

Abstract
Eruptive vellus hair cysts were first described in 1977. They usually appear as yellow to reddish-brown papules on the chest. Usual onset is between ages 17 and 24 years, but they may be congenital. Some believe that they may be inherited as an autosomal dominant disorder. Histologically the cyst has a stratified squamous epithelium and it contains laminated keratin and vellus hairs. They are felt to be caused by an abnormality at the infundibular level of the vellus hair. We present this because of this patient's unusual distribution of eruptive vellus hair cysts.
Keywords: Eruptive vellus hair cyst, infundibular cyst, steatocystoma multiplex
INTRODUCTION
Eruptive vellus hair cyst (EVHC) represents developmental abnormality of vellus hair follicle. Cysts are characteristically located in the mid dermis and contain variable amount of laminated keratin and multiple transversally and obliquely cut vellus hair. We are reporting a case of EVHC in young female presenting as asymptomatic papules on flexor aspect of upper extremities.
CASE REPORT
A 12-year-old female presented with multiple, asymptomatic skin lesions on flexor aspect of both upper extremities since 6 months. Lesions used to heal with postinflammatory hyperpigmentation. Physical examination revealed discrete, symmetrically distributed, 2-3 mm sized, dome-shaped hyperpigmented follicular papules, few of them with central crust, on flexor aspect of both upper extremities [Figure 1]. There was no family history of similar lesions. Oral and genital examination was normal. Differential diagnosis of eruptive vellus hair cyst, milia was considered.
Figure 1.

Multiple hyperpigmented follicular papules on flexural aspect of forearm
Biopsy of the papule showed a mid-dermal cyst lined by flattened squamous epithelium [Figure 2]. The cyst cavity contained abundant laminated keratinous material and varying numbers of transversely and obliquely cut vellus hair shafts [Figure 3]. Thus diagnosis of Eruptive vellus hair cyst was confirmed. We started the patient on topical retinoic acid cream (0.05%) daily at night with complete resolution of lesions, but few lesions recurred after stopping the treatment.
Figure 2.
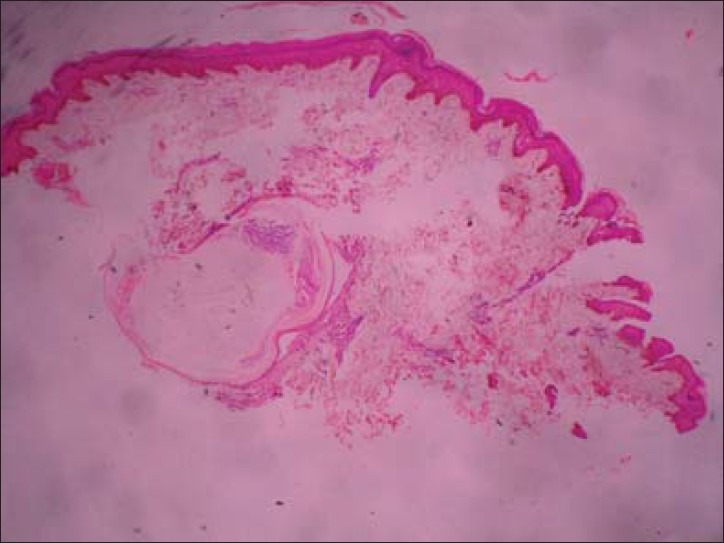
Mid dermal cyst lined by flattened squamous epithelium [H & E, 10X]
Figure 3.
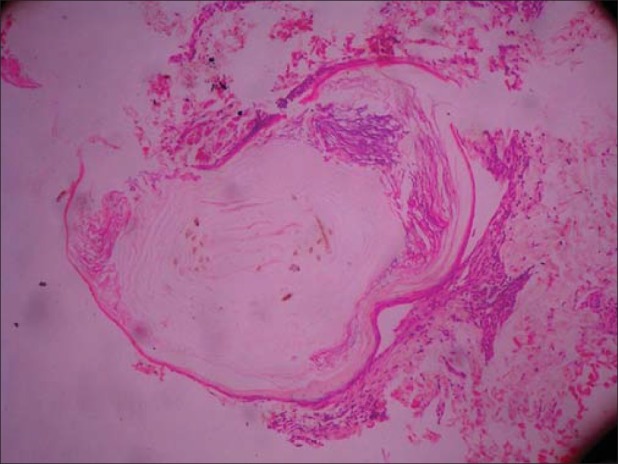
Cyst cavity containing laminated keratinous material and varying numbers of transversely and obliquely cut vellus hair shafts [H & E, 100X]
DISCUSSION
Eruptive vellus hair cysts (EVHCs) were first described by Esterly, Fretzin, and Pinkus in 1977.[1] The exact cause of EVHC is unknown; some consider it to be a hamartoma differentiating toward vellus hair while some believe that it is an unusual developmental abnormality of vellus hair follicles predisposing them to occlusion at the level of infundibulum, resulting in retention of hair, cystic dilatation of proximal part of the follicle and secondary atrophy of the hair bulbs.
EVHCs can be sporadic in occurrence, in which case they appear without any antecedent trauma in the first or second decade of life. They may occur in an autosomal dominant inheritance pattern with lesions appearing at birth or in early infancy.[2] There is no sex predilection. They most commonly present as multiple small, dome shaped papules, 1-4 mm in diameter, with colors ranging from skin colored, yellow, blue, red or hyperpigmented. They may be topped with central hyperkeratotic crust, puncta, and umbilication. Generally they are asymptomatic, but they may be associated with itching and tenderness occasionally. Common sites of involvement are anterior chest, abdomen, and extremities.[3] Lesions may also occur on face, neck, axillae, and groins.
