

Abstract
Changes in sexual behavior have resulted in longer periods of multiple serial or concurrent relationships. This study investigated the effects of multiple heterosexual partners on mental health, specifically, whether higher numbers of partners were linked to later anxiety, depression, and substance dependency. Data from the Dunedin Multidisciplinary Health and Development Study, a prospective, longitudinal study of a birth cohort born in 1972–1973 in Dunedin, New Zealand were used. The relationship between numbers of sex partners over three age periods (18–20, 21–25, and 26–32 years) and diagnoses of anxiety, depression, and substance dependence disorder at 21, 26, and 32 years were examined, using logistic regression. Interaction by gender was examined. Adjustment was made for prior mental health status. There was no significant association between number of sex partners and later anxiety and depression. Increasing numbers of sex partners were associated with increasing risk of substance dependence disorder at all three ages. The association was stronger for women and remained after adjusting for prior disorder. For women reporting 2.5 or more partners per year, compared to 0–1 partners, the adjusted odd ratios (and 95 % CIs) were 9.6 (4.4–20.9), 7.3 (2.5–21.3), and 17.5 (3.5–88.1) at 21, 26, and 32 years, respectively. Analyses using new cases of these disorders showed similar patterns. This study established a strong association between number of sex partners and later substance disorder, especially for women, which persisted beyond prior substance use and mental health problems more generally. The reasons for this association deserve investigation.
Keywords: Sex partners, Sexual behavior, Anxiety, Depression, Substance use
Introduction
Changes in heterosexual behavior in many countries since the 1960s have been characterized by a decline in the age at first intercourse and an increase in age at first parenthood. Consequently, the period of multiple serial or concurrent sexual relationships has lengthened, especially for women(Johnson, Wadsworth, Wellings, & Field, 1994). Data from the U.S. National Survey of Family Growth has shown an increase in numbers of sexual partners from 1988 to 2002, despite a recent stabilization in age at first intercourse (Aral, 2006). Although sexual risk taking is a feature of young adulthood (CDC, 2005), the psychological effects of this contemporary pattern of sexual behavior are uncertain.
Cross-sectional studies have shown a link between sexual risk taking (e.g., early age at first intercourse, multiple partners, and lack of condom use) and mental health problems in clinical and population samples (e.g., Bachanas et al., 2002; Baskin-Sommers & Sommers, 2006; Brown et al., 2006; Erbelding, Hummel, Hogan, & Zenlman, 2001; Hutton, Lyketsos, Zenilman, Thompson, & Erbelding, 2004; Lavan & Johnson, 2002; Mazzaferro et al., 2006; Mota, Cox, Katz, & Sareen, 2010). Studies addressing the directionality of this association have mainly focussed on mental health problems resulting in sexual risk taking (e.g., Boden, Fergusson, & Horwood, 2010; Bohon, Garber, & Horowitz, 2007; Brook, Balka, & Whiteman, 1999; Dishion, 2000; Duncan, Strycker, & Duncan, 1999). There is evidence from these studies that alcohol or substance use as well as antisocial behavior in childhood and adolescence predicts risky sexual behavior. The few studies that have examined whether sexual risk taking results in mental health problems found early sex and sexually transmitted infections (STIs) associated with later depression and substance problems (e.g., Cornelius, Clark, Reynolds, Kirisci, & Tarter, 2007; Hallfors, Waller, Bauer, Ford, & Halpern, 2005; McGue & Iacono, 2005; Shrier, Harris, & Beardslee, 2002).
Sexual risk taking generally refers to patterns of sexual behavior that put individuals and their sexual partner at greater risk of STIs. However, less is known about the psychological consequences of multiple partners, be they short-term serial or concurrent relationships. The psychological impact of such relationships may be because the relational aspect of sex is missing, i.e., the sex is “impersonal” (Långström & Hanson, 2006) and therefore there may be negative emotional consequences. Or it may be due to emotional consequences of the break ups of multiple short-term relationships. Further, men and women may differ in how they experience such relationships in so much as they vary in the reasons for engaging in sex: women tend more often to engage emotionally in sexual relationships than men (Meston & Buss, 2007).
In this study, we examined whether multiple sexual partners, one aspect of sexual risk taking, predicted a later diagnosis of common mental disorders: anxiety, depression, and substance dependence disorders. We examined this in three age periods over young adulthood. Our earlier work has shown cross-sectional associations at age 21 between multiple partners combined with inconsistent condom use, early sex, and STIs and a range of mental disorders, including anxiety, depression, and substance dependence (Ramrakha, Caspi, Dickson, Moffitt, & Paul, 2000). Further, we have previously examined whether prior mental health problems were associated with subsequent risky sex and showed that childhood antisocial behavior and low anxiety were associated with later sexual risk taking (Ramrakha et al., 2007).
Method
Participants
Participants were members of the Dunedin Multidisciplinary Health and Development Study, which has investigated the health and behavior of a cohort born during a 1-year period between April 1, 1972 and March 31, 1973, in Dunedin, a city of approximately 120,000 in New Zealand’s South Island. The cohort (n = 1037), a representative population sample, was established at age 3 years when the children were traced for follow-up and 91 % of the eligible births (still resident in the province) participated in the assessment. Cohort families were primarily white (91 %) and represented the full range of socioeconomic status in the general population of New Zealand’s South Island. Assessments have since been conducted at 2-year intervals until age 15 years, then again at age 18 (1990–1991), 21 (1993–1994), 26 (1998–1999), and 32 years (2003–2005). The total numbers seen at each assessment phase used in this study (as a percentage of known survivors) were as follows: age 18, 993/1027 (97 %), age 21, 992/1020 (97 %), age 26, 980/1019 (96 %), and age 32, 972/1015 (96 %). Ethical approval was obtained and confidentiality was assured for each component of the assessment.
Procedure
Participants (from all over New Zealand and overseas) were brought back to the unit for a full day of individual data collection at each assessment. Mental health data were collected in private standardized interviews by trained interviewers who were blind to the participants’ prior mental health status. Sexual behavior data were also collected in private interviews using a questionnaire based on the 1990 British National Survey of Sexual Attitudes and lifestyles (Johnson, Wadsworth, Wellings, & Field, 1994). Questions were presented by computer with an interviewer present who was placed so that they could not see the participants’ response but was available to provide instruction and to assist those with limited reading ability.
