

Abstract
Background:
Ankle injuries are the most common high school basketball injury. Little is known regarding the utilization of ankle injury prevention strategies in high school settings.
Objective:
To determine high school basketball coaches’ utilization of ankle injury prevention strategies, including prophylactic ankle bracing (PAB) or an ankle injury prevention exercise program (AIEPP).
Study Design:
Cross-sectional survey.
Methods:
The survey was distributed to all high school basketball coaches in Wisconsin. Fisher exact and Wilcoxon rank sum tests were used to determine if the injury prevention strategies utilized differed according to school size, sex of the team, years of coaching experience, and the coach’s education level.
Results:
Four hundred eighty (55%) coaches from 299 (74%) high schools completed the survey. Thirty-seven percent of the coaches encouraged or required their players to use PAB. School enrollment of the coaches’ teams did not affect their stance on the use of PAB (P = 0.30), neither did the sex of the team (P = 0.16), years coaching (P = 0.09), nor the coach’s education (P = 0.49). Fifty percent (n = 242) of the coaches indicated they do not utilize an AIEPP, with no difference based on school enrollment (P = 0.47), team sex (P = 0.41), years coaching (P = 0.78), or the education level (P = 0.44). Barriers to utilization of AIEPP included a lack of time, awareness, and expertise. Coaches preferred an AIEPP that was specific to basketball, combined injury prevention and performance enhancement components, was performed 2 to 3 days per week, and lasted 5 to 15 minutes.
Conclusion:
Less than half of the coaches encouraged use of PAB, and half did not utilize an AIEPP. Coaches had specific preferences for the type of AIEPP they would implement.
Clinical Relevance:
Sports medicine providers should promote ankle injury prevention strategies but need to address why prevention strategies may not be utilized in high school basketball settings.
Keywords: ankle injury, prevention, high school, basketball
Basketball is one of the most popular sports in the United States. In 2011, nearly 1 million adolescent athletes were members of basketball teams at over 18,000 US high schools.23 Ankle injuries are the most common musculoskeletal injury sustained in high school basketball2 (US Consumers Product Safety Commission, Directorate of Economic Analysis, written communication, September 7, 2012) and impose severe monetary consequences on the US health care system with an estimated $2 billion in total costs spent to treat these injuries in 2010.24 Repeated ankle injuries are associated with development of chronic ankle instability, increased likelihood for the onset of osteoarthritis, decreased levels of physical activity, and lower quality of life.1,9,12,13,17,25 There is an increasing body of evidence that ankle injuries can be prevented in young athletes through the implementation of prophylactic ankle bracing (PAB), which reduces the risk of ankle injury by 50% to 85%,6,19,21 and ankle injury prevention exercise programs (AIPEPs), which reduce the risk of ankle injury by 60% to 85%.4,14,20,22,26
Less well studied is the extent to which ankle injury prevention strategies are actually implemented in adolescent sport settings.18 Information gained from working directly with high school basketball programs for 20 years in various geographic settings showed that the utilization of ankle injury prevention strategies was inconsistent. In addition, previous research in high school settings revealed that factors such as school enrollment or the coaches’ education level may play a role in the incidence of high school sport injuries.16 Experts have highlighted the need to move beyond traditional epidemiologic and prevention studies, with greater emphasis on sports injury prevention implementation strategies and research.8,10,27,28 One of the first steps in the implementation process is to better understand the end user’s perceptions and behaviors regarding injury prevention programming.11 To date, no studies have reported on the attitudes and behaviors of coaches regarding ankle injury prevention strategies. Understanding the current utilization of these strategies and identifying barriers coaches face when trying to implement these strategies in their individual sport settings is crucial for successful implementation in the general sports community.
The objective of this study was to determine high school basketball coaches’ utilization of and attitudes and behaviors toward the use of ankle injury prevention strategies to reduce ankle injuries.