Histologically, EVHCs are characteristically located in the mid dermis. The epithelium lining cyst wall is identical to infundibular or sometimes isthmus portion of the hair follicle and contains two or three layers of squamous epithelium with focal areas of granular layer. The cyst cavity contains variable amount of laminated keratin and multiple transversally and obliquely cut vellus hair.[3] The cyst wall may be in continuity with a rudimentary hair follicle or arrector pilli muscle. Generally, no sebaceous glands are present in the cyst wall. Occasionally the cyst may be surrounded by granulomatous inflammation, causing partial destruction of the cyst wall. The differential diagnosis of pilosebaceous cysts includes infundibular cysts, steatocystoma multiplex, and EVHCs. All three commonly affect the anterior chest wall and consist of asymptomatic papules or nodules. Obstructed or occluded follicles form the common infundibular cysts. These do not contain sebaceous glands or vellus hairs. The cysts of steatocystoma multiplex (SM) arises in the sebaceous duct and has a crenulated, eosinophilic, hyaline lining to the cyst wall where the granular layer is absent. Steatocystomas also contain sebaceous glands arising within the cyst wall.[4] Some authors believe that EVHC and steatocystoma multiplex are variants of the same disorder because both lesions have been reported in the same patient,[5] while other authors consider them as distinct entities based on different histologic patterns. Tamokova et al. 0 revealed, through staining with K 10 and K17, that EVHC and SM were two distinct entities.[6]
Other clinical differential diagnosis include comedones, keratosis pilaris, perforating folliculitis, syringoma, milia, and mollluscum contagiosum.[7] Histological examination is often essential to differentiate these lesions from EVHC.
A simple, rapid diagnostic test has been described in which the contents of the cyst were expressed and microscopic examination of the expressed contents in potassium hydroxide preparation shows numerous vellus hairs.[4,8] Associations of EVHCs with eccrine poromas, sebaceous adenomas, anhidrotic ectodermal dysplasia, hidrotic ectodermal dysplasia, pachyonychia congenita have been reported.[9]
Most lesions persist if untreated, but in some cases (approximately in 25% cases) spontaneous resolution (due to transepidermal elimination of cyst contents) may occur. Patients generally seek medical advice for cosmetic reasons.
Treatment modalities include incision and drainage, needle evacuation using 18 gauge needle after local anesthesia with topical anesthetic cream, application of topical keratolytic agents such as retinoic acid (0.05%), tazarotene cream (0.1%), urea (10%) or lactic acid (12%), as well as CO2 or Erbium YAG LASER ablation. Topical calcipotriene showed partial response in one case[10] as opposed to oral isotretinoin (1 mg/kg/day) and systemic vitamin A therapy which failed to show any clinical improvement.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Esterly NB, Fretzin DF, Pinkus H. Eruptive vellus hair cysts. Arch Dermatol. 1977;113:500–3. [PubMed] [Google Scholar]
- 2.Stiefler RE, Bergfeld WF. Eruptive vellus hair cysts–An inherited disorder. J Am Acad Dermatol. 1980;3:425–9. doi: 10.1016/s0190-9622(80)80338-0. [DOI] [PubMed] [Google Scholar]
- 3.Rao R, Balachandran C. Asymptomatic papular lesions on the trunk. Indian J Dermatol Venereol Leprol. 2009;75:217–9. doi: 10.4103/0378-6323.48687. [DOI] [PubMed] [Google Scholar]
- 4.Karen JK, Heller M, Wee SA, Mikkilineni R. Eruptive vellus hair cysts. Dermatol Online J. 2007;13:14. [PubMed] [Google Scholar]
- 5.Kiene P, Hauschild A, Christophers E. Eruptive vellus hair cysts and steatocystoma multiplex. variants of one entity? Br J Dermatol. 1996;134:365–7. [PubMed] [Google Scholar]
- 6.Tomková H, Fujimoto W, Arata J. Expression of keratins (K10 and K17) in steatocystoma multiplex, eruptive vellus hair cysts, and epidermoid and trichilemmal cysts. Am J Dermatopathol. 1997;19:250–3. doi: 10.1097/00000372-199706000-00008. [DOI] [PubMed] [Google Scholar]
- 7.Reep MD, Robson KJ. Eruptive vellus hair cysts presenting as multiple periorbital papules in a 13-year-old boy. Pediatr Dermatol. 2002;19:26–7. doi: 10.1046/j.1525-1470.2002.00009.x. [DOI] [PubMed] [Google Scholar]
- 8.Karadag AS, Cakir E, Pelitli A. Eruptive vellus hair cysts: An alternative diagnosing method. Indian J Dermatol Venereol Leprol. 2009;75:537–8. doi: 10.4103/0378-6323.55421. [DOI] [PubMed] [Google Scholar]
- 9.Romiti R, Festa Neto C. Eruptive vellus hair cysts in a patient with ectodermal dysplasia. J Am Acad Dermatol. 1997;36:261–2. doi: 10.1016/s0190-9622(97)70294-9. [DOI] [PubMed] [Google Scholar]
- 10.Erkek E, Kurtipek GS, Duman D, Sanli C, Erdoðan S. Eruptive vellus hair cysts: Report of a pediatric case with partial response to calcipotriene therapy. Cutis. 2009;84:295–8. [PubMed] [Google Scholar]