Measures
Number of Sexual Partners
Participants were asked questions about the number of opposite sex partners with whom they had penetrative sex in the last 3 years (at age 21), 5 years (at age 26), and last 6 years (at age 32). At each assessment age, they were also asked about the numbers for the last 12 months. These data were used to create the number of sexual partners’ variables for three age periods, that is, 2-year period from 18 to 20 years, 4-year period from 21 to 25 years, and 5-year period from 26 to 31 years. By subtracting the last 12 months sexual partners’ data, from the previous 3, 5, and 6 years, we ensured that these predictor variables did not overlap with the outcome, mental disorder, which was assessed for the previous 12 months at each age. Number of sexual partners per year was then categorized into three groups: 1.0 or less as the reference group, 1.1–2.5, and >2.5 partners for each period which allowed for comparison over three differing assessment periods.
Mental Health
Mental health data were collected using the Diagnostic Interview Schedule (Robins, Helzer, Croughan, & Ratcliff, 1981), a standardized interview which assessed disorders using criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM) developed by the American Psychiatric Association. The DSM is a standard classification of mental disorders and the then current editions were used at each age: DSM-III-R (APA, 1987), at ages 18 and 21, and DSM-IV (APA, 1994) at age 26 and 32. In addition to symptom criteria, diagnosis required an impairment rating >2 on a scale from 1 (some impairment) to 5 (severe impairment). Each disorder was diagnosed regardless of the presence of other disorders. Using a reporting period of the past year, mental disorders were assessed and they included those used in this study: anxiety, depression, and substance (cannabis and/or alcohol) dependence disorders.
Statistical Analysis
Logistic regression models were used to examine the association between reported number of sexual partners and later mental disorders (anxiety, depression, substance dependence). This was conducted separately for each age period because sexual behavior changed across time such that most people in the highest number of partners’ category in one period were not in it in the next period (Humblet, Paul, & Dickson, 2003). For each mental disorder outcome, we first assessed the interaction between gender and number of sex partners. If this was not statistically significant, we removed the interaction term and fitted two models: adjusting for gender only, and for gender and any mental disorder, at the prior assessment phase (e.g., for outcomes at age 21 years, prior disorder status at age 18 years, for outcomes at 26 and 32 years, prior disorder at 21 and 26 years, respectively). At age 18, n = 527 (50.8 %), at age 21 n = 569 (54.9 %), and at age 26 years, n = 519 (50.0 %) had a disorder the previous 12 months. Disorders included anxiety, depression, mania, eating, substance dependence, schizophrenia, conduct disorder (at 18 years) and antisocial personality disorders (at 21 and 26 years). We adjusted for any mental disorder at the prior assessment because comorbidity is more common in mental disorders than not (Angold, Costello, & Erkanli, 1999; Kim-Cohen et al., 2003). To illustrate, in this cohort, of those who had a substance dependence disorder at ages 21, 26, and 32 years, 45 %, 56 %, and 39 % respectively had a disorder other than substance dependence at the previous assessment. We also undertook prediction modelling using reported number of partners as a continuous variable for the outcome of substance abuse, while restricting this analysis to those with 50 reported partners or less, in order to estimate the interaction point that was most problematic for men and women.
Analyses were also conducted using new cases of disorder at each assessment age. For the purposes of this study, “a new case” was defined as those who had the disorder in question at 21, 26 or 32 years but did not have it at the previous assessment age (i.e., at 18, 21, or 26 years, respectively).
Assessment of potential confounding by socioeconomic status in childhood and at adulthood (age 32 years) was conducted. Adjustment had no appreciable effect on the results so socioeconomic status was not included in the final analyses.
Post-hoc analyses were conducted where the findings were significant to see if adjustment for early sex, or sexually transmitted infections, explained these findings. Because there were no appreciable differences to the odds ratio and the significance remained unchanged, only adjustment for prior disorder is shown in the tables.
Results
Table 1 shows the number and percentage of men and women with no mental disorder, with anxiety, depression, and substance dependence disorders, as well as new cases of disorder, at three assessment ages.
Table 1.
Numbers and percentages of men and women with a mental disorder, and a new disorder, at each assessment age
| Age | No disorder
|
Men
|
No disorder
|
Women
|
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | (%) | Anxiety
|
Depression
|
Substance dependence
|
N | % | Anxiety
|
Depression
|
Substance dependence
|
|||||||
| N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | |||||
| 21 | 299 | (61.3) | 65 | (13.3) | 55 | (11.3) | 148 | (30.6) | 270 | 57.6 | 130 | (27.7) | 106 | (22.6) | 68 | (14.6) |
| 26 | 262 | (52.7) | 101 | (20.3) | 67 | (13.5) | 132 | (26.6) | 257 | 53.7 | 136 | (28.4) | 94 | (19.6) | 56 | (11.7) |
| 32 | 309 | (57.8) | 92 | (18.8) | 59 | (12.0) | 82 | (16.8) | 293 | 58.4 | 122 | (25.8) | 98 | (20.7) | 34 | (7.2) |
| New case of disordera | ||||||||||||||||
| 21 | 33 | (7.2) | 34 | (7.4) | 78 | (17.1) | 51 | (11.4) | 67 | (15.1) | 42 | (9.5) | ||||
| 26 | 63 | (13.1) | 42 | (8.8) | 53 | (11.1) | 68 | (14.6) | 60 | (12.8) | 27 | (5.8) | ||||
| 32 | 45 | (9.3) | 40 | (8.3) | 30 | (6.3) | 61 | (13.0) | 67 | (14.2) | 18 | (3.8) | ||||
New cases are defined as those who did not have the disorder at the previous assessment phase
The relationships between annual number of sex partners and later anxiety and depression are shown in Table 2. Engaging in sex with multiple partners was not associated with an increased risk for anxiety or depression at 21, 26, or 32 years, once adjustment was made for any prior disorder. There was no significant interaction by gender so the combined results are presented.
Table 2.
