jclinepi.2004.09.014. [DOI] [PubMed] [Google Scholar]
- Merello M, Lees AJ, Webster R, Bovingdon M, Gordin A. Effect of entacapone, a peripherally acting catechol-O-methyltransferase inhibitor, on the motor response to acute treatment with levodopa in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1994;57:186–189. doi: 10.1136/jnnp.57.2.186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicolle E, Pollak P, Serre-Debeauvais F, Richard P, Gervason CL, Broussolle E, Gavend M. Pharmacokinetics of apomorphine in parkinsonian patients. Fundam Clin Pharmacol. 1993;7:245–252. doi: 10.1111/j.1472-8206.1993.tb00238.x. [DOI] [PubMed] [Google Scholar]
- Nilsson D, Nyholm D, Aquilonius SM. Duodenal levodopa infusion in Parkinson’s disease—long-term experience. Acta Neurol Scand. 2001;104:343–348. doi: 10.1034/j.1600-0404.2001.00153.x. [DOI] [PubMed] [Google Scholar]
- Nutt JG. Effects of catechol-O-methyl transferase (COMT) inhibition on the pharmacokinetics of l-dopa. Adv Neurol. 1996;69:493–496. [PubMed] [Google Scholar]
- Nutt JG. Effect of COMT inhibition on the pharmacokinetics and pharmacodynamics of levodopa in parkinsonian patients. Neurology. 2000;55(11 Suppl 4):S33–S37. [PubMed] [Google Scholar]
- Nutt JG, Gancher ST, Woodward WR. Motor fluctuations in Parkinson’s disease. Ann Neurol. 1989;25:633–634. doi: 10.1002/ana.410250619. [DOI] [PubMed] [Google Scholar]
- Nutt JG, Woodward WR, Beckner RM, Stone CK, Berggren K, Carter JH, et al. Effect of peripheral catechol-O-methyltransferase inhibition on the pharmacokinetics and pharmacodynamics of levodopa in parkinsonian patients. Neurology. 1994;44:913–919. doi: 10.1212/WNL.44.5.913. [DOI] [PubMed] [Google Scholar]
- Nutt JG, Obeso JA, Stocchi F. Continuous dopamine-receptor stimulation in advanced Parkinson’s disease. Trends Neurosci. 2000;23(10 Suppl):S109–S115. doi: 10.1016/S1471-1931(00)00029-X. [DOI] [PubMed] [Google Scholar]
- Nyholm D, Askmark H, Gomes-Trolin C, Knutson T, Lennernäs H, Nyström C, Aquilonius SM. Optimizing levodopa pharmacokinetics: intestinal infusion versus oral sustained-release tablets. Clin Neuropharmacol. 2003;26:156–163. doi: 10.1097/00002826-200305000-00010. [DOI] [PubMed] [Google Scholar]
- Nyholm D, Nilsson Remahl AI, Dizdar N, Constantinescu R, Holmberg B, Jansson R, et al. Duodenal levodopa infusion monotherapy versus oral polypharmacy in advanced Parkinson disease. Neurology. 2005;64:216–223. doi: 10.1212/01.WNL.0000149637.70961.4C. [DOI] [PubMed] [Google Scholar]
- Obeso JA, Olanow CW, Nutt JG. Levodopa motor complications in Parkinson’s disease. Trends Neurosci. 2000;23(Suppl):S2–S7. doi: 10.1016/S1471-1931(00)00031-8. [DOI] [PubMed] [Google Scholar]
- Obeso JA, Marin C, Rodriguez-Oroz MC, Blesa J, Benitez-Temiño B, Mena-Segovia J, et al. The basal ganglia in Parkinson’s disease: current concepts and unexplained observations. Ann Neurol. 2008;64(Suppl 2):S30–S46. doi: 10.1002/ana.21481. [DOI] [PubMed] [Google Scholar]
- Olanow CW, Obeso JA. Preventing levodopa-induced dyskinesia. Ann Neurol. 2000;47:167–178. [PubMed] [Google Scholar]
- Olanow CW, Obeso JA, Stocchi F. Continuous dopamine-receptor treatment of Parkinson’s disease: scientific rationale and clinical implications. Lancet Neurol. 2006;5:677–687. doi: 10.1016/S1474-4422(06)70521-X. [DOI] [PubMed] [Google Scholar]
- Olanow CW, Stern MB, Sethi K. The scientific and clinical basis for the treatment of Parkinson disease. Neurology. 2009;72(21 Suppl 4):S1–S136. doi: 10.1212/WNL.0b013e3181a1d44c. [DOI] [PubMed] [Google Scholar]
- Olanow CW, Chatamra K, Benesh J, Pritchett YL, Lenz RA. Design of a randomized, double-blind, double-dummy, placebo-controlled study of levodopa-carbidopa intestinal gel in patients currently receiving optimized treatment for advanced Parkinson’s disease. Mov Disord. 2011;26(Suppl 2):S137. [Google Scholar]