Methods
A cross-sectional survey was distributed electronically to all 868 high school basketball coaches with school-provided e-mail addresses from 402 high schools in Wisconsin during the 2011-2012 basketball season. The survey (see Appendix A, available at http://sph.sagepub.com/content/suppl) was initially developed from key informant interviews with a panel of 12 current and former high school basketball coaches and school athletic administrators. As a result of these interviews, several themes were identified to explore coaches’ attitudes and behaviors regarding ankle injury prevention strategies. With regard to the utilization of braces, members of the panel indicated they would be concerned about the efficacy of ankle braces as well as the possible impact braces would have on athletic performance or other lower extremity injuries. Concerns regarding ankle injury prevention programs included questioned efficacy, lack of awareness these programs existed, the ease of implementation, as well as the components (sport specificity) and formats (duration and days per week) for these programs. The final survey (see Appendix A) contained 42 items and consisted of yes/no and Likert-scaled (eg, strongly agree to strongly disagree) questions and included an area for comments at the end of the survey for coaches to add to or clarify their responses. Face validity of the survey was determined by a committee of medical providers and sports injury researchers with experience working in high school sport settings.
In the survey, lace-up ankle braces were defined as “consisting of fabric or some similar material, may contain additional straps that surround the ankle, are designed to be worn over a pair of socks and laced up the front like a shoe” (Figure 1). An AIPEP was described as “a series of planned, systematic exercises that are designed to prevent ankle, knee, and other lower extremity injuries. Activities may include the following: structured warm-up, stretching, core muscle strengthening, proper take-off and landing techniques, and balance and agility training. These programs are usually performed at the beginning or end of practice, take place 2 to 5 times a week throughout the season, and require 10 to 30 minutes to complete” (Figure 2).
Figure 1.

Lace-up ankle brace.
Figure 2.

Balance training activities.
The reliability (test, retest) of the survey was r = 0.698 and was calculated by administering the survey 2 times 7 to 10 days apart to a convenience sample of 20 current high school basketball coaches. The survey was administered through the Qualtrics Web Survey platform (https://www.qualtrics.com) and sent through the University of Wisconsin Web Hosting Service. Reminder postcards were sent to nonresponders 7 to 10 days following the initial survey request and were followed by a second e-mail solicitation.
Descriptive statistics were used to characterize the sample. Fisher exact and Wilcoxon rank sum tests were used to determine if the recommendation of PAB or the utilization of injury prevention strategies differed according to school size (enrollment), team sex (female vs male), years of coaching experience, and the coach’s education level. Frequencies were used to summarize the coaches’ responses regarding current utilization and beliefs toward the efficacy and/or harm of using lace-up ankle braces, recommendations for PAB, the use of AIPEP, factors that coaches identify as significant barriers to implementation of AIPEP, and formats coaches prefer to use for AIPEP. This study was approved by the University of Wisconsin Health Sciences Minimal Risk Institutional Review Board in December of 2011.
Results
A total of 480 (55%) coaches from 299 (74%) high schools completed the survey. Coaches were split evenly between male and female teams and primarily consisted of head coaches at the varsity level (Table 1). For the purpose of analysis, the school enrollment (range, 52-2251) was stratified into small, medium, and large school groups with equal representation in each group. A minority of coaches encouraged or required their players to use ankle braces (Figure 3). There was no association in PAB recommendations based on school enrollment (P = 0.30), team sex (P = 0.19), years of coaching experience (P = 0.09), or coach’s education level (P = 0.50). The majority of the coaches believed that ankle braces would decrease their players’ risks of sustaining an ankle injury (Figure 4) and that braces would not increase their players’ risks for other lower extremity injuries (Figure 5) or negatively impact their players’ performances (Figure 6).
Table 1.
Coaches’ demographic characteristics (N = 480)
| n (%) | |
|---|---|
| Team Sex | |
| Female | 247 (51.5) |
| Male | 233 (48.5) |
| School enrollment, no. of students | |
| Small (<270) | 160 (33.3) |
| Medium (271 to 759) | 160 (33.3) |
| Large (>760) | 160 (33.3) |
| Coaches’ education level | |
| High school | 36 (7.5 |
| Tech/2-year diploma | 18 (3.7) |
| Bachelor’s degree | 202 (42.0) |
| Graduate degree | 224 (46.6) |
| Coaches’ experience, y | |
| <5 | 85 (3.7) |
| 6-10 | 115 (23.9) |
| 11-15 | 98 (20.4) |
| 16-20 | 62 (12.9) |
| >20 | 116 (24.1) |
Figure 3.

