

Abstract
The current study investigated whether younger (college-age) and older adults (60+ years) differ in their ability to perceive safe and unsafe motor actions. Participants decided whether to walk through openings varying in width in two penalty conditions: In the doorway condition, if participants attempted to squeeze through impossibly narrow openings, the penalty for error was entrapment. In the ledge condition, if participants attempted to inch along impossibly narrow ledges, the penalty for error was falling. Results showed that across the lifespan, people consider falling to be a more severe penalty than getting stuck: Both younger and older adults made more conservative decisions when the penalty for error was falling, and older women were especially leery of falling. In both age groups, abilities and decisions were based on dynamic properties of the body, such as compressed body size in the doorway condition and balance in the ledge condition. Findings indicate that failure to perceive possibilities for action is unlikely to be the cause of the increased prevalence of falling in older adults.
Keywords: Affordances, Apertures, Falling, Perception, Judgments
Introduction
For a typical city-dweller, walking along the edge of a subway platform and squeezing through the closing doors of a train are everyday activities. Performing such actions may seem like a mundane accomplishment, but the underlying perceptual-motor processes are complex. To safely navigate the world, people must perceive affordances—the relations between the features of the environment and the characteristics of the body that make a particular action possible (Gibson 1979). For instance, doorways larger than a person's narrowest dimension afford passage, and doorways smaller than a person's narrowest dimension do not (Warren and Whang 1987).
Younger, college-age adults accurately perceive affordances, attempting possible actions and refusing impossible ones (Mark 1987; Warren and Whang 1987; Stoffregen et al. 2005; Higuchi et al. 2006; Ishak et al. 2008; Franchak et al. 2010; Franchak et al. 2012). They can even recalibrate to changes in affordances when their bodies are experimentally altered with “pregnancy” packs (Franchak and Adolph 2013), platform shoes (Mark et al. 1990; Stefanucci and Geuss 2010), tall helmets (Stefanucci and Geuss 2010), or padded gloves (Ishak et al. 2008). Whether older adults perceive affordances as accurately as younger adults is less certain, and of particular concern.
After young adulthood, possibilities for action change. In general, motoric and perceptual abilities decrease in old age and the range of possible actions contracts. Muscles weaken (Larsson et al. 1979), visual contrast deteriorates (Pitts 1982), and sensitivity of peripheral vision declines (Jaffe et al. 1986). With decreased sensitivity to visual and somatosensory input, postural sway increases and balance worsens (Woollacott 1993). These age-related changes can have grim consequences: About one-third of older adults over 65 years of age fall each year (Hausdorff et al. 2001). In addition, older adults are less able than younger adults to compensate for motor errors. After stumbling, older adults are more likely to fall, due to less effective compensatory responses (Schillings et al. 2004). Adults 65–74 years of age are more than twice as likely, compared to younger adults, to fall and to incur serious fall injuries, and adults more than 75-years-old are four times as likely (Adams et al. 2011). Although numerous studies document the decline in older adults' perceptual-motor skills, the question remains as to whether older adults are sensitive to their worsening abilities, and whether their motor decisions reflect the consequent changes in affordances.
One possibility is that older adults perceive affordances just as well as younger adults—or even better—and they make accurate motor decisions. For example, older adults, like college students, correctly matched the largest possible riser height for stair climbing to their abilities (Konczak et al. 1992; Cesari et al. 2003): What they judged they could do matched what they could actually do, taking into account the fact that their hip flexibility was substantially reduced and that they could not lift their legs as high as younger adults. In fact, older adults were slightly more accurate than younger adults when gauging affordances for stair climbing. Similarly, older adults were more accurate than younger adults when asked to estimate how far they could reach while standing and leaning forward (Robinovitch and Cronin 1999).
A second possibility is that older adults may perceive affordances accurately, but their motor decisions are overly conservative because they are more concerned than younger adults about the consequences of motor errors. Even younger adults are wary of actions that incur risk of physical injury. They duck at higher increments when running under a barrier than when walking under it (van der Meer 1997), and they are less willing to run under low barriers made of hard materials than soft ones (Wagman and Malek 2009). Penalties for error grow more severe with age. In 2008, 82 % of deaths due to falling were among adults age 65 and older (National Center for Injury Prevention and Control 2010). Thus, older adults might be more risk averse than younger adults because the penalties for poor motor decisions are harsher. In particular, older women are more likely than older men to report fear of falling (Vellas et al. 1997; Suzuki et al. 2002) and believe that they are at risk of osteoporosis (Nayak et al. 2010). Indeed, older women are more likely to be injured by a fall than older men (Stel et al. 2004). Fear of falling likely contributes to older women being more cautious than younger women when stepping onto, and down from a curb (Lythgo et al. 2007).
