

Abstract
Woolly hair is a congenital abnormality of scalp hair manifesting as short, kinked hair, which may also involve the hair over the other parts of the body. Keratosis pilaris has been a well known association of woolly hair, and can also be a part of the Naxos or Carvajal syndromes. We herein present a case of woolly hair with associated keratosis pilaris, canaliform dystrophy of nails, increased interdental spaces and recurrent bullous impetigo. Although keratosis pilaris and teeth abnormalities have been reported as isolated associations with woolly hair, such a combination of findings as seen in our patient has not been reported before.
Keywords: Bullous impetigo, keratosis pilaris, woolly hair
INTRODUCTION
Woolly hair is a rare, congenital structural abnormality of scalp hair. The rate of hair growth is usually normal but the anagen phase is truncated, resulting in shorter hair. The hair shaft exhibits elliptical cross section, axial rotation and kink formation. There are mainly two types of woolly hair; the autosomal dominant woolly hair, also called hereditary woolly hair, and the less commoner autosomal recessive familial woolly hair. We herein describe a case of woolly hair with associated keratosis pilaris, periodontal changes, canaliform dystrophy of nails and recurrent bullous impetigo. Such a combination of findings has not been previously reported in literature.
CASE REPORT
A 4-year-old boy, product of third degree consanguineous marriage, presented with history of light colored curly hair on the scalp and skin-colored pinhead type of raised lesions over the body since birth. The skin lesions began on the scalp and later spread to the whole body. He also gave a history of recurrent pus-filled lesions over the body since the age of 3 months. There was no delay in developmental milestones.
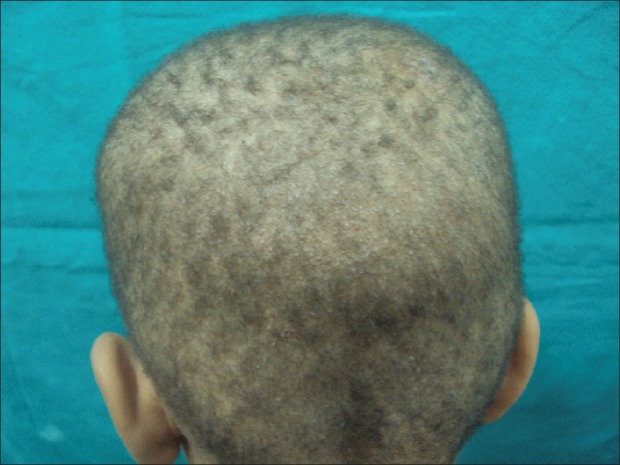
Examination revealed curled hypopigmented scalp hair [Figure 1]. The scalp hairs were short and thinner in diameter. The body hair was also sparse, shorter and lighter in color. Multiple skin colored, spiny follicular papules were present over his scalp, back and arms [Figures 2 and 3]. The eyebrows had sparse hair. Multiple bullae were present over his extremities, some of which were filled with yellow fluid with a positive hypopyon sign [Figure 4]. There was canaliform dystrophy of the bilateral great toe nails [Figure 5]. Dental examination revealed increased interdental spaces and dental caries [Figure 6]. Eye examination was normal. There were no cardiac manifestations or any other systemic involvement.
Figure 1.

Woolly hair on the scalp with sparse eyebrow hair
Figure 2.
Keratosis pilaris lesions on the scalp
Figure 3.

Keratosis pilaris lesions on the trunk
Figure 4.

Bullous impetigo lesions on the forearms
Figure 5.

Canaliform dystrophy of bilateral toe nails
Figure 6.