Coaches’ current use of prophylactic ankle bracing (PAB).
Figure 4.

Coaches’ responses to the statement, “Basketball players who routinely use lace-up ankle braces will decrease their risk of sustaining an ankle injury.”
Figure 5.
Coaches’ responses to the statement, “Basketball players who routinely use lace-up braces will increase their risk of sustaining a knee or other leg injury.”
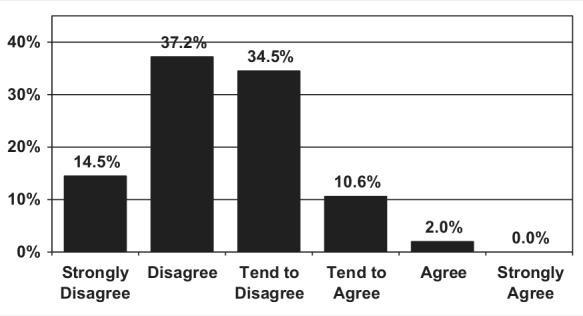
Figure 6.

Coaches’ responses to the statement, “I think that basketball players who routinely use lace-up ankle braces will negatively impact their performance (running speed, agility, and jump height).”
Half of the coaches indicated that they do not utilize an AIPEP. There was no difference in utilization of AIPEP based on school enrollment (P = 0.47), team sex (P = 0.41), years of coaching experience (P = 0.78), or coaches’ education level (P = 0.44). Coaches who did not utilize an AIPEP indicated barriers that included lack of time, expertise, and awareness to implement them (Table 2). Coaches indicated they would prefer programs that were specific to basketball in format and location, consisted of both injury prevention and performance enhancement components, were performed 2 to 3 days per week, lasted 5 to 15 minutes, and used minimal equipment (Table 3).
Table 2.
Common reasons coaches reported for not utilizing an ankle injury prevention exercise program (AIEPP)
| Statement | n (%) |
|---|---|
| I don’t have the time to run this type of program during practice. | 129 (53.3) |
| I (and my staff) don’t have the expertise to run this type of program. | 120 (49.5) |
| I am not aware that these programs exist. | 115 (47.5) |
| Our school does not have the extra space to implement one of these programs. | 92 (38.0) |
| Our players take part in an overall conditioning/performance enhancement type of program in the summer with all of our other high school athletes. | 72 (29.7) |
| Our school does not have the equipment to implement one of these programs. | 62 (25.6) |
| I don’t think that these types of programs will reduce ankle injuries. | 12 (4.9) |
| I used a similar program previously but did not think it helped reduce injuries. | 11 (4.5) |
Table 3.
Coaches’ preferences regarding the format and components of an ankle injury prevention exercise program (AIEPP)a
| Program Formats and Components | n (%) |
|---|---|
| Specificity | |
| Specific to basketball players | 324 (67.5) |
| Not sport specific (generic) | 156 (32.5) |
| Type of program | |
| Combination of performance enhancement and injury prevention | 410 (87.1) |
| Performance enhancement | 36 (7.9) |
| Injury prevention | 24 (4.9) |
| Location of program | |
| Basketball court | 418 (90.4) |
| Multipurpose room | 35 (7.5) |
| Other location | 9 (1.9) |
| Type of equipment needed | |
| Minimal (rubber cords, cones, athletic tape) | 308 (64.4) |
| Extensive (weights, hurdles, step boxes) | 106 (21.8) |
| None | 66 (13.6) |
| Duration, min | |
| 5-10 | 165 (34.3) |
| 11-15 | 226 (47.4) |
| 16–20 | 78 (16.3) |
| >20 | 11 (2.3) |
| Days per week program would be performed | |
| 1 | 31 (6.4) |
| 2 | 189 (39.4) |
| 3 | 169 (35.8) |
| 4 to 5 | 90 (18.8) |
Columns may not add up to 480 since all respondents did not answer each question.
Discussion
The purpose of this study was to determine the utilization, attitudes, and behaviors of high school basketball coaches toward ankle injury prevention strategies. The primary finding is that these strategies are underutilized in this study sample. Understanding how prevalent the use of injury prevention strategies is as well as reasons for their disuse is an essential first step to increasing the utilization of these programs in school settings7 and making it more likely that injury prevention strategies will be successfully implemented in sport settings.7,8,28
This study illustrated that the majority of coaches surveyed thought lace-up ankle braces are effective in reducing the risk of ankle injuries but do not increase the risk for other lower extremity injuries or negatively impact performance. These attitudes are in agreement with recent findings on the efficacy of lace-up ankle braces21 as well as research that shows a limited effect on knee kinematics5 and athletic performance.3 Despite these positive attitudes regarding ankle bracing, only one third of the coaches encouraged or required ankle brace use in their players. The rationale for this behavior was not specifically measured. However, several coaches indicated in written comments that they did not feel comfortable recommending braces because they did not know which specific brand was best for their athletes. Other coaches indicated that they were unsure where to purchase ankle braces or were concerned about the associated costs ($40 to $60 per pair).
Similar to low ankle brace use, a significant number of coaches also did not utilize an AIPEP, citing factors such as a lack of time, space, awareness, and expertise to run these programs. Lack of time and space should not be underestimated as significant barriers affecting the implementation of AIPEP. With regard to time, several coaches indicated that they were only allotted 100 to 120 minutes of court time per day and therefore felt they could not give up 10 to 20 minutes of that time to have players perform an AIPEP. With regard to space limitations, 1 high school athletic administrator from a large school in a rural setting commented that they have only 1 large wooden court available for all 6 of the school’s basketball teams (3 each for both the male and female teams), and as a result, each team’s time spent on the court is tightly scheduled throughout the season.
Almost half of the coaches who did not utilize an AIPEP cited a lack of awareness or expertise to utilize these programs. This result is enlightening, since a recent 2010 review14 found that neuromuscular training would reduce the risk of ankle sprains (relative risk [RR] = 0.50, 95% confidence interval [CI], 0.31–0.79), acute knee injuries (RR = 0.46, 95% CI, 0.28–0.76), or lower limb injuries (RR = 0.61, 95% CI, 0.49–0.77) in adolescent and young adult athletes. This type of disconnect has been mentioned by Finch8 and Verhagen et al,27 who emphasize that rigorous scientific sports injury research does not necessarily ensure the widespread use of these effective interventions by the targeted population in the real world.
It should also be noted that providing expertise to basketball coaches regarding prevention programming may not be enough to have them implement these programs for their teams. In one study, the authors offered to instruct and provide equipment for a group of coaches in an urban setting and found that nearly two thirds declined to participate because of a lack of time and/or interest.17 Coaches in this study were provided with the expertise needed to implement the programs but still did not participate. This finding illustrates that working with individual coaches alone may not ensure injury prevention as a priority. Instead, a concerted effort may have to be made at the sport association level down through the school administration to the individual coaches as well as parents and athletes. In this manner, injury prevention may be thought of as an integral component of offering an interscholastic basketball program.
Learning about the formats and components of an AIPEP preferred by coaches may be key to the successful implementation of these programs. Our results showed that coaches had strong preferences for the AIPEP formats they would be willing to implement for their teams (Table 3). Hübscher et al13 reviewed 7 papers (2 that included basketball players) on the effect of neuromuscular training and reported that the programs were implemented up to 6 months prior to the sport season and consisted of exercises performed from 1 to 7 days per week for 15 to 30 minutes per session. A 2010 review by Zech et al28 on balance training for neuromuscular control and performance enhancement also found that the training protocols varied considerably in the time (5 to 90 minutes per day) and the number of days (2 to 7 days) per week. In addition, many of the injury prevention programs focused solely on balance training with limited demonstrable improvement in basketball-related performance (speed, agility, or vertical jump height).