The relationship between the reported number of sex partners and later anxiety and depression at three age periods
| Partners per year | N (%) | Anxiety
|
Depression
|
||||
|---|---|---|---|---|---|---|---|
| Odds ratio (95 % CI)
| |||||||
| N (%) | AORa | AORb | N (%) | AORa | AORb | ||
| 18–20 years | At age 21 years | ||||||
| 0–1 | 512 (55.7) | 107 (21.0) | 1.0 (reference) | 83 (16.3) | 1.0 (reference) | ||
| 1.1–2.5 | 293 (31.8) | 53 (18.1) | 0.9 (0.6, 1.3) | 0.8 (0.5, 1.2) | 47 (16.0) | 1.1 (0.7, 1.6) | 1.0 (0.7, 1.5) |
| > 2.5 | 115 (12.5) | 27 (23.5) | 1.4 (0.8, 2.3) | 1.0 (0.6, 1.6) | 25 (21.7) | 1.7 (1.0, 2.8) | 1.2 (0.7, 2.2) |
| 21–25 years | At age 26 years | ||||||
| 0–1 | 450 (47.7) | 111 (24.8) | 1.0 (reference) | 64 (14.3) | 1.0 (reference) | ||
| 1.1–2.5 | 412 (43.6) | 94 (22.9) | 1.0 (0.7, 1.3) | 1.0 (0.7, 1.4) | 75 (18.2) | 1.5 (1.0, 2.1)* | 1.3 (0.9, 2.0) |
| >2.5 | 82 (8.7) | 18 (22.0) | 1.0 (0.6, 1.8) | 0.9 (0.5, 1.7) | 15 (18.3) | 1.6 (0.9, 3.1) | 1.4 (0.7, 2.8) |
| 26–31 years | At age 32 years | ||||||
| 0–1 | 513 (56.1) | 109 (21.1) | 1.0 (reference) | 73 (14.1) | 1.0 (reference) | ||
| 1.1–2.5 | 350 (38.0) | 73 (20.9) | 1.1 (0.8, 1.5) | 0.9 (0.6, 1.3) | 59 (16.9) | 1.4 (1.0, 2.1)* | 1.2 (0.8, 1.8) |
| >2.5 | 54 (5.9) | 17 (31.5) | 2.3 (1.2, 4.3)* | 1.5 (0.8, 3.0) | 9 (16.7) | 1.8 (0.8, 3.9) | 1.3 (0.6, 3.0) |
p<.05
AOR = Adjusted, for sex, odds ratio
AOR = Adjusted, for sex and prior disorder, odds ratio
The association between number of partners and later substance dependence disorders for women and men are shown in Table 3. Because analyses showed a significant interaction by gender, the results are shown separately for men and women. For women, there were statistically significant associations between numbers of sexual partners and substance dependence disorder at all age periods and the odds ratio increased with increasing number of partners. For men, this was true at ages 21 and 32 but not at age 26 years. Women reporting more than 2.5 partners per year had much greater odds of being diagnosed with a substance dependence disorder than those with only one or no partners, at each age: adjusted odds ratios and 95 % confidence intervals were 9.6 (4.4–20.9), 7.3 (2.5–21.3), and 17.5 (3.5–88.1) at 21, 26, and 32 years, respectively. The effect was strongest at age 32, but this was based on small numbers. Further, the predictive models showed that at ages 21, 26, and 32 years, although having multiple sex partners was followed by substance dependence disorders for both genders, men were more likely than women to have a disorder when they had no or few sex partners whereas women who had more than approximately 10 sex partners in the same time period were much more likely to have a disorder than men (see Fig. 1).
Table 3.
The association between reported number of sex partners and later substance dependence disorder for women and men at three age periods
| Partner per year | N (%) | Substance dependence disorder
|
||
|---|---|---|---|---|
| N (%) | Unadjusted | AORa | ||
| Women | ||||
| 18–20 years | At 21 years | |||
| 0–1 | 281 (61.8) | 21 (7.5 %) | 1.0 (reference) | |
| 1.1–2.5 | 131 (28.8) | 22 (16.8) | 2.5 (1.3, 4.7)* | 2.4 (1.2, 4.6)* |
| > 2.5 | 43 (9.5) | 20 (46.5) | 10.8 (5.1, 22.7)* | 9.6 (4.4, 20.9)* |
| 21–25 years | At 26 years | |||
| 0–1 | 264 (56.2) | 20 (7.6) | 1.0 (reference) | |
| 1.1–2.5 | 185 (39.4) | 28 (15.1) | 2.2 (1.2, 4.0)* | 2.1 (1.1, 4.0)* |
| > 2.5 | 21 (4.5) | 7 (33.3) | 6.1 (2.2, 16.7)* | 7.3 (2.5, 21.3)* |
| 26–31 years | At 32 years | |||
| 0–1 | 306 (65.9) | 12 (3.9) | 1.0 (reference) | |
| 1.1–2.5 | 150 (32.3) | 17 (11.3) | 3.1 (1.4, 6.7)* | 2.3 (1.0, 5.1)* |
| > 2.5 | 8 (1.7) | 4 (50.0) | 24.3 (5.4, 109.2)* | 17.5 (3.5, 88.1)* |
| Men | ||||
| 18–20 years | At 21 years | |||
| 0–1 | 231 (49.7) | 42 (18.4) | 1.0 (reference) | |
| 1.1–2.5 | 162 (34.8) | 60 (37.0) | 2.7 (1.6, 4.1)* | 2.6 (1.6, 4.3)* |
| > 2.5 | 72 (15.5) | 38 (52.8) | 5.0 (2.8, 8.8)* | 4.3 (2.3, 8.1)* |
| 21–25 years | At 26 years | |||
| 0–1 | 186 (39.2) | 35 (18.8) | 1.0 (reference) | |
| 1.1–2.5 | 227 (47.9) | 71 (31.4) | 2.0 (1.2, 3.1)* | 2.0 (1.2, 3.3)* |
| > 2.5 | 61 (12.9) | 16 (26.2) | 1.5 (0.8, 3.0)* | 1.3 (0.6, 2.7) |
| 26–31 years | At 32 years | |||
| 0–1 | 210 (46.1) | 22 (10.5) | 1.0 (reference) | |
| 1.1–2.5 | 200 (43.9) | 35 (17.6) | 1.8. (1.0, 3.2)* | 1.5 (0.8, 2.7) |
| > 2.5 | 46 (10.1) | 14 (30.4) | 3.7 (1.7, 8.0)* | 2.6 (1.2, 5.7)* |
p<.05
AOR = Adjusted, for prior disorder, odds ratio
Fig. 1.
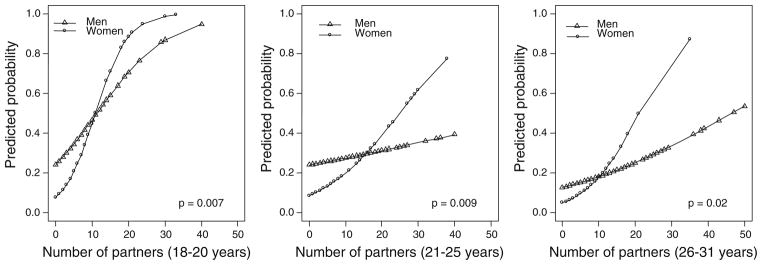
Predicted probability of substance dependence disorder from a logistic model including reported number of partners, sex, and their interaction. Reported number of partners was used as a continuous variable and restricted to those with partners ≤50. The p value shown is for the interaction term
The effects of alcohol and cannabis dependence disorders were examined separately and similar patterns were shown for both men and women combined (Table 4). Separate results by gender were not possible due to very small numbers in the cells.