A third possibility is that older adults are worse at perceiving affordances than younger adults, causing their motor decisions to be more variable and/or less accurate than younger adults. In fact, older adults are more likely than younger adults to overestimate their abilities when crossing streets by underestimating the amount of time it would take them to get safely across (Oxley et al. 2005; Zivotofsky et al. 2012). Moreover, older adults overestimate the amount of space needed to walk through doorways—they turn their bodies to ft through doorways that are much wider than their shoulders, whereas younger adults scale their decisions to turn more closely to shoulder width (Hackney and Cinelli 2011). Older adults may be less accurate because their perceptual-motor systems are compromised. Being in motion provides information about the body's abilities: Younger adults who took a few running steps were better than stationary participants at judging their ability to catch a ball (Oudejans et al. 1996), and older adults who took a few walking steps toward a doorway were better than stationary participants when judging whether they could pass through the doorway (Hackney and Cinelli 2013a). Older adults are less physically active than younger adults, as evidenced by self-report (Schoenborn et al. 2004). Perception of affordances may be worse in older adults because they move less and move less effectively and therefore obtain impoverished information about the limits of their abilities. As a consequence of degraded information, older adults may also show more within-subject variability in estimating their own abilities.
Current study
The current study was designed to illuminate how—if at all—older and younger adults differ in motor abilities and decisions for action. Younger adults in their twenties and older adults age 60+ decided whether to walk through openings varying in size in two penalty conditions. In the doorway condition, participants decided whether to walk through doorways of varying widths. Turning sideways allowed passage through narrow doorways, but attempts to squeeze through impossibly small doorways resulted in entrapment. In the ledge condition, participants decided whether to walk along ledges of varying widths. Turning sideways allowed passage along narrow ledges, but attempts to walk along impossibly narrow ledges resulted in falling. The absence of a second wall in the ledge condition changed the affordances for passage. Whereas passage in the doorway condition should depend primarily on body size, passage in the ledge condition should also depend on participants' ability to keep balance (Franchak and Adolph 2012).
We estimated affordance thresholds (the smallest opening size that allowed passage) for each participant and compared motor decisions (attempts to pass through the openings) relative to their abilities (Franchak and Adolph in press). This experimental paradigm was used previously to test affordance thresholds and motor decisions in 17-month-olds (Franchak and Adolph 2012). Infants' thresholds were similar in both conditions, but their decisions were more accurate in the ledge condition, where the penalty was falling, than in the doorway condition where they became wedged on trial after trial.
We expected that younger adults would be more slender and spry than older adults and thus have smaller thresholds in both conditions. We also expected that adults, like infants, would be more reticent to err when the penalty was falling rather than entrapment, and that older adults might be especially wary of falling. We reasoned that if older adults perceive affordances as accurately as younger adults, then both age groups should attempt possible openings and reject impossible ones. If older adults' perception is accurate but their decisions are conservative relative to younger adults, older adults should refuse possible actions more frequently. And if older adults' perception is less accurate relative to younger, their decisions should be more variable and they may be more likely to overestimate their abilities.
Methods
Participants
We tested 25 younger adults (12 women, 13 men) between 20.0 and 27.4 years of age (M = 22.0) and 22 older adults (10 women, 12 men) between 60.1 and 83.1 years of age (M = 68.5). Participants were recruited through the departmental subject pool, word of mouth, and on-line classifieds; they received course credit or $10 as compensation. None had known physical or neurological disabilities, and all had normal or corrected-to-normal vision. Four younger adults and 11 older adults had previously experienced a serious fall requiring medical care or painkillers. Five additional people participated, but were excluded from analyses (4 due to experimenter error and 1 refused to follow experimental instructions).
Apparatus
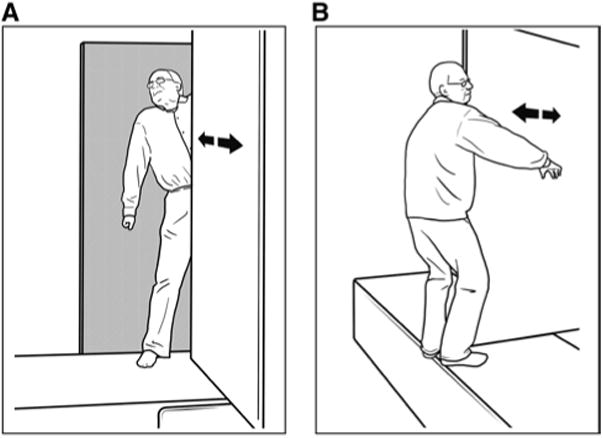
We observed participants' ability to squeeze through doorways and inch along narrow ledges on a specially constructed wooden apparatus (Fig. 1). A raised platform (4.9 m long × 0.98 m wide × 0.64 m high) lined with high-density foam was interrupted 3.0 m from the starting edge by a sliding wall. In the doorway condition, a stationary wall (1.22 m wide × 1.92 m high) was attached perpendicular to the sliding wall (1.12 m wide × 1.92 m high) to create doorways varying in width from 0 to 64 cm. In the ledge condition, the stationary wall was removed so that the sliding wall reduced the space available for passage as it moved toward the edge of the platform, creating ledges varying in width from 0 to 64 cm.
Fig. 1. Adjustable opening apparatus in (a) doorway and (b) ledge conditions. In the doorway condition, participants walked through bounded openings. In the ledge condition, participants walked along a ledge between the moving wall and a precipice.
We recorded participants' actions from two views: A stationary overhead camera focused on participants as they navigated the opening, and a panning side camera provided a continual view of participants' bodies during approach and passage. A miniature measurement camera attached to the sliding door projected to an external monitor to allow precise adjustment of the sliding wall. We combined the footage from these three cameras into a single video file with a playback rate of 30 frames/second.
Procedure
Half of the participants completed the doorway condition first, and half completed the ledge condition first. None wore shoes. They started each trial standing 2.5 m away from the door or ledge with their backs toward the opening. After the experimenter set the sliding wall to the appropriate width, participants turned to view the opening. We instructed participants to attempt passage if they thought it was possible and not to attempt if they thought it was impossible. Participants could take as much time as they wanted to attempt or refuse each opening, and they could make their decision from the starting line or at any point during their approach to the opening.
Pilot testing showed that in both conditions, participants could navigate smaller openings if they turned toward the sliding wall rather than away from it. To ensure that differences in abilities between participants were not due to differences in the direction they faced, we asked participants to face the sliding wall if they needed to turn. Pilot testing also showed that participants could navigate narrower ledges if they gripped the sliding wall for support. So, we told them not to hold onto the sliding wall. To ensure participants' safety, a spotter followed alongside the walkway; in addition, the floor alongside the platform was lined with gym mats covered with high-density foam.
As in Franchak and Adolph (2012), we used a modified psychophysical staircase procedure to ensure that most trials were presented in the region of interest around the affordance threshold. A staircase method is a standard psychophysical procedure that efficiently estimates a threshold or change point by using previous trial outcomes to guide future trial placement (Cornsweet 1962). The experimenter coded each trial online as a success (passed through the doorway or navigated along the ledge), failure (became stuck or fell), or refusal (did not attempt passage). Each condition started with a baseline opening size of 44 cm. Then, after each successful trial, the experimenter presented an opening 6 cm smaller, and after each failure or refusal, the experimenter presented an opening 4 cm larger, until converging on the smallest opening size with at least 2/3 successes. Occasionally, the experimenter presented clearly impossible or possible opening sizes to maintain participants' motivation and to prevent participants from tracking the staircase protocol. After the completion of the staircase protocol, the experimenter randomly presented opening sizes at ±1, ±3, ±6, and –9 cm around the participant's threshold width until accumulating at least 2 trials at each opening size. If participants did not spontaneously fail in a condition, we asked them to attempt smaller openings until they failed. Participants completed a total of 21–59 trials in each condition, M = 33; however, the requested attempts contributed only to analyses of affordance thresholds, not decision thresholds.
At the end of each session, we obtained two measures of participants' narrowest body dimensions—their static sagittal (from front to back) body size and their compressed sagittal body size. Participants stood on the apparatus with their backs against the stationary wall and the sliding door lined up with their sternum. To determine static body size, we moved the sliding door until it touched their stomach or chest. For compressed body size, we continued to apply pressure to the sliding door until it could not move further or participants said they were uncomfortable. All of the body size measurements for one older adult and compressed body size for one younger adult were not recorded due to experimenter error. The entire session took 45–60 min.
Data processing
A primary coder verified trial outcomes (successes, failures, and refusals) from video using a computerized coding software, Datavyu (datavyu.org). A second, reliability coder independently scored 25 % of the trials. Coders agreed on 97.5 % of trials (kappa = .95); disagreements were resolved through discussion.
As in Franchak et al. (2010), we modeled affordance and decision functions for each condition as Gaussian cumulative probability density functions using maximum likelihood estimates of the mu (threshold) and sigma (variability) parameters (for details, see Franchak et al. 2012). The affordance function characterized participants' ability to ft through openings based on their success rate at each opening size, S/(S + F). The decision function characterized their perception of whether they could ft through openings based on their attempt rate at each opening size (S + F)/(S + F + R). As illustrated in Fig. 2, thresholds were estimated at the 50 % point along each function. The discrepancy between the decision threshold and the affordance threshold provided a measure of decision error (dashed line in Fig. 2). The sigma parameters from each function were used to index variability in affordances and decisions across repeated trials.
Fig. 2.
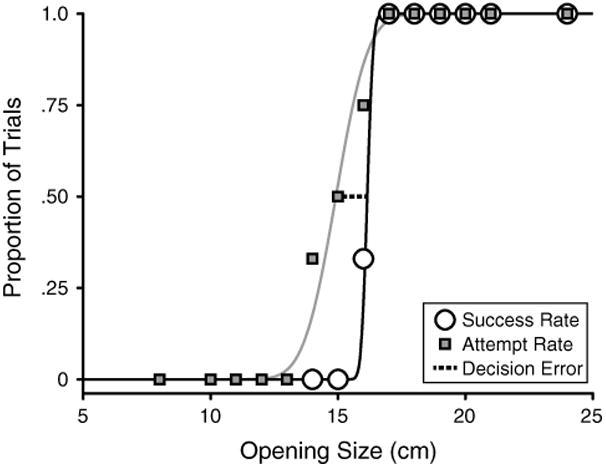
Affordance function (black curve) and decision function (gray curve) fit to a typical participant's attempts and decisions, respectively, in the doorway condition. Thresholds were estimated at the 50 % point of each function. Decision error is the difference between the two thresholds. This participant's decision threshold was smaller than her affordance threshold, indicating that she attempted some openings that were too small
Results
Preliminary analyses showed no effects of condition order or previous fall experience, so these variables were excluded from subsequent analyses.
Ten participants (7 older adults and 3 younger adults) did not spontaneously fail by attempting impossibly narrow openings in the ledge condition. So we asked them to attempt smaller openings until they failed. Three older women refused to participate in these additional trials because they did not want to fall from the ledge. Therefore, these three older adults were excluded from analyses of affordance thresholds.
Affordances and body dimensions
The spread of points along the y-axis in Fig. 3 denotes a wide range of affordance thresholds—14.5–33.9 cm for squeezing through doorways and 4.8–23.8 cm for navigating along ledges—affirming the importance of identifying abilities on an individual basis. In both conditions, all participants spontaneously turned sideways for narrower openings so that their sagittal body dimensions were the most relevant aspect of body size for determining affordances for passage. When attempting narrow doorways, participants typically moved one foot past the sliding wall then slowly squeezed their torsos into the opening as they pulled their heads through sideways. But passage in the ledge condition was not limited by body dimensions. In the ledge condition, participants inched toward the opening, then moved one foot around the sliding wall and slowly slid their torsos around the wall while balancing on the front of their feet with heels and buttocks hanging off the edge of the walkway. Some participants used their arms as ballasts by holding them parallel to the floor on either side of the sliding wall. Despite using different actions for passage in the two conditions, doorway and ledge thresholds were correlated for older r(18) = .84, p < .001, and younger adults r(24) = .48, p = .016. As apparent in the figure, differences in how participants performed the two actions resulted in larger thresholds in the doorway condition than the ledge condition (compare Fig. 3a, b) for both older (M difference between thresholds = 9.79 cm) and younger adults (M difference = 9.67 cm).
Fig. 3. Individual plots of participants' body dimensions and corresponding thresholds in each condition. The left panel shows static body dimensions, and the right panel shows dynamic body dimensions.
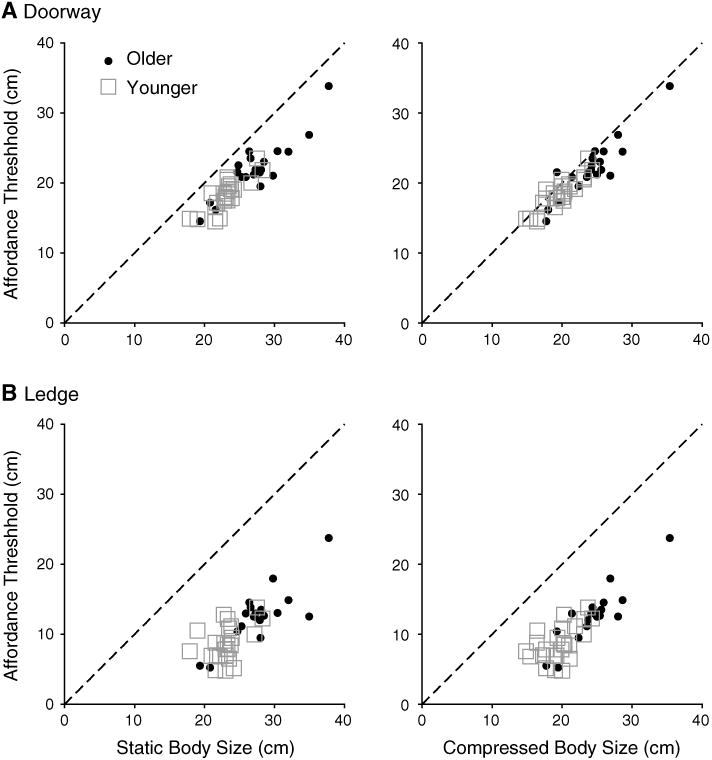
Because participants squeezed themselves through the doorways, we measured the sagittal width of their bodies with and without compression. The compressibility of participants' bodies ranged from 0.15 cm to 6.95 cm (M = 3.41 cm). Despite some overlap in body size between groups, Fig. 3 shows that older adults were larger than younger adults: older adults (Ms = 27.83 cm and 24.53 cm for static and compressed body size, respectively) and younger adults (Ms = 23.14 cm and 19.63 cm for static and compressed body size, respectively). One-way ANOVAs confirmed that older adults had larger compressed (F(1,40) = 23.45, p < .001) and static body dimensions (F(1,41) = 21.18, p < .001). Accordingly, as shown in Fig. 3, older adults had larger thresholds in the doorway and ledge conditions (Ms = 22.45 cm and 12.66 cm, respectively) compared with those of younger adults (Ms = 18.37 cm and 8.70 cm, respectively). A 2 (condition) × 2 (group) repeated measures ANOVA revealed main effects of condition, F(1,42) = 750.76, p < .001, partial η2 = .95, and group, F(1,42) = 20.47, p < .001, partial η2 = .33.
Across age groups, participants with smaller body dimensions tended to have smaller thresholds. In the doorway condition (Fig. 3a), static and compressed body size strongly predicted thresholds for older adults, r(17) = .90, p < .001, and r(17) = .90, p < .001, respectively, and younger adults, r(24) = .89, p < .001, and r(23) = .83, p < .001, respectively. Similarly, in the ledge condition (Fig. 3b), static and compressed body size strongly predicted thresholds for older adults, r(17) = .82, p < .001, and r(17) = .90, p < .001, respectively. However, the correlation between body size and opening size was smaller for ledge thresholds in younger adults, r(24) = .42, p = .038, r(23) = .55, p = .005 for static and compressed body size, respectively. A test of differences between correlation coefficients confirmed significantly higher correlations in the older adults as compared to younger adults for static body size and ledge threshold and for compressed body size and ledge threshold, Z = 2.12, p = .034 and Z = 2.57, p = .010, respectively.
Although body dimensions were reliable predictors of affordance thresholds, the relation was imperfect. For static body size in the doorway condition and for both static and compressed body size in the ledge condition, participants' thresholds were consistently smaller than their sagittal dimensions. As shown in Fig. 3, the points on these plots were consistently beneath the identity line. To examine which measure—static or compressed body size—better accounts for affordance thresholds, we calculated the difference between each measure and affordance thresholds, that is, the distance from the identity line. Static body size showed larger difference scores for doorway and ledge conditions (Ms = 5.03 cm and 14.70 cm, respectively) compared to compressed body size (Ms = 1.62 cm and 11.29 cm, respectively). A 2 (measure) × 2 (condition) × 2 (group) repeated measures ANOVA revealed main effects of condition, F(1,40) = 688.47, p < .001, partial η2 = .95, and measure, F(1,40) = 183.99, p < .001, partial η2 = .82. No other effects reached significance.
We examined the variability of performance across trials using the sigma parameters of each participant's affordance function. Trial outcomes were less variable in the doorway (M = 0.23 cm) than ledge condition (M = 1.25 cm). A 2 (condition) × 2 (group) repeated measures ANOVA revealed only a main effect of condition, F(1,42) = 14.83, p < .001, partial η2 = .26. Older adults were no more variable than younger.
Motor decisions
Of primary interest were potential differences in motor decisions between younger and older adults. Previous research showed that women are more fearful of falling than men (Vellas et al. 1997; Suzuki et al. 2002), which may be reflected in motor decisions when falling is a penalty. So, we included sex as an independent variable for analyses of motor decisions.
To quantify decision errors, we compared decision thresholds to affordance thresholds. Although we could not fit affordance functions to the data for the three older women who declined to fall, to exclude their data from analyses of decision errors would exclude the most cautious participants and consequently misrepresent the data. Therefore, we estimated affordance thresholds for these participants based on their body dimensions. We derived linear regression parameters that predicted older adults' ledge thresholds from their compressed body size. Using those parameters, we estimated affordance thresholds for the three older women and incorporated those thresholds into the subsequent analyses.
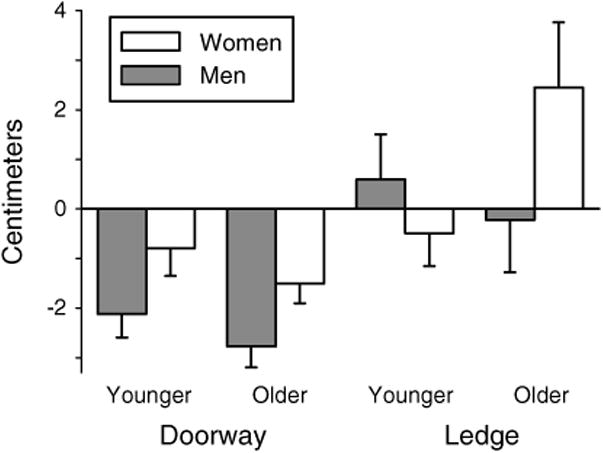
To determine the direction of participants' errors, we calculated signed decision error—the difference between participants' decision thresholds and affordance thresholds. Negative signed error denotes risky or liberal decision criteria, where participants attempted impossibly small openings. Positive signed error denotes cautious or conservative decision criteria, where participants refused to attempt possible openings. Figure 4 shows that participants were generally more cautious in the ledge condition (M = 0.50 cm) than in the doorway condition (M = −1.82 cm), and the effect was especially pronounced for older women. A 2 (condition) × 2 (group) × 2 (sex) repeated measures ANOVA confirmed a main effect of condition, F(1,43) = 24.60, p < .001, partial, η2 = .36. The condition × group × sex interaction was marginally significant F(1,43) = 3.94, p = .054. Follow-up Sidak-adjusted pairwise comparisons showed that in the ledge condition, older women were more cautious (M = 2.45 cm) than younger women (M = −0.50 cm), p = .049. There were no other significant differences. The condition × group × sex interaction was not significant if the most conservative older women (those who refused to fail in the ledge condition) were excluded from analyses.
Fig. 4. Decision error by sex, age, and condition. Error bars show 1 SE.
If participants are inconsistent in their decisions to attempt or refuse an opening, it may indicate that they have difficulty in perceiving affordances. Similar to affordance variability, we used the sigma parameters of the decision functions as a measure of decision variability. Participants were less variable in their decisions for the doorway condition (M = 0.91 cm) than for the ledge condition (M = 1.49 cm). A 2 (condition) × 2 (group) × 2 (sex) repeated measures ANOVA showed only a main effect of condition, F(1,43) = 8.19, p = .006, partial η2 = .16. Older adults were no more variable than younger.
Discussion
This study examined whether younger and older adults differ in their motor abilities and motor decisions. We observed participants in two tasks that involved navigating openings: walking through doorways and along ledges. The penalty for error—entrapment versus falling—was presumably more severe in the ledge condition, providing a way to determine whether decision errors arose from overly conservative response biases or failure to perceive affordances accurately.
Passage through doorways and along ledges
We designed the doorway and ledge conditions to present different penalties for error (entrapment and falling). This allowed us to determine whether younger and older adults take penalties into account when deciding whether to attempt passage. Both younger and older adults were cavalier in the doorway condition, frequently attempting doorways that were a few centimeters too small. They were more wary in the ledge condition, more closely matching attempts to their actual abilities. Falling is a salient penalty across the lifespan; indeed, infants are also more conservative when navigating ledges than trying to fit through doorways (Franchak and Adolph 2012).
Although infants showed similar affordance thresholds in doorway and ledge conditions (Franchak and Adolph 2012), they performed the actions differently and we expected adults to do likewise. Indeed, adults performed the two actions in strikingly different ways: Passage in the doorway condition involved wriggling and squeezing the body through the opening; on impossibly small doorways, participants became wedged based on the compressed size of their torsos. In contrast, passage in the ledge condition involved balancing on the toes with the backside hanging over the edge of the platform; agile participants could navigate ledges considerably smaller than their sideways body dimensions.
Previous work on locomotion through horizontal openings focused primarily on static body dimensions such as participants' shoulder width (Warren and Whang 1987; Wagman and Taylor 2005; Hackney and Cinelli 2011, 2013b), sagittal dimensions (Franchak et al. 2010), or stomach circumference (Franchak and Adolph 2013). However, squeezing through openings may depend more on dynamic body dimensions (Fath and Fajen 2011; Franchak et al. 2012; Franchak and Adolph in press) such as how much the body can compress. For example, fitting the hand through small openings depends on people's scrunched hand size (Ishak et al. 2008). In the current study, compressed sagittal dimensions more closely aligned with affordance thresholds in both conditions. In the doorway condition, the difference between compressed body size and affordance thresholds was close to 1 cm. However, in the ledge condition, participants could manage openings 10 cm smaller than their compressed body dimensions, indicating that although compressed body size is a strong predictor, balance likely accounts for a substantial portion of the remaining variance.
Since affordances for squeezing through doorways and navigating along ledges depended on dynamic factors, did adults' decisions take body dynamics into account? Previous work suggested that adults' motor decisions are based on static body geometry, presuming that static dimensions account for affordances (Warren 1984; Mark 1987; Warren and Whang 1987). When walking through doorways, if participants had used information about static body size, they would have underestimated their abilities by roughly 5 cm. Instead, they attempted doorways that were just slightly too small, thus more closely matching their compressed body size. In the ledge condition, neither static nor compressed body size accurately matched affordance thresholds. But participants attempted ledges that were much smaller than either body measure and matched their actual abilities, suggesting that decisions incorporated a dynamic property beyond their body size, likely balance. These findings are in accord with previous research that showed adults' decisions took the dynamic aspects of walking into account when judging whether they could pass through openings without turning or ducking (Franchak et al. 2012).
Although decision variability was similar for younger and older adults, variability differed between the two tasks. Decisions for both younger and older adults were more variable for ledges compared to doorways. Decision variability might depend on the variability of the affordance itself: Variability in individual affordance functions was higher in the ledge condition, indicating that balance-based performance was less consistent over trials. Previous research showed that participants are sensitive to variability in their own movements: They adjust the aim of rapid pointing actions to account for their own motor noise (Trommershäuser et al. 2008). Similar findings hold for navigating through openings (Franchak et al. 2012). Perceptual judgments of the ability to walk through horizontal openings, without turning, and vertical openings, without ducking, reflected variability in the actions: Actual gait modifications for walking through horizontal openings are more variable than for vertical openings.
The effects of aging
We found only two robust main effects of aging—both related to participants' bodies and motor skills. Older adults were generally wider from front to back than younger, and older adults had larger thresholds in both conditions. Larger thresholds in the doorway condition are clearly due to older adults' more portly figures. Larger thresholds in the ledge condition were again due to body size, but balance may have also been a factor. Possibly, older adults did not rely on balance to the same degree as younger adults. Evidence for this supposition is the stronger correlation between body size and ledge thresholds in older adults compared with younger adults. However, the similarity in affordance variability between younger and older adults calls this into question. Perhaps, older adults are more uniform as a group in their ability to balance than younger adults, thereby removing it as a source of threshold variance but still causing variability in action performance. Indeed, older adults' balance is deteriorating (Overstall et al. 1977; Woollacott 1993) which may act as an equalizer in balance ability among the group. However, since we did not directly assess balance, we can only speculate.
Although older adults were larger and less nimble than younger adults, we did not find evidence of a decrement in affordance perception due to aging: Analyses revealed no main effects of age for decision error or variability. As a group, older adults were not more cautious or more risky than younger—their signed error was similar to younger adults. This finding contradicts previous research showing general age decrements in older adults for judging possibilities for crossing a street (Oxley et al. 2005; Zivotofsky et al. 2012). One possible reason for this discrepancy is that the older adults in the previous work were, on average, several years older than the older adults in the current study. In support of this possibility, the 60- to 69-year-old participants in Oxley et al. (2005) were as accurate as the younger adults. Likewise, other studies that found similar affordance perception between younger and older adults included older adults whose ages were closer to our sample (Lobjois and Cavallo 2007; Konczak et al. 1992; Cesari et al. 2003). Moreover, in the current study, decision variability did not differ between age groups. We expected that if older adults were worse at perceiving affordances, they would have displayed more variability in their decisions, reflecting a lack of confidence and stability when judging whether an action is possible. The absence of a difference in variability, coupled with a lack of an age effect for decision errors, supports the hypothesis that older adults are not at a deficit when compared with younger adults in affordance perception.
Although we did not find main effects for age on decision thresholds, we did, however, find an interaction between age, sex, and condition. Overall, participants were more conservative in the ledge condition where the penalty for error was falling, but older women were especially cautious. They frequently refused to attempt ledges within their abilities. Why? A possible interpretation is that older women were less accurate at perceiving affordances and thus underestimated their abilities. However, findings from the doorway condition argue against this interpretation. If older women were worse at perceiving affordances in general, they should have also underestimated their abilities in the doorway condition. They did not. Additionally, three older women refused to risk falling in the ledge condition even when asked to do so, indicating that caution was guiding their decisions rather than poor affordance perception. This accords with previous research showing that older women are more cautious than older men when selecting a beam to walk across (Butler 2010), are more cautious than younger women when stepping on or off a curb (Lythgo et al. 2007), and report greater fear of falling than older men (Vellas et al. 1997; Suzuki et al. 2002).
The current study's lack of age effects in decisions leaves us with a puzzle: If older adults perceive affordances as well as younger adults, and older women are more cautious, then why do older adults fall more often than younger adults? And why are fall rates similar in older women and older men (Tinetti et al. 1988)? One possibility is that older adults detect potentially risky obstacles at the same rates as younger adults, but they are less able to recover from a slip or a trip (Lockhart et al. 2002) and thus fall more frequently. The most frequent causes of falls for older adults are weakness and problems with gait (Rubenstein et al. 1994). Therefore, falls frequently occur in situations that do not necessitate making a decision of whether the environment affords safe passage. The combination of weakening muscles and worsening balance can cause a fall when walking on fat ground or simply standing still, even though the ground affords walking and standing. Falling is not due to an error in perceiving affordances in such situations. Therefore, older adults still fall despite perceiving affordances accurately and unfortunately older women's extra caution may be in vain.
Conclusion
The current study shows that older adults can update their perception of affordances to take their changing bodies and skills into account. Affordances and the accurate perception thereof involve dynamic properties of the body. Additionally, falling is considered a worse penalty than entrapment throughout the lifespan, especially for older women. Findings suggest that the increased risk of falling in older adults is not due to a failure to perceive affordances.
Acknowledgments
This research was supported by National Institute of Health and Human Development Grant R37-HD33486 to Karen Adolph and a New York University Dean's Undergraduate Research Fund Grant to Angela Char.
References
- Adams P, Martinez M, Vickerie J, Kirzinger W. Summary health statistics for the US population: National Health Interview Survey, 2010. Vital Health Stat. 2011;10:1–117. [PubMed] [Google Scholar]
- Butler A. Action and ageing (Doctoral thesis, University of New South Wales, Sydney, Australia) 2010 [Google Scholar]
- Cesari P, Formenti F, Olivato P. A common perceptual parameter for stair climbing for children, young and old adults. Hum Mov Sci. 2003;22:111–124. doi: 10.1016/s0167-9457(03)00003-4. [DOI] [PubMed] [Google Scholar]
- Cornsweet TN. The staircase-method in psychophysics. Am J Psychol. 1962;75:485–491. [PubMed] [Google Scholar]
- Fath AJ, Fajen BR. Static and dynamic visual information about the size and passability of an aperture. Perception. 2011;40:887–904. doi: 10.1068/p6917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, Adolph KE. What infants know and what they do: perceiving possibilities for walking through openings. Dev Psychol. 2012;48:1254–1261. doi: 10.1037/a0027530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, Adolph KE. Gut Estimates: pregnant women perceive possibilities for walking through doorways. Manuscript under review. 2013 doi: 10.3758/s13414-013-0578-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, Adolph KE. (in press) Affordances for action as probabilistic functions: Implications for development, perception, and decision-making. Ecol Psychol. doi: 10.1080/10407413.2014.874923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, van der Zalm D, Adolph KE. Learning by doing: action performance facilitates affordance perception. Vis Res. 2010;50:2758–2765. doi: 10.1016/j.visres.2010.09.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, Celano EC, Adolph KE. Perception of passage through openings cannot be explained geometric body dimensions alone. Exp Brain Res. 2012;223:301–310. doi: 10.1007/s00221-012-3261-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson JJ. The ecological approach to visual perception. Houghton Miffin Company; Boston: 1979. [Google Scholar]
- Hackney AL, Cinelli ME. Action strategies of older adults walking through apertures. Gait Posture. 2011;33:733–736. doi: 10.1016/j.gaitpost.2011.02.019. [DOI] [PubMed] [Google Scholar]
- Hackney AL, Cinelli ME. Older adults are guided by their dynamic perceptions during aperture crossing. Gait Posture. 2013a;37:93–97. doi: 10.1016/j.gaitpost.2012.06.020. [DOI] [PubMