

Abstract
Background:
Shoulder instability is a common problem in American football players entering the National Football League (NFL). Treatment options include nonoperative and surgical stabilization.
Purpose:
This study evaluated how the method of treatment of pre-NFL shoulder instability affects the rate of recurrence and the time elapsed until recurrence in players on 1 NFL team.
Design:
Retrospective cohort.
Methods:
Medical records from 1980 to 2008 for 1 NFL team were reviewed. There were 328 players included in the study who started their career on the team and remained on the team for at least 2 years (mean, 3.9 years; range, 2-14 years). The history of instability prior to entering the NFL and the method of treatment were collected. Data on the occurrence of instability while in the NFL were recorded to determine the rate and timing of recurrence.
Results:
Thirty-one players (9.5%) had a history of instability prior to entering the NFL. Of the 297 players with no history of instability, 39 (13.1%) had a primary event at a mean of 18.4 ± 22.2 months (range, 0-102 months) after joining the team. In the group of players with prior instability treated with surgical stabilization, there was no statistical difference in the rate of recurrence (10.5%) or the timing to the instability episode (mean, 26 months) compared with players with no history of instability. Twelve players had shoulder instability treated nonoperatively prior to the NFL. Five of these players (41.7%) had recurrent instability at a mean of 4.4 ± 7.0 months (range, 0-16 months). The patients treated nonoperatively had a significantly higher rate of recurrence (P = 0.02) and an earlier time of recurrence (P = 0.04). The rate of contralateral instability was 25.8%, occurring at a mean of 8.6 months.
Conclusion:
Recurrent shoulder instability is more common in NFL players with a history of nonoperative treatment. Surgical stabilization appears to restore the rate and timing of instability to that of players with no prior history of instability.
Keywords: shoulder instability, dislocation, athlete, National Football League
Shoulder instability is a common problem in American football players, with a prevalence of 10% to 14%.2,8 There is a high rate of recurrent dislocation with nonoperative treatment in younger patients.4,6,7,9,12 This has led many surgeons to advocate early operative treatment of young patients with anterior shoulder instability to prevent repeat episodes. Contact and collision athletes are considered high demand and may be at an increased risk for recurrent instability when treated nonoperatively.1 Operative results in these patients have been favorable, with recurrence rates ranging from 3% to 31%.1,3,5,10,11,13-16
The null hypotheses for this study were as follows: (1) There is no difference in the incidence of recurrent instability in professional football players with prior instability treated nonoperatively or with surgical stabilization; (2) there is no difference in the time elapsed until the occurrence of the instability episode in the National Football League (NFL) between these groups.
Materials and Methods
This study was approved by the Institutional Review Board (study no. 2007P002339). A retrospective review of charts was performed for all players who started their career with 1 NFL team and completed at least 2 years with that team during the period ranging from 1980 to 2008. The data included the number of years on the team, history of instability before the NFL, method of treatment, time to instability after entry into the NFL, and contralateral shoulder instability.
The rate of instability was analyzed in players with no instability history prior to the NFL, prior instability treated nonoperatively, and prior instability who underwent surgical stabilization prior to joining the NFL. An assessment of mean time to instability was also performed to determine if previous history and treatment method predict the timing of shoulder instability. In players with shoulder instability prior to entering the NFL, the rate of instability in the contralateral shoulder was calculated to determine if instability in one shoulder predisposes a player to instability in the other shoulder.
Statistical analysis was performed with the statistical software Analyze-it (Leeds, England). Statistical significance was assessed using an unpaired t test, analysis of variance, Fisher exact test, and the chi-square test, depending on the data being compared. A P value of less than 0.05 was considered to be statistically significant.
Results
The player search identified 356 players who completed at least 2 years with 1 NFL team. The charts of 28 players could not be located, leaving 328 players included in this review. The mean length of participation with the team was 3.9 years (range, 2-14 years). Among the 328 players studied, 46 had episodes of shoulder instability while a member of the team (14.0%). Of these 46 players, 31 (9.5%) had instability before entering the NFL. Twelve of these players had been treated nonoperatively and 19 with surgery. Of the 297 players with no prior shoulder instability, 39 (13.1%) had a subluxation or dislocation of the shoulder at an mean of 18.4 ± 22.2 months (range, 0-102 months) into their NFL careers (Table 1). Of the 12 players with shoulder instability before entering the NFL who were treated nonoperatively, 5 (41.7%) had recurrent instability at a mean of 4.4 ± 7.0 months (range, 0-16 months) into their professional career. Of the 19 players with shoulder instability before entering the NFL who were treated with surgical stabilization, 2 (10.5%) had a recurrence at a mean of 26 ± 17.2 months into their career. Statistical analysis revealed that the group with prior instability treated nonoperatively had a significantly higher recurrence rate (41.7% vs 13.1%, P = 0.02) and a shorter time to recurrence (4.4 vs 18.4 months, P = 0.04). There was no significant difference in the recurrence rate or the time elapsed to an instability episode in the group treated with surgical stabilization compared with players with no prior history of instability (10.5% vs 13.1%, P = 0.5; 26.0 vs 18.4 months, P = 0.6) (Figure 1).