Table 4.
The association between reported number of sexual partners and alcohol and cannabis dependence disorders at three age periods
| Partners/year | N (%) | Alcohol dependence
|
Cannabis dependence
|
|||
|---|---|---|---|---|---|---|
| Odds ratio (95 % CI)
| ||||||
| AORa | AORb | N (%) | AORa | AORb | ||
| 18–20 years | At 21 years | |||||
| 0–1 | 26 (5.1) | 1.0 (reference) | 26 (5.1) | 1.0 (reference) | ||
| 1.1–2.5 | 39 (13.3) | 2.7 (1.6, 4.5)* | 2.4 (1.4, 4.2)* | 29 (9.9) | 1.8 (1.1, 3.2)* | 1.7 (0.9, 3.1)* |
| > 2.5 | 24 (20.9) | 4.4 (2.4, 8.0)* | 3.4 (1.8, 6.4)* | 34 (29.6) | 6.9 (3.9, 12.2)* | 6.0 (3.2, 11.1)* |
| 21–25 years | At 26 years | |||||
| 0–1 | 31 (6.9) | 1.0 (reference) | 31 (6.9) | 1.0 (reference) | ||
| 1.1–2.5 | 72 (17.5) | 2.6 (1.6, 4.0)* | 2.6 (1.6, 4.1)* | 49 (11.9) | 1.6 (1.0, 2.6)* | 1.6 (1.0, 2.7)* |
| > 2.5 | 21 (25.6) | 3.5 (1.9, 6.7)* | 3.3 (1.7, 6.5)* | 6 (7.3) | 0.8 (0.3, 2.0) | 0.6 (0.2, 1.7) |
| 26–32 years | At 32 years | |||||
| 0–1 | 27 (5.3) | 1.0 (reference) | 11 (2.1) | 1.0 (reference) | ||
| 1.1–2.5 | 31 (8.9) | 1.6 (0.9, 2.8) | 1.3 (0.7, 2.2) | 27 (7.7) | 3.3 (1.6, 6.8)* | 2.8 (1.3, 5.8)* |
| > 2.5 | 12 (22.2) | 4.2 (1.9, 9.1)* | 2.8 (1.2, 6.1)* | 7 (13.0) | 4.6 (1.7, 12.8)* | 3.2 (1.1, 9.1)* |
p<.05
AOR = Adjusted, for sex, odds ratio
AOR = Adjusted, for sex and prior disorder, odds ratio
These analyses were repeated using new cases of disorder, that is, those who had the disorder at one assessment age but did not have it at the previous assessment age and the results are similar. Table 5 shows no significant relationships between numbers of sex partners and later anxiety and depression, except for depression and the 1.1–2.5 partners per year category, at age 26. However, this was not supported by significance for those who had >2.5 partners per year, i.e., there was no expected dose response relationship. Further, when this link was examined using the continuous partner variable, there was no significant association.
Table 5.
The association between the reported number of sex partners and new cases of anxiety and depression at three age periods
| Partners/year | Adjusted odds ratioa (95 % CI)
|
|||
|---|---|---|---|---|
| N (%) | New anxietyb | N (%) | New depressionb | |
| 18–20 years | At 21 years | |||
| 0–1 | 47 (9.8) | 1.0 (reference) | 56 (11.6) | 1.0 (reference) |
| 1.1–2.5 | 22 (7.9) | 0.8 (0.5, 1.4) | 30 (10.8) | 1.0 (0.6, 1.6) |
| > 2.5 | 10 (9.3) | 1.0 (0.5, 2.1) | 11 (10.3) | 1.0 (0.5, 2.0) |
| 21–25 years | At 26 years | |||
| 0–1 | 55 (12.6) | 1.0 (reference) | 37 (8.5) | 1.0 (reference) |
| 1.1–2.5 | 58 (14.4) | 1.2 (0.8, 1.8) | 52 (12.9) | 1.7 (1.1, 2.7)* |
| > 2.5 | 11 (13.9) | 1.2 (0.6, 2.4) | 9 (11.4) | 1.7 (0.8, 3.8) |
| 26–31 years | At 32 years | |||
| 0–1 | 54 (10.5) | 1.0 (reference) | 53 (10.3) | 1.0 (reference) |
| 1.1–2.5 | 35 (10.1) | 1.0 (0.7, 1.7) | 40 (11.5) | 1.3 (0.8, 2.0) |
| > 2.5 | 8 (14.8) | 2.0 (0.8, 4.5) | 4 (7.4) | 1.0 (0.3, 2.8) |
p<.05
Adjusted for sex
New cases are defined as those who did not have the disorder at the previous assessment phase
In Table 6, the relationship between number of sex partners and new cases of later substance dependence disorder are shown. Although the interaction analysis by gender was not significant at age 21 or 26, it was significant at age 32 (p = .01). Because of this and due to the significant differences between men and women in the earlier analyses (as shown in Table 3), the results are again presented separately by gender. These results showed similar, though less marked trends: women were more likely than men to have a new substance dependence disorder with increasing numbers of partners.
Table 6.
The association between the reported number of sex partners and later new cases of substance dependence disorder at three age periods
| Partners/year | N (%) | Men | Women | |
|---|---|---|---|---|
| New case of substance disordera
| ||||
| Odds ratio (95 % CI) | N (%) | Odds ratio (95 % CI) | ||
| 18–20 years | At 21 years | |||
| 0–1 | 24 (11.1) | 1.0 (reference) | 13 (4.9) | 1.0 (reference) |
| 1.1–2.5 | 35 (22.9) | 2.4 (1.4, 4.2)* | 17 (13.5) | 3.0 (1.4, 6.4)* |
| > 2.5 | 16 (24.6) | 2.6 (1.3, 5.3)* | 9 (20.9) | 5.1 (2.0, 12.9)* |
| 21–25 years | At 26 years | |||
| 0–1 | 15 (8.4) | 1.0 (reference) | 8 (3.1) | 1.0 (reference) |
| 1.1–2.5 | 26 (11.8) | 1.5 (0.7, 2.9) | 16 (8.8) | 3.0 (1.3, 7.2) |
| > 2.5 | 7 (11.9) | 1.5 (0.6, 3.8) | 2 (11.1) | 3.9 (0.8, 19.9) |
| 26–32 years | At 32 years | |||
| 0–1 | 11 (5.3) | 1.0 (reference) | 8 (2.6) | 1.0 (reference) |
| 1.1–2.5 | 15 (7.6) | 1.5 (0.7, 3.3) | 7 (4.7) | 1.8 (0.6, 5.1) |
| > 2.5 | 3 (6.5) | 1.2 (0.3, 4.6) | 3 (35.5) | 22.1 (4.5, 109.1)* |
p<.05
New cases are defined as those who did not have a substance dependence disorder at the previous assessment phase
Discussion
The results showed that, taking into account prior disorder status, increasing number of sex partners was associated with a striking increase in later substance dependence disorders, especially for women. On the other hand, no consistent associations were found with later anxiety or depression at any age. The results were confirmed when using new cases of disorder, that is, a disorder present at one assessment age but not at the previous assessment age.
The strong associations between multiple sex partners and later substance dependence disorders during young adulthood are particularly interesting. Other studies have shown a similar relationship in the reverse direction, that with frequent and heavy drinking, there is a greater likelihood of risk taking, including having multiple sex partners (e.g., Cavazos-Rehg et al., 2007; Dogan, Stockdale, Widaman, & Conger, 2010; Ferguson & Lynsky, 1996; Lavan & Johnson, 2002; Valois, Oeltmann, Waller, & Hussey, 1999; Zenilman, Hook, Shepherd, Rompalo, & Celentano, 1994). Our study examined substance use at a disorder level and established that the association persisted beyond prior substance use and prior mental health problems more generally. Further, there appeared to be a “dose–response” relation with number of partners. That is, the risk of substance dependence disorder increased with increasing number of sex partners. It was also present at each age for women. These associations were not confounded by socioeconomic status, age at first coitus, or a history of STIs.
Other studies have examined prospectively early age at first intercourse and subsequent substance dependence disorders. McGue and Iacono (2005) reported that sexual intercourse in early adolescence was associated with later substance use disorder. Cornelius et al. (2007) also found that early age at first sex for men predicted later substance disorder, for both alcohol and cannabis. To our knowledge, this is the first study to examine the effect of multiple sex partners on mental health in young adulthood in a general population sample.
The explanation for the relationship is likely to be complex. Four possibilities are proposed. First, sexual risk taking and substance use may be part of the cluster of risk taking behaviors common in adolescence and young adulthood (Arnett, 1992; Boyer et al., 2000; Caspi et al., 1997; Desiderato & Crawford, 1995; Donovan & Jessor, 1985; Taylor, Fulop, & Green, 1999). For instance, people who are impulsive may be more likely to engage in both activities and, consequently, more likely to become substance dependent. Second, occasions of substance use are opportunities for sexual behavior because of its disinhibitory effects and lack of accurate perception of risk (Crowe & George, 1989; Fromme, D’Amico, & Katz, 1999). Weinhardt and Carey (2000) have suggested, in a review of event-level research on this topic, that the association, especially with condom use, is also complex. Thirdly, shared context may be an important factor, insomuch as young people are likely to meet new sexual partners in situations where alcohol is served. These settings might encourage sexual behavior and facilitate multiple partnering.
The fourth intriguing possibility is that it is something about having multiple sex partners itself which puts people at risk of substance disorder. For instance, it may be due to the impersonal nature of such relationships. Or, it might be that multiple failed relationships create anxiety about initiating new relationships. Self “medication” with substances may be one way of dealing with this interpersonal anxiety (Khantzian, 1997; Stoner, George, Peters, & Norris, 2006). Specifically, feelings of loneliness and hopelessness are related to substance use (Page, Allen, Moore, & Hewitt, 1993) and drinking alcohol to cope with negative emotions has been shown to result in alcohol problems (Cooper, Shapiro, & Powers, 1998; Taylor et al., 1999).
Perhaps surprisingly in view of the earlier cross-sectional relationship, there was no clear association with multiple sex partners and subsequent anxiety or depressive disorders. Consistent with this null finding, a review of studies found that negative states (including depression and anxiety) were unrelated to sexual risk taking (Crepaz & Marks, 2000). However, Shrier et al. (2002) showed relationships between STI diagnoses and depression a year later for both men and women. In the same cohort, Hallfors et al. (2005) found that multiple partners (>13) in adolescence substantially increased the risk for depression 1 year later, especially for women. Spriggs and Halpern (2008) also found that early sex was related to later depression though only among very young adolescents. In our study, we examined sexual behavior over three discrete periods and mental health in the 12 months immediately after those periods. It is possible that any problems from depression or anxiety that may have arose from multiple sexual partnerships may have resolved themselves in that time period, that is, there were no long-term consequences for depression or anxiety. Alternatively, the true causal direction may run from anxiety and depressive disorders to sexual behavior and this needs to be explored further.
Sex Differences
Although having multiple sex partners increased the odds of substance dependence disorders for both sexes, the probability of a disorder was higher for men with up to 10 sex partners in the same period compared to women; however, with more than 10 partners, the probability of a disorder was substantially higher among women versus men. This trend was repeated over approximately a decade, from early 20s to early 30s. Although substance dependence and multiple partners were more common among men than women at each age, the relationship between multiple partners and substance dependence was stronger for women at each age.
Studies have shown that there is increasing similarity between the sexual behavior of young men and women (Grunseit, Richters, Crawford, Song, & Kippax 2005) as well as patterns of substance use (Sarigiani, Ryan, & Petersen, 1999). These results suggest that although women may behave in a manner similar to men, they may nevertheless experience more dissonance between their behavior and both their own expectations as well as societal gender role expectations. Gender differences in relation to sexual attitudes include differences towards casual sex: men are generally more accepting of casual sex and hold more sexually permissive attitudes than women and women are more accepting of double standards in society (e.g., Crawford & Popp, 2003; Oliver & Hyde, 1993; Sprecher & Hatfield, 1996). Further, men and women may have different motives for having sex. Women often say it is for love, commitment, and emotional reasons and while men also share these motivations, they may be more likely to also participate in sex just for physical reasons (Carroll, Volk, & Hyde 1985; Meston & Buss, 2007). Some women may use alcohol for its disinhibiting effects, thus making it easier to engage in sex (Taylor et al., 1999). Tolman (2002) suggested that young women may find it difficult to acknowledge and assert their own sexual feelings and desires and therefore act only on their partner’s desires. Further, they may suppress or ignore their own desires because they fear pregnancy and disease, which results in confusion and anxiety. In a recent study, Blythe, Fortenberry, Temkit, Tu, and Orr (2006) found that young women engaged in unwanted sex because they feared anger from their partner if they denied sex. Therefore, it is probable that, for women, experiences with frequent casual sex will sometimes result in complex and conflicting feelings of shame, fear, and dissatisfaction, and substance use may alleviate the negative feelings while facilitating these encounters.
This study was not without limitations. The data were from one country. However, the prevalence rates for mental disorder and sexual behavior were broadly similar to other Western countries (Humblet et al., 2003; Kim-Cohen et al., 2003; Moffitt et al., 2007). Nevertheless, the study needs to be replicated in other countries and cultures. Further, the sexual risk measures were self-reported and there was insufficient contextual information available to fully inform interpretation of the findings. Although adjustment was made for prior substance disorder, no allowance was made for prior heavy drinking short of disorder. The analysis was restricted to heterosexual partners, because people with same-sex partners operate in different contexts. However, this could lead to potential misclassification, as people with multiple same-sex partners only would be classified as 0–1 partners. In fact, only one man was in this category. We excluded dependence on other drugs apart from alcohol and cannabis as we did not have other drug dependence information at age 21. For the analyses at age 26 and 32, we examined the effect of all substance dependence and the results were unchanged. The major strengths of this study were the prospective longitudinal design, which allows temporality of the measures to be established, the same measures were examined over three age periods, and the ability to take into account prior mental disorder status. Moreover, the extremely high retention of the cohort greatly reduced the possibility of bias.
In conclusion, this study examined whether multiple sex partnerships can lead to later mental health problems and found no association with anxiety and depression but a strong association with substance dependence across three age periods. It highlights the possibility that interpersonal anxieties stemming from multiple (possibly failed) sexual partnerships may lead to substance abuse problems, especially for women.
Changes in contemporary society are demonstrated in the current sexual mores and alcohol consumption norms. Our findings showed that there are serious health concerns regarding multiple short term sexual partnerships. Further research is required to examine these relationships in other cultures and to elucidate the mechanisms involved.
Acknowledgments
The Dunedin Multidisciplinary Health and Development Research Unit is supported by the Health Research Council of New Zealand. This research also received support from the United Kingdom Medical Research Council (Grant G0100527) and from the National Institute of Mental Health (Grants MH45070 and MH49414). Terrie E. Moffitt and Avshalom Caspi are Royal Society Wolfson Research Merit Award holders. The authors are grateful to Richie Poulton, Director of the Research Unit, for valuable comments on earlier drafts of this paper. We thank Antony Ambler for assistance with the analyses. The authors are indebted to Phil Silva, the founder of the Dunedin Study, and to the Study members and their families for their long-term involvement.
Contributor Information
Sandhya Ramrakha, Email: sandhya.ramrakha@otago.ac.nz, Dunedin Multidisciplinary Health and Development Research Unit, Department of Preventive and Social Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand.
Charlotte Paul, Department of Preventive and Social Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand.
Melanie L. Bell, Department of Preventive and Social Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand
Nigel Dickson, Department of Preventive and Social Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand.
Terrie E. Moffitt, Departments of Psychology and Neuroscience and Psychiatry and Behavioral Sciences and Institute for Genome Sciences and Policy, Duke University, Durham, NC, USA. Social, Genetic, and Developmental Psychiatry Research Centre, Institute of Psychiatry, Kings College, London, UK
Avshalom Caspi, Departments of Psychology and Neuroscience and Psychiatry and Behavioral Sciences and Institute for Genome Sciences and Policy, Duke University, Durham, NC, USA. Social, Genetic, and Developmental Psychiatry Research Centre, Institute of Psychiatry, Kings College, London, UK.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3. Washington, DC: Author; 1987. rev. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: Author; 1994. [Google Scholar]
- Angold A, Costello EJ, Erkanli A. Comorbidity. Journal of Child Psychology and Psychiatry. 1999;40:57–87. [PubMed] [Google Scholar]
- Aral SO. Social and behavioral determinants of sexually transmitted disease: Scientific and technologic advances, demography, and the global political economy. Sexually Transmitted Diseases. 2006;33:698–702. doi: 10.1097/01.olq.0000250476.76031.e8. [DOI] [PubMed] [Google Scholar]
- Arnett JJ. Reckless behavior in adolescence: A developmental perspective. Developmental Review. 1992;12:339–373. [Google Scholar]
- Bachanas PJ, Morris MK, Lewis-Gess JK, Sarett-Cuasay EJ, Flores AL, Sirl KS, Sawyer MK. Psychological adjustment, substance use, HIV knowledge, and risky sexual behavior in at-risk minority females: Developmental differences during adolescence. Journal of Pediatric Psychology. 2002;27:373–384. doi: 10.1093/jpepsy/27.4.373. [DOI] [PubMed] [Google Scholar]
- Baskin-Sommers A, Sommers I. The co-occurrence of substance use and high risk behaviors. Journal of Adolescent Health. 2006;38:609–611. doi: 10.1016/j.jadohealth.2005.07.010. [DOI] [PubMed] [Google Scholar]
- Blythe MJ, Fortenberry JD, Temkit M, Tu W, Orr DP. Incidence and correlates of unwanted sex in relationships of middle and late adolescence women. Archives of Pediatric Medicine. 2006;160:591–595. doi: 10.1001/archpedi.160.6.591. [DOI] [PubMed] [Google Scholar]
- Boden JM, Fergusson DM, Horwood LJ. Alcohol and STI risk: Evidence from a New Zealand longitudinal birth cohort. Drug and Alcohol Dependence. 2010;113:200–206. doi: 10.1016/j.drugalcdep.2010.08.005. [DOI] [PubMed] [Google Scholar]
- Bohon C, Garber J, Horowitz JL. Predicting school dropout and adolescent sexual behavior in offspring of depressed and non-depressed mothers. Journal of the American Academy of Child and Adolescent Psychiatry. 2007;46:15–24. doi: 10.1097/01.chi.0000246052.30426.6e. [DOI] [PubMed] [Google Scholar]
- Boyer CB, Shafer M, Wibbelsman CJ, Seeberg D, Teitle E, Lowell N. Associations of sociodemographic, psychosocial, and behavioral factors with sexual risk and sexually transmitted diseases in teen clinic patients. Journal of Adolescent Health. 2000;27:102–111. doi: 10.1016/s1054-139x(99)00113-5. [DOI] [PubMed] [Google Scholar]
- Brook JS, Balka EB, Whiteman M. The risks for late adolescence of early adolescent marijuana use. American Journal of Public Health. 1999;89:1549–1554. doi: 10.2105/ajph.89.10.1549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown LK, Tolou-Shams M, Lescano C, Houck C, Zeidman J, Pugatch D, et al. Depressive symptoms as a predictor of sexual risk among African American adolescents and young adults. Journal of Adolescent Health. 2006;39:444e1–444e8. doi: 10.1016/j.jadohealth.2006.01.015. [DOI] [PubMed] [Google Scholar]
- Carroll JL, Volk KD, Hyde JS. Differences between males and females in motives for engaging in sexual intercourse. Archives of Sexual Behavior. 1985;14:131–139. doi: 10.1007/BF01541658. [DOI] [PubMed] [Google Scholar]
- Caspi A, Begg D, Dickson N, Harrington H, Langley J, Moffit TE, Silva PA. Personality differences predict health-risk behaviors in young adulthood: Evidence from a longitudinal study. Journal of Personality and Social Psychology. 1997;73:1052–1063. doi: 10.1037//0022-3514.73.5.1052. [DOI] [PubMed] [Google Scholar]
- Cavazos-Rehg PA, Spitznagel EL, Bucholz KK, Norberg K, Reich W, Numberger J, et al. The relationship between alcohol problems and dependence, conduct problems and diagnosis, and number of sex partners in a sample of young adults. Alcoholism, Clinical and Experimental Research. 2007;31:2046–2052. doi: 10.1111/j.1530-0277.2007.00537.x. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Trends in reportable sexually transmitted disease in the United States, 2004. Atlanta, GA: U.S. Department of Health and Human Services; 2005. [Google Scholar]
- Cooper ML, Shapiro CM, Powers AM. Motivations for sex and risky sexual behavior among adolescents and young adults: A functional perspective. Journal of Personality and Social Psychology. 1998;75:1528–1558. doi: 10.1037//0022-3514.75.6.1528. [DOI] [PubMed] [Google Scholar]
- Cornelius JR, Clark DB, Reynolds M, Kirisci L, Tarter R. Early age of first sexual intercourse predict development of SUD: A prospective longitudinal study. Addictive Behaviors. 2007;32:850–854. doi: 10.1016/j.addbeh.2006.06.027. [DOI] [PubMed] [Google Scholar]
- Crawford M, Popp D. Sexual double standards: A review and methodological critique of two decades of research. Journal of Sex Research. 2003;40:13–26. doi: 10.1080/00224490309552163. [DOI] [PubMed] [Google Scholar]
- Crepaz N, Marks G. Are affective negative states associated with HIV sexual risk behaviors? A meta-analytic review. Health Psychology. 2000;20:291–299. doi: 10.1037//0278-6133.20.4.291. [DOI] [PubMed] [Google Scholar]
- Crowe LC, George WH. Alcohol and human sexuality: Review and integration. Psychological Bulletin. 1989;105:374–386. doi: 10.1037/0033-2909.105.3.374. [DOI] [PubMed] [Google Scholar]
- Desiderato LL, Crawford HJ. Risky sexual behavior in college students: Relationships between number of sexual partners, disclosure of previous risky behavior, and alcohol use. Journal of Youth and Adolescence. 1995;24:55–68. [Google Scholar]
- Dishion TJ. Cross-setting consistency in early adolescent psychopathology: Deviant friendships and problem behavior sequelae. Journal of Personality. 2000;68:1109–1126. doi: 10.1111/1467-6494.00128. [DOI] [PubMed] [Google Scholar]
- Dogan SJ, Stockdale GD, Widman KF, Conger RD. Developmental relations and patterns of change between alcohol use and number of sexual partners from adolescence through adulthood. Developmental Psychology. 2010;46:1747–1759. doi: 10.1037/a0019655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donovan JE, Jessor R. Structure of problem behavior in adolescence and young adulthood. Journal of Consulting and Clinical Psychology. 1985;53:890–904. doi: 10.1037//0022-006x.53.6.890. [DOI] [PubMed] [Google Scholar]
- Duncan SE, Strycker LA, Duncan TE. Exploring associations in developmental trends of adolescent substance use and risky sexual behavior in a high-risk population. Journal of Behavioral Medicine. 1999;22:21–33. doi: 10.1023/a:1018795417956. [DOI] [PubMed] [Google Scholar]
- Erbelding E, Hummel B, Hogan T, Zenlman J. High rates of depressive symptoms in STD clinic patients. Sexually Transmitted Diseases. 2001;28:281–284. doi: 10.1097/00007435-200105000-00008. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Lynskey MT. Alcohol misuse and adolescent sexual behaviors and risk taking. Pediatrics. 1996;98:91–96. [PubMed] [Google Scholar]
- Fromme K, D’Amico EJ, Katz EC. Intoxicated sexual risk taking: An expectancy or cognitive impairment explanation? Journal of Studies on Alcohol. 1999;60:54–63. doi: 10.15288/jsa.1999.60.54. [DOI] [PubMed] [Google Scholar]
- Grunseit AC, Richters J, Crawford J, Song A, Kippax S. Stability and change in sexual practices among first-year Australian university students (1990–1999) Archives of Sexual Behavior. 2005;34:557–568. doi: 10.1007/s10508-005-6281-x. [DOI] [PubMed] [Google Scholar]
- Hallfors DD, Waller MW, Bauer D, Ford CA, Halpern CT. Which comes first in adolescence—sex and drugs or depression? American Journal of Preventive Medicine. 2005;29:163–170. doi: 10.1016/j.amepre.2005.06.002. [DOI] [PubMed] [Google Scholar]
- Humblet O, Paul C, Dickson N. Core group evolution over time: High-risk behavior in a birth cohort between sexual debut and age 26. Sexually Transmitted Diseases. 2003;30:818–824. doi: 10.1097/01.OLQ.0000097102.42149.11. [DOI] [PubMed] [Google Scholar]