- Olanow CW, Antonini A, Kieburtz K, Fernandez HH, Espay AJ, Standaert DG, Vanagunas AD. Randomized, double-blind, double-dummy study of continuous infusion of levodopa-carbidopa intestinal gel in patients with advanced Parkinson’s disease: efficacy and safety (abstract) Mov Disord. 2012;27(Suppl 1):411. [Google Scholar]
- Pahwa R, Lyons K, McGuire D, Silverstein P, Zwiebel F, Robischon M, Koller WC. Comparison of standard carbidopa-levodopa and sustained-release carbidopa-levodopa in Parkinson’s disease: pharmacokinetic and quality-of-life measures. Mov Disord. 1997;12:677–681. doi: 10.1002/mds.870120508. [DOI] [PubMed] [Google Scholar]
- Pahwa R, Factor SA, Lyons KE, Ondo WG, Gronseth G, Bronte-Stewart H, et al. Practice parameter: treatment of Parkinson disease with motor fluctuations and dyskinesia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2006;66:983–995. doi: 10.1212/01.wnl.0000215250.82576.87. [DOI] [PubMed] [Google Scholar]
- Pahwa R, Stacy MA, Factor SA, Lyons KE, Stocchi F, Hersh BP, EASE-PD Adjunct Study Investigators et al. Ropinirole 24-hour prolonged release: randomized, controlled study in advanced Parkinson disease. Neurology. 2007;68:1108–1115. doi: 10.1212/01.wnl.0000258660.74391.c1. [DOI] [PubMed] [Google Scholar]
- Parkinson Study Group A controlled, randomized, delayed-start study of rasagiline in early parkinson disease. Arch Neurol. 2004;61:561–566. doi: 10.1001/archneur.61.4.561. [DOI] [PubMed] [Google Scholar]
- Parkinson Study Group CALM Cohort Investigators Long-term effect of initiating pramipexole vs levodopa in early Parkinson disease. Arch Neurol. 2009;66:563–570. doi: 10.1001/archneurol.2009.32. [DOI] [PubMed] [Google Scholar]
- Pearce RK, Banerji T, Jenner P, Marsden CD. De novo administration of ropinirole and bromocriptine induces less dyskinesia than l-dopa in the MPTP-treated marmoset. Mov Disord. 1998;13:234–241. doi: 10.1002/mds.870130207. [DOI] [PubMed] [Google Scholar]
- Pfieffer RF. A promising new technology for Parkinson’s disease. Neurology. 2005;65(Suppl 1):S6–S10. doi: 10.1212/WNL.65.2_suppl_1.S6. [DOI] [PubMed] [Google Scholar]
- Piccini P, Brooks DJ, Korpela K, Pavese N, Karlsson M, Gordin A. The catechol-O-methyltransferase (COMT) inhibitor entacapone enhances the pharmacokinetic and clinical response to Sinemet CR in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2000;68:589–594. doi: 10.1136/jnnp.68.5.589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poewe WH, Rascol O, Quinn N, Tolosa E, Oertel WH, Martignoni E, Rupp M, Boroojerdi B, SP 515 Investigators Efficacy of pramipexole and transdermal rotigotine in advanced Parkinson’s disease: a double-blind, double-dummy, randomised controlled trial. Lancet Neurol. 2007;6:513–520. doi: 10.1016/S1474-4422(07)70108-4. [DOI] [PubMed] [Google Scholar]
- Politis M, Piccini P, Pavese N, Koh SB, Brooks DJ. Evidence of dopamine dysfunction in the hypothalamus of patients with Parkinson’s disease: an in vivo 11C-raclopride PET study. Exp Neurol. 2008;214:112–116. doi: 10.1016/j.expneurol.2008.07.021. [DOI] [PubMed] [Google Scholar]
- Rascol O, Brooks DJ, Melamed E, Oertel W, Poewe W, Stocchi F, Tolosa E, LARGO study group Rasagiline as an adjunct to levodopa in patients with Parkinson’s disease and motor fluctuations (LARGO, lasting effect in adjunct therapy with Rasagiline given once daily, study): a randomised, double-blind, parallel-group trial. Lancet. 2005;365:947–954. doi: 10.1016/S0140-6736(05)71083-7. [DOI] [PubMed] [Google Scholar]
- Reuter I, Ellis CM, Chaudhuri KR. Nocturnal subcutaneous apomorphine infusion in Parkinson’s disease and restless legs syndrome. Acta Neurol Scand. 1999;100:163–167. doi: 10.1111/j.1600-0404.1999.tb00732.x. [DOI] [PubMed] [Google Scholar]
- Rizos A, Martinez-Martin P, Martin A, Henriksen T, Kessel B, Koch I, Durner G. European multicentre survey of tolerability rates and impulse control behaviour trends of prolonged release dopamine agonists in young and old PD (abstract) Mov Disord. 2012;27(Suppl 1):161. [Google Scholar]
- Robertson DR, Wood ND, Everest H, Monks K, Waller DG, Renwick AG, George CF. The effect of age on the pharmacokinetics of levodopa administered alone and in the presence of carbidopa. Br J Clin Pharmacol. 1989;28:61–69. doi: 10.1111/j.1365-2125.1989.tb03506.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruottinen HM, Rinne UK. Effect of one month’s treatment with peripherally acting catechol-O-methyltransferase inhibitor, entacapone, on pharmacokinetics and motor response to levodopa in advanced parkinsonian patients. Clin Neuropharmacol. 1996;19:222–233. doi: 10.1097/00002826-199619030-00004. [DOI] [PubMed] [Google Scholar]
- Ruottinen HM, Rinne UK. Entacapone prolongs levodopa response in a one month double blind study in parkinsonian patients with levodopa related fluctuations. J Neurol Neurosurg Psychiatry. 1996;60:36–40. doi: 10.1136/jnnp.60.1.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sage JI, Mark MH. Pharmacokinetics of continuous-release carbidopa/levodopa. Clin Neuropharmacol. 1994;17(Suppl 2):S1–S6. [PubMed] [Google Scholar]
- Schapira AHV, Barone P, Hauser RA, Mizuno Y, Rascol O, Busse M, et al. Extended-release pramipexole in advanced Parkinson’s disease: a randomized controlled trial. Neurology. 2011;77:767–774. doi: 10.1212/WNL.0b013e31822affdb. [DOI] [PubMed] [Google Scholar]
- Scheller D, Ullmer C, Berkels R, Gwarek M, Lübbert H. The in vitro receptor profile of rotigotine: a new agent for the treatment of Parkinson’s disease. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:73–86. doi: 10.1007/s00210-008-0341-4. [DOI] [PubMed] [Google Scholar]
- Schultz W. Behavior-related activity of primate dopamine neurons. Rev Neurol (Paris) 1994;150:634–639. [PubMed] [Google Scholar]
- Simuni T, Sethi K. Nonmotor manifestations of Parkinson’s disease. Ann Neurol. 2008;64(Suppl 2):S65–S80. doi: 10.1002/ana.21472. [DOI] [PubMed] [Google Scholar]
- Stocchi F, Hersh BP, Scott BL, Nausieda PA, Giorgi L, Ease-PD Monotherapy Study Investigators Ropinirole 24-hour prolonged release and ropinirole immediate release in early Parkinson’s disease: a randomized, double-blind, non-inferiority crossover study. Curr Med Res Opin. 2008;24:2883–2895. doi: 10.1185/03007990802387130. [DOI] [PubMed] [Google Scholar]
- Stocchi F, Rascol O, Kieburtz K, Poewe W, Jankovic J, Tolosa E, et al. Initiating levodopa/carbidopa therapy with and without entacapone in early Parkinson disease: the STRIDE-PD study. Ann Neurol. 2010;68:18–27. doi: 10.1002/ana.22060. [DOI] [PubMed] [Google Scholar]
- Stocchi F, Giorgi L, Hunter B, Schapira AH. PREPARED: comparison of prolonged and immediate release ropinirole in advanced Parkinson’s disease. Mov Disord. 2011;26:1259–1265. doi: 10.1002/mds.23498. [DOI] [PubMed] [Google Scholar]
- Stowe RL, Ives NJ, Clarke C, van Hilten J, Ferreira J, Hawker RJ, et al. Dopamine agonist therapy in early Parkinson’s disease. Cochrane Database Syst Rev. 2008;2:CD006564. doi: 10.1002/14651858.CD006564.pub2. [DOI] [PubMed] [Google Scholar]
- Stowe R, Ives N, Clarke CE, van Hilten J, Wheatley K, et al. Evaluation of the efficacy and safety of adjuvant treatment to levodopa therapy in Parkinson’s disease patients with motor complications. Cochrane Database Syst Rev. 2010;7:CD007166. doi: 10.1002/14651858.CD007166.pub2. [DOI] [PubMed] [Google Scholar]
- Talati R, Reinhart K, Baker W, White CM, Coleman CI. Pharmacologic treatment of advanced Parkinson’s disease: a meta-analysis of COMT inhibitors and MAO-B inhibitors. Parkinsonism Relat Disord. 2009;15:500–505. doi: 10.1016/j.parkreldis.2008.12.007. [DOI] [PubMed] [Google Scholar]
- Tasmar® (2009) Tolcapone (package insert). Aliso Viejo, CA: Valeant Pharmaceuticals North America, June 2009