Table 1.
Instability rates and timing in National Football League players
| Group | Instability Rate in the NFL (%) | Months to Instability Episode in the NFL |
|---|---|---|
| No instability prior to the National Football League | 13.1 | 18.4 |
| Prior instability treated nonoperatively | 41.7 | 4.4 |
| Prior instability treated with surgical stabilization | 10.5 | 26.0 |
Figure 1.
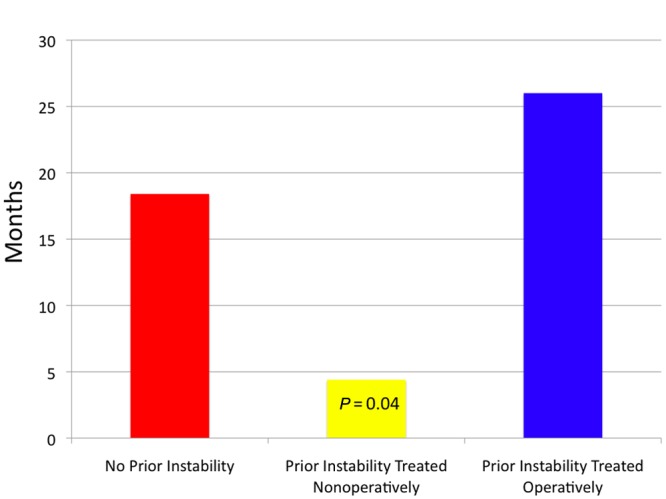
Mean time from entry into the National Football League until recurrent instability. Players with a history of instability prior to entry into the league who were treated nonoperatively had a significantly shorter time until recurrent instability.
In players with instability prior to their NFL career, 8 of 31 players (25.8%) had contralateral instability after a mean period of 8.6 ± 6.7 months (range, 0-16 months). There was no difference in the rate of instability (P = 0.22) or time elapsed to instability episode (P = 0.06) in the contralateral shoulder compared with the group with no prior instability in either shoulder.
Discussion
Four important conclusions may be drawn from this study. In following NFL football players on a single team over a nearly 3-decade period, the rate of shoulder instability was similar to the instability rates of football players evaluated at the NFL combine prior to entry into the league.2,8 Second, the recurrence rate of players with a history of shoulder instability treated nonoperatively is much higher than that in the normal population and much higher than shoulders treated operatively. When treated operatively, recurrent shoulder instability rates in NFL players are similar to players with no history of shoulder instability prior to entry into the NFL. Third, the time from entry into the NFL until the first instability event is much shorter in patients with shoulder instability treated nonoperatively. Finally, players with a history of shoulder instability have a high rate of contralateral shoulder instability while playing in the NFL.
Shoulder instability is a common injury in football players. In a retrospective review of players entering the NFL combine, 9.7% of players had a history of instability and 4.7% had prior shoulder stabilization surgery.2 In a cohort of 336 college players entering the NFL combine, a history of shoulder instability was found in 14% and prior stabilization surgery in 10%.8 These cohorts were analyzed prior to playing in the NFL.
Recurrence of instability is common in young patients treated nonoperatively and may be even more likely in those who return to contact and collision sports. This has led many surgeons to recommend early operative treatment for young high-demand patients with the goal of preventing recurrent episodes.11 Ninety-eight percent (16 of 17) of players in one series were able to return to sports participation. However, there was a higher recurrence rate in football (5% vs 0%).11
A recurrence rate in contact athletes of 31% has been reported with the transglenoid repair technique.14 In 58 football players with shoulder instability treated with open stabilization, 2 had a subluxation postoperatively, and 52 were able to return to play for at least 1 year.13 The 4 NFL players in their series returned to professional play. In 66 collision or contact athletes with shoulder instability treated with open stabilization (transosseous tunnels and suture anchors), 15 patients (23%) had a recurrent subluxation or dislocation.16
Bacilla et al reported on 40 patients with shoulder instability treated with arthroscopic stabilization using suture anchors.1 All were less than 23 years old and in collision or contact sports.1 Ninety-three percent had stable shoulders at a mean follow-up of 30 months, with 3 patients requiring reoperation for recurrent instability.1 Twenty-nine returned to the same level of play or higher at a mean of 6 months.1 In another series, 18 contact athletes with shoulder instability under 20 years of age were treated with arthroscopic stabilization.10 Two patients (11%) had recurrent instability at a mean follow-up of 37 months. Neither required reoperation during the study period.
The limitations of this study are many. This was a retrospective study without a description of the surgical stabilization or the nonoperative approach used. The treatment decision (operative or nonoperative) was not randomized, and the results are therefore subject to selection bias. Additionally, no patient-reported outcome measures were used. There is also recall bias because some players likely underreported instability episodes because of the impact it would have on their career. Furthermore, shoulder instability may have ended the careers of some players prior to the 2 full seasons necessary for inclusion in this study, thus introducing additional selection bias into the results. Finally, although there was no statistical difference between players without instability and those with instability treated with surgery, these groups did not reach statistical power because they were too small.
Conclusion
Shoulder instability is a common condition in football players entering the NFL. Players with prior instability treated nonoperatively have a substantially higher rate of recurrent instability early in their professional careers. Surgical stabilization appears to restore the incidence and timing of recurrence to levels comparable with players with no history of shoulder instability.
Footnotes
The following authors declared potential conflicts of interest: Thomas J. Gill, MD, is a consultant for ConMed Linvatec.
References
- 1. Bacilla P, Field LD, Savoie FH. Arthroscopic Bankart repair in a high demand patient population. Arthroscopy. 1997;13(1):51-60 [DOI] [PubMed] [Google Scholar]
- 2. Brophy RH, Barnes R, Rodeo SA, Warren RF. Prevalence of musculoskeletal disorders at the NFL combine: trends from 1987 to 2000. Med Sci Sports Exerc. 2007;39(1):22-27 [DOI] [PubMed] [Google Scholar]
- 3. Carreira DS, Mazzocca AD, Oryhon J, et al. A prospective outcome evaluation of arthroscopic Bankart repairs: minimum 2-year follow-up. Am J Sports Med. 2006;34(5):771-777 [DOI] [PubMed] [Google Scholar]
- 4. Deitch J, Mehlman CT, Foad SL, Obbehat A, Mallory M. Traumatic anterior shoulder dislocation in adolescents. Am J Sports Med. 2003;31(5):758-763 [DOI] [PubMed] [Google Scholar]
- 5. Gill TJ, Micheli LJ, Gebhard F, Binder C. Bankart repair for anterior instability of the shoulder. Long-term outcome. J Bone Joint Surg Am. 1997;79(6):850-857 [DOI] [PubMed] [Google Scholar]
- 6. Hovelius L. Anterior dislocation of the shoulder in teen-agers and young adults: five-year prognosis. J Bone Joint Surg Am. 1987;69(3):393-399 [PubMed] [Google Scholar]
- 7. Hovelius L, Augustini BG, Fredin H, Johansson O, Norlin R, Thorling J. Primary anterior dislocation of the shoulder in young patients: a ten-year prospective study. J Bone Joint Surg Am. 1996;78(11):1677-1684 [DOI] [PubMed] [Google Scholar]
- 8. Kaplan LD, Flanigan DC, Norwig J, Jost P, Bradley J. Prevalence and variance of shoulder injuries in elite collegiate football players. Am J Sports Med. 2005;33(8):1142-1146 [DOI] [PubMed] [Google Scholar]
- 9. Marans HJ, Angel KR, Schemitsch EH, Wedge JH. The fate of traumatic anterior dislocation of the shoulder in children. J Bone Joint Surg Am. 1992;74(8):1242-1244 [PubMed] [Google Scholar]
- 10. Mazzocca AD, Brown FM, Carreira DS, Hayden J, Romeo AA. Arthroscopic anterior shoulder stabilization of collision and contact athletes. Am J Sports Med. 2005;33(1):52-60 [DOI] [PubMed] [Google Scholar]
- 11. O’Neill DB. Arthroscopic Bankart repair of anterior detachments of the glenoid labrum: a prospective study. J Bone Joint Surg Am. 1999;81(10):1357-1366 [PubMed] [Google Scholar]
- 12. Owens BD, Dawson L, Burks R, Cameron KL. Incidence of shoulder dislocation in the United States military: demographic considerations from a high-risk population. J Bone Joint Surg Am. 2009;91(4):791-796 [DOI] [PubMed] [Google Scholar]
- 13. Pagnani MJ, Dome DC. Surgical treatment of traumatic anterior shoulder instability in american football players. J Bone Joint Surg Am. 2002;84(5):711-715 [DOI] [PubMed] [Google Scholar]
- 14. Pagnani MJ, Warren RF, Altchek DW, Wickiewicz TL, Anderson AF. Arthroscopic shoulder stabilization using transglenoid sutures: a four-year minimum followup. Am J Sports Med. 1996;24(4):459-467 [DOI] [PubMed] [Google Scholar]
- 15. Speer KP, Warren RF, Pagnani M, Warner JJ. An arthroscopic technique for anterior stabilization of the shoulder with a bioabsorbable tack. J Bone Joint Surg Am. 1996;78(12):1801-1807 [DOI] [PubMed] [Google Scholar]
- 16. Uhorchak JM, Arciero RA, Huggard D, Taylor DC. Recurrent shoulder instability after open reconstruction in athletes involved in collision and contact sports. Am J Sports Med. 2000;28(6):794-799 [DOI] [PubMed] [Google Scholar]