- Hutton HE, Lyketsos CG, Zenilman JM, Thompson RE, Erbelding EJ. Depression and HIV risk behaviors among patients in a sexually transmitted disease clinic. American Journal of Psychiatry. 2004;161:912–914. doi: 10.1176/appi.ajp.161.5.912. [DOI] [PubMed] [Google Scholar]
- Johnson AM, Wadsworth J, Wellings K, Field J. Sexual attitudes and lifestyle. Oxford: Blackwell; 1994. [Google Scholar]
- Khantzian EJ. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harvard Review of Psychiatry. 1997;4:231–244. doi: 10.3109/10673229709030550. [DOI] [PubMed] [Google Scholar]
- Kim-Cohen J, Caspi A, Moffitt TE, Harrington HL, Milne BJ, Poulton R. Prior juvenile diagnoses in adults with mental disorder. Archives of General Psychiatry. 2003;60:709–717. doi: 10.1001/archpsyc.60.7.709. [DOI] [PubMed] [Google Scholar]
- Långström N, Hanson High rates of sexual behavior in the general population: Correlates and predictors. Archives of Sexual Behavior. 2006;35:37–52. doi: 10.1007/s10508-006-8993-y. [DOI] [PubMed] [Google Scholar]
- Lavan H, Johnson JG. The association between axis I and II psychiatric symptoms and high-risk sexual behavior during adolescence. Journal of Personality Disorders. 2002;16:73–94. doi: 10.1521/pedi.16.1.73.22559. [DOI] [PubMed] [Google Scholar]
- Mazzaferro KE, Murray PJ, Ness RB, Bass DC, Tyus N, Cook RL. Depression, stress, and social support as predictors of high-risk sexual behaviors and STIs in young women. Journal of Adolescent Health. 2006;39:601–603. doi: 10.1016/j.jadohealth.2006.02.004. [DOI] [PubMed] [Google Scholar]
- McGue M, Iacono WG. The association of early adolescent problem behavior with adult psychopathology. American Journal of Psychiatry. 2005;162:1118–1124. doi: 10.1176/appi.ajp.162.6.1118. [DOI] [PubMed] [Google Scholar]
- Meston CM, Buss DM. Why humans have sex. Archives of Sexual Behavior. 2007;36:477–507. doi: 10.1007/s10508-007-9175-2. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Harrington H, Caspi A, Kim-Cohen J, Goldberg D, Gregory A, Poulton R. Depression and generalized anxiety disorder. Archives of General Psychiatry. 2007;64:651–660. doi: 10.1001/archpsyc.64.6.651. [DOI] [PubMed] [Google Scholar]
- Mota NP, Cox BJ, Katz LJ, Sareen J. Relationship between mental disorders/suicidality and three sexual behaviours: Results from the National Comorbidity Survey Replication. Archives of Sexual Behavior. 2010;39:724–734. doi: 10.1007/s10508-008-9463-5. [DOI] [PubMed] [Google Scholar]
- Oliver MB, Hyde JS. Gender differences in sexuality: A meta-analysis. Psychological Bulletin. 1993;114:29–51. doi: 10.1037/0033-2909.114.1.29. [DOI] [PubMed] [Google Scholar]
- Page RM, Allen O, Moore L, Hewitt C. Co-occurrence of substance use and loneliness as a risk factor for adolescent hopelessness. Journal of School Health. 1993;63:104–108. doi: 10.1111/j.1746-1561.1993.tb06090.x. [DOI] [PubMed] [Google Scholar]
- Ramrakha S, Bell ML, Paul C, Dickson N, Moffitt TE, Caspi A. Childhood behavior problem linked to sexual risk taking in young adulthood: A birth cohort study. Journal of the American Academy of Child and Adolescent Psychiatry. 2007;46:1272–1279. doi: 10.1097/chi.0b013e3180f6340e. [DOI] [PubMed] [Google Scholar]
- Ramrakha S, Caspi A, Dickson N, Moffitt TE, Paul C. Psychiatric disorders and risky sexual behavior in young adulthood: Cross sectional study in birth cohort. British Medical Journal. 2000;321:263–266. doi: 10.1136/bmj.321.7256.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health Diagnostic Interview Schedule: Its history, characteristics, and validity. Archives of General Psychiatry. 1981;38:381–389. doi: 10.1001/archpsyc.1981.01780290015001. [DOI] [PubMed] [Google Scholar]
- Sarigiani PA, Ryan L, Petersen AC. Prevention of high risk behaviors in adolescent women. Journal of Adolescent Health. 1999;25:109–119. doi: 10.1016/s1054-139x(99)00015-4. [DOI] [PubMed] [Google Scholar]
- Shrier LA, Harris SK, Beardslee WR. Temporal associations between depressive symptoms and self-reported sexually transmitted disease among adolescents. Archives of Pediatrics and Adolescent Medicine. 2002;156:599–606. doi: 10.1001/archpedi.156.6.599. [DOI] [PubMed] [Google Scholar]
- Sprecher S, Hatfield E. Premarital sexual standards among U.S. college students: Comparisons with Russian and Japanese students. Archives of Sexual Behavior. 1996;25:261–287. doi: 10.1007/BF02438165. [DOI] [PubMed] [Google Scholar]
- Spriggs AL, Halpern CT. Sexual debut timing and depressive symptoms in emerging adulthood. Journal of Youth and Adolescence. 2008;37:1085–1096. doi: 10.1007/s10964-008-9303-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoner SA, George WH, Peters LM, Norris J. Liquid courage: Alcohol fosters risky sexual decision-making in individuals with sexual fears. AIDS and Behavior. 2006;11:227–237. doi: 10.1007/s10461-006-9137-z. [DOI] [PubMed] [Google Scholar]
- Taylor J, Fulop N, Green J. Drink, illicit drugs and unsafe sex in women. Addiction. 1999;94:1209–1218. doi: 10.1046/j.1360-0443.1999.948120911.x. [DOI] [PubMed] [Google Scholar]
- Tolman D. Dilemmas of desire: Teenage girls talk about sexuality. Cambridge, MA: Harvard University Press; 2002. [Google Scholar]
- Valois RF, Oeltmann JE, Waller J, Hussey JR. Relationship between number of sexual intercourse partners and selected health risk behaviors among public high school adolescents. Journal of Adolescent Health. 1999;25:328–335. doi: 10.1016/s1054-139x(99)00051-8. [DOI] [PubMed] [Google Scholar]
- Weinhardt LS, Carey MP. Does alcohol lead to sexual risk behavior? Findings from event-level research. Annual Review of Sex Research. 2000;11:125–157. [PMC free article] [PubMed] [Google Scholar]
- Zenilman JM, Hook EW, Shepherd M, Rompalo AM, Celentano DD. Alcohol and other substance use in STD clinic patients: Relationships with STDs and prevalent HIV infection. Sexually Transmitted Diseases. 1994;21:220–225. doi: 10.1097/00007435-199407000-00008. [DOI] [PubMed] [Google Scholar]