The findings that coaches preferred programs that require minimal equipment are interesting because this may indicate that sports medicine providers need to emphasize that a minimal level of equipment (at low cost) can be utilized effectively. The injury prevention interventions cited by Hübscher et al13 utilized minimal (balance boards) or no equipment (stretching, hopping, and landing techniques). Ideally, sports medicine providers should be able to cite data that show the change in the effectiveness (reduction of injury incidence) of injury prevention strategies performed 1 or 2 days per week with those performed 4 to 5 days per week. Likewise, data that show the difference in injury prevention programming with no, limited, or extensive equipment usage may make it more likely that specific injury prevention strategies are implemented in high school basketball settings. However, to the authors’ knowledge, these comparative data do not exist at this time.
Implications for Researchers
Much of the sports medicine research has focused on intervention strategies, with little attention placed on implementation strategies.15,20 Incorporating coach-directed preferences for ankle injury prevention strategies may enhance injury prevention research through the design of strategies that are more relevant, practical, and applicable in the real world.11 If shorter programs are found to be just as effective in reducing injury and improving performance, they may be more likely to be adopted in real-world sport settings and may improve the likelihood that ankle injury prevention strategies are widely implemented in secondary school settings. Understanding the rationale for coaches’ beliefs regarding their injury prevention preferences would also be worthwhile.
Limitations
There are several limitations to this study. First, the study participants were solely Wisconsin high school coaches. While the demographics of the subjects varied a great deal, they may not be representative of coaches across the United States. Second, respondents consisted almost exclusively of varsity coaches instead of equal numbers of subvarsity or freshman-level coaches. Finally, subjects were not asked if they had received any previous education on injury prevention strategies for high school basketball players as part of their training as coaches. This information would shed more light on factors that influenced whether a coach utilized ankle bracing or an AIPEP.
Conclusion
A majority of coaches did not actively encourage their players to use lace-up ankle braces despite believing that they would reduce the risk of ankle injuries. Half of the coaches did not utilize an ankle injury prevention program, citing a lack of time, awareness, expertise, and space to implement these programs.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this manuscript.
References
- 1. Anandacoomarasamy A, Barnsley L. Long term outcomes of inversion ankle injuries. Br J Sports Med. 2005;39:e14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Borowski LA, Yard EE, Fields SK, Comstock RD. The epidemiology of US high school basketball injuries, 2005-2007. Am J Sports Med. 2008;36:2328-2335 [DOI] [PubMed] [Google Scholar]
- 3. Cordova ML, Ingersoll CD, Palmieri R. Efficacy of prophylactic ankle support: an experimental perspective. J Athl Train. 2002;37:446-457 [PMC free article] [PubMed] [Google Scholar]
- 4. Cumps E, Verhagen E, Meeusen R. Efficacy of a sports specific training programme on the incidence of ankle sprains in basketball. J Sports Sci Med. 2007;6:212-219 [PMC free article] [PubMed] [Google Scholar]
- 5. DiStefano LJ, Padua D, Brown C, Guskiewicz K. Lower extremity kinematics and ground reaction forces after prophylactic lace-up ankle bracing. J Athl Train. 2008;43:234-241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Dizon JM, Reyes JJ. A systematic review on the effectiveness of external ankle supports in the prevention of inversion ankle sprains among elite and recreational players. J Sci Med Sport. 2010;13:309-317 [DOI] [PubMed] [Google Scholar]
- 7. Doll L, Bonzo S, Mercy J, et al. Dissemination, implementation, and widespread use of injury prevention interventions. In: Doll L, Bonzo S, Mercy J, Sleet D. eds. Handbook of Injury and Violence Prevention. New York: Springer; 2007 [Google Scholar]
- 8. Finch C. No longer lost in translation: the art and science of sports injury prevention implementation research. Br J Sports Med. 2011;45:1253-1257 [DOI] [PubMed] [Google Scholar]
- 9. Gerber JP, Williams GN, Scoville CR, Arciero RA, Taylor DC. Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int. 1998;19:653-660 [DOI] [PubMed] [Google Scholar]
- 10. Hanson D, Finch C, Allegrante J, Sleet D. Closing the gap: progression from injury prevention research to safety promotion practice. Inj Prev. 2012;18:A8-A9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Herman K, Barton C, Malliaras P, Morrissey D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: a systematic review. BMC Med. 2012;10:75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hertel J. Functional instability following lateral ankle sprain. Sports Med. 2000;29:361-371 [DOI] [PubMed] [Google Scholar]
- 13. Hübscher M, Zech A, Pfeifer K, Hänsel F, Vogt L, Banzer W. Neuromuscular training for sports injury prevention: a systematic review. Med Sci Sports Exerc. 2010;42:413-421 [DOI] [PubMed] [Google Scholar]
- 14. Klügl M, Shrier I, McBain K, et al. The prevention of sport injury: an analysis of 12,000 published manuscripts. Clin J Sport Med. 2010;20:407-412 [DOI] [PubMed] [Google Scholar]
- 15. Knowles SB, Marshall SW, Miller T, et al. Cost of injuries from a prospective cohort study of North Carolina high school athletes. Inj Prev. 2007;13:416-421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. LaBella CR, Huxford MR, Grissom J, Kim K-Y, Peng J, Christoffel KK. Effect of neuromuscular warm-up on injuries in female soccer and basketball athletes in urban public high schools: cluster randomized controlled trial. Arch Pediatr Adolesc Med. 2011;165:1033-1040 [DOI] [PubMed] [Google Scholar]
- 17. Marchi AG, Di Bello D, Messi G, Gazzola G. Permanent sequelae in sports injuries: a population based study. Arch Dis Child. 1999;814:324-328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. McGuine T. Sports injuries in high school athletes: a review of injury-risk and injury-prevention research. Clin J Sport Med. 2006;16:488-499 [DOI] [PubMed] [Google Scholar]
- 19. McGuine TA, Brooks MA, Hetzel SJ. The effect of lace-up ankle braces on injury rates in high school basketball players. Am J Sports Med. 2011;39:1840-1848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. McGuine TA, Keene JS. The effect of a balance training program on risk of ankle injury in high school athletes. Am J Sports Med. 2006;34:1103-1111 [DOI] [PubMed] [Google Scholar]
- 21. McKeon PO, Mattacola CG. Interventions for the prevention of first time and recurrent ankle sprains. Clin Sports Med. 2008;27:371-382 [DOI] [PubMed] [Google Scholar]
- 22. National Federation of State High School Associations 2011-2012 athletics participation summary. http://www.nfhs.org/content.aspx?id=3282 Accessed October 23, 2012
- 23. Nelson AJ, Collins CC, Yard EE, Fields SK, Comstock RD. Ankle injuries among United States high school sports athletes, 2005-2006. J Athl Train. 2007;42:381-387 [PMC free article] [PubMed] [Google Scholar]
- 24. Valderrabano V, Hintermann B, Horisberger M, Fung T. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006;34:612-620 [DOI] [PubMed] [Google Scholar]
- 25. Verhagen EA, Bay K. Optimising ankle sprain prevention: a critical review and practical appraisal of the literature. Br J Sports Med. 2010;44:1082-1088 [DOI] [PubMed] [Google Scholar]
- 26. Verhagen EA, Finch C. Setting our minds to implementation. Br J Sports Med. 2011;45:1015-1016 [DOI] [PubMed] [Google Scholar]
- 27. Verhagen EA, van Stralen MM, van Mechelen W. Behaviour, the key factor for sports injury prevention. Sports Med. 2010;40:899-906 [DOI] [PubMed] [Google Scholar]
- 28. Zech A, Hübscher M, Vogt L, Banzer W, Hänsel F, Pfeifer K. Balance training for neuromuscular control and performance enhancement: a systematic review. J Athl Train. 2010;45:392-403 [DOI] [PMC free article] [PubMed] [Google Scholar]