Dental caries with increased interdental spaces
Investigations revealed normal hematological and biochemical parameters. Skin biopsy of the keratotic papules revealed features consistent with keratosis pilaris [Figure 7]. Gram stain of pus from the bullous lesion revealed gram positive cocci, and the culture grew Staphylococcus aureus. Microscopy of hair revealed an elliptical cross-section, axis rotation and calibre variation. There was no evidence of trichorrhexis nodosa. X-ray chest, electrocardiogram and echocardiography were normal.
Figure 7.
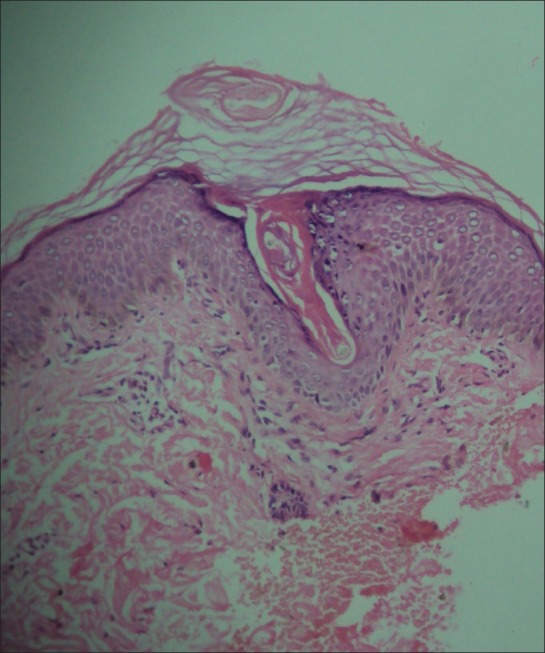
Histopathology of keratosis pilaris lesion revealing characteristic features [H & E, 40×]
DISCUSSION
Woolly hair is a rare congenital abnormality of the structure of scalp hair. It was first described by Gossage in 1907 in an European family.[1] Woolly hair is extremely curly, with the average diameter of hair recorded up to a maximum of 0.5 cm. It is different from the curly hair of black people, in that the curled hair of black people lies separately while the curls of woolly hair usually merge.[2,3]
Woolly hair can appear as a part of systemic disease (Woolly hair syndrome) or without systemic findings (non-syndromic woolly hair). Non syndromic wooly hair can be inherited as either an autosomal dominant or recessive disorder. An earlier classification has described four types of woolly hair: hereditary woolly hair, familial woolly hair, symmetrical circumscribed allotrichia and woolly hair nevus.[4]
Our patient, in addition to woolly hair, had widespread keratosis pilaris (involving the scalp, trunk and upper extremities), canaliform dystrophy of bilateral toe nails, dental changes in the form of increased interdental spaces and dental caries and recurrent bullous impetigo.
Autosomal dominant woolly hair has been reported in six generations of a German family. A dominant form of woolly hair has also been reported in an English family with associated ichthyosis and deafness.[5] Additional features in a Dutch family with woolly hair included dental caries, acral keratoderma and facial abnormalities.[6] A case of woolly hair with keratosis follicularis spinulosa decalvans, teeth abnormalities, scarring alopecia and ophthalmological abnormalities has also been reported. The dental abnormalities included agenesis, inclusions and malformed teeth.[7] Another case of woolly hair associated with pachyonychia congenita, nail changes in the form of yellowish brown hypertrophy and wedge-shaped subungual hyperkeratosis of all 20 nails with natal teeth has been reported.[8] A case similar to ours, but without the nail and teeth findings, has been described earlier by Devinder et al.[9]
Two characteristic associations of woolly hair are Naxos disease and Carvajal disease. Naxos disease is characterised by woolly hair, palmoplantar keratoderma and dilated cardiomyopathy with right ventricular dysplasia.[10] It is an autosomal-recessive disorder occurring due to mutation in the plakoglobin gene.[11] Carvajal disease is similar clinically to Naxos disease, except for left ventricular involvement and presentation at a younger age, and it is due to mutation in the desmoplakin gene.[12]
Acquired woolly hair occurs most commonly in the context of patterned hair loss. It may also be caused by drugs like valproate and retinoids.[13] Our patient did not have any cardiac involvement and there was no history of any drug intake prior to onset of lesions.
To the best of our knowledge, woolly hair with a combination of associated findings in the form of keratosis pilaris, canaliform dystrophy of nails, dental changes and recurrent bullous impetigo occurring together has not been reported earlier in literature.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
REFERENCES
- 1.Gossage AM. The inheritance of certain human abnormalities. Quartz J Med. 1907;1:331–47. [Google Scholar]
- 2.Mohr OL. Woolly hair a dominant mutant characteristic in man. J Hered. 1932;23:345–52. [Google Scholar]
- 3.Schokking CP. Another woolly hair mutation in man. J Hered. 1934;25:337–40. [Google Scholar]
- 4.Hutchison PE, Cairns RJ, Wells RS. Woolly hair. Trans St John's Hosp Dermatol Soc. 1974;60:160–76. [PubMed] [Google Scholar]
- 5.Verbov J. Woolly hair-study of a family. Dermatologica. 1978;157:42–7. doi: 10.1159/000250807. [DOI] [PubMed] [Google Scholar]
- 6.Van Steensel MA, Koedam MI, Swinkels OQ, Rietveld F, Steijlen PM. Woolly hair, premature loss of teeth, nail dystrophy, acral hyperkeratosis and facial abnormalities: Possible new syndrome in a Dutch kindred. Br J Dermatol. 2001;145:157–61. doi: 10.1046/j.1365-2133.2001.04303.x. [DOI] [PubMed] [Google Scholar]
- 7.Lacarrubba F, Dall’Oglio F, Rossi A, Schwartz RA, Micali G. Familial keratosis follicularis spinulosa decalvans associated with woolly hair. Int J Dermatol. 2007;46:840–3. doi: 10.1111/j.1365-4632.2007.03162.x. [DOI] [PubMed] [Google Scholar]
- 8.Ehsani A, Moeineddin F, Rajaee A. Pachyonychia congenita with woolly hair in a ten month old infant. Indian J Dermatol Venereol Leprol. 2008;74:485–6. doi: 10.4103/0378-6323.44306. [DOI] [PubMed] [Google Scholar]
- 9.Thappa DM, Thadeus J, Garg BR. Wooly Hair. Ind J Dermatol. 1995;40:181–3. [Google Scholar]
- 10.Protonotarios N, Tsatsopoulou A, Patsourakos P, Alexopoulos D, Gezerlis P, Simitsis S, et al. Cardiac abnormalities in familial palmoplantar keratosis. Br Heart J. 1986;56:321–6. doi: 10.1136/hrt.56.4.321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McKoy G, Protonotarios N, Crosby A, Tsatsopoulou A, Anastasakis A, Coonar A, et al. Identification of a deletion in plakoglobin in arrhythmogenic right ventricular cardiomyopathy with palmoplantar keratoderma and woolly hair (Naxos disease) Lancet. 2000;355:2119–24. doi: 10.1016/S0140-6736(00)02379-5. [DOI] [PubMed] [Google Scholar]
- 12.Norgett EE, Hatsell SJ, Carvajal-Huerta L, Cabezas JC, Common J, Purkis PE, et al. Recessive mutation in desmoplakin disrupts desmoplakin-intermediate filament interactions and causes dilated cardiomyopathy, woolly hair and keratoderma. Hum Molec Genet. 2000;9:2761–6. doi: 10.1093/hmg/9.18.2761. [DOI] [PubMed] [Google Scholar]
- 13.Bunker CB, Maurice PD, Dowd PM. Isotretinoin and curly hair. Clin Exp Dermatol. 1990;15:143–5. doi: 10.1111/j.1365-2230.1990.tb02053.x. [DOI] [PubMed] [Google Scholar]