- Tolosa E, Martí MJ, Valldeoriola F, Molinuevo JL. History of levodopa and dopamine agonists in Parkinson’s disease treatment. Neurology. 1998;50(6 Suppl 6):S2–S10. doi: 10.1212/WNL.50.6_Suppl_6.S2. [DOI] [PubMed] [Google Scholar]
- Tompson DJ, Vearer D. Steady-state pharmacokinetic properties of a 24-hour prolonged-release formulation of ropinirole: results of two randomized studies in patients with Parkinson’s disease. Clin Ther. 2007;29:2654–2666. doi: 10.1016/j.clinthera.2007.12.010. [DOI] [PubMed] [Google Scholar]
- Trenkwalder C, Kies B, Rudzinska M, Fine J, Nikl J, Honczarenko K, Recover Study Group et al. Rotigotine effects on early morning motor function and sleep in Parkinson’s disease: a double-blind, randomized, placebo-controlled study (RECOVER) Mov Disord. 2011;26:90–99. doi: 10.1002/mds.23441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trenkwalder C, Kohnen R, Högl B, Metta V, Sixel-Döring F, Frauscher B, et al. Parkinson disease sleep scale—validation of the revised version PDSS-2. Mov Disord. 2011;26:644–652. doi: 10.1002/mds.23476. [DOI] [PubMed] [Google Scholar]
- Venton BJ, Zhang H, Garris PA, Phillips PE, Sulzer D, Wightman RM. Real-time decoding of dopamine concentration changes in the caudate-putamen during tonic and phasic firing. J Neurochem. 2003;87:1284–1295. doi: 10.1046/j.1471-4159.2003.02109.x. [DOI] [PubMed] [Google Scholar]
- Verhagen Metman L, Locatelli ER, Bravi D, Mouradian MM, Chase TN. Apomorphine responses in Parkinson’s disease and the pathogenesis of motor complications. Neurology. 1997;48:369–372. doi: 10.1212/WNL.48.2.369. [DOI] [PubMed] [Google Scholar]
- Visser M, Leentjens AF, Marinus J, Stiggelbout AM, van Hilten JJ. Reliability and validity of the Beck depression inventory in patients with Parkinson’s disease. Mov Disord. 2006;21:668–672. doi: 10.1002/mds.20792. [DOI] [PubMed] [Google Scholar]
- Watts RL, Lyons KE, Pahwa R, Sethi K, Stern M, Hauser RA, 228 Study Investigators et al. Onset of dyskinesia with adjunct ropinirole prolonged-release or additional levodopa in early Parkinson’s disease. Mov Disord. 2010;25:858–866. doi: 10.1002/mds.22890. [DOI] [PubMed] [Google Scholar]
- Weintraub D, Nirenberg MJ. Impulse control and related disorders in Parkinson’s disease. Neurodegener Dis. 2013;11:63–71. doi: 10.1159/000341996. [DOI] [PubMed] [Google Scholar]
- Wilding IR, Hardy JG, Davis SS, Melia CD, Evans DF, Short AH, et al. Characterisation of the in vivo behaviour of a controlled-release formulation of levodopa (Sinemet CR) Clin Neuropharmacol. 1991;14:305–321. doi: 10.1097/00002826-199108000-00003. [DOI] [PubMed] [Google Scholar]
- Witjas T, Kaphan E, Azulay JP, Blin O, Ceccaldi M, Pouget J, et al. Nonmotor fluctuations in Parkinson’s disease: frequent and disabling. Neurology. 2002;59:408–413. doi: 10.1212/WNL.59.3.408. [DOI] [PubMed] [Google Scholar]
- Witjas T, Kaphan E, Azulay JP. Non-motor fluctuations in Parkinson’s disease. Rev Neurol (Paris) 2007;163:846–850. doi: 10.1016/S0035-3787(07)91470-8. [DOI] [PubMed] [Google Scholar]
- Youdim MB, Bakhle YS. Monoamine oxidase: isoforms and inhibitors in Parkinson’s disease and depressive illness. Br J Pharmacol. 2006;147(Suppl 1):S287–S296. doi: 10.1038/sj.bjp.0706464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zanettini R, Antonini A, Gatto G, Gentile R, Tesei S, Pezzoli G. Valvular heart disease and the use of dopamine agonists for Parkinson’s disease. N Engl J Med. 2007;356:39–46. doi: 10.1056/NEJMoa054830. [DOI] [PubMed] [Google Scholar]
- Zesiewicz TA, Sullivan KL, Arnulf I, Chaudhuri KR, Morgan JC, Gronseth GS, Quality Standards Subcommittee of the American Academy of Neurology et al. Practice parameter: treatment of nonmotor symptoms of Parkinson disease: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010;74:924–931. doi: 10.1212/WNL.0b013e3181d55f24. [DOI] [PubMed] [Google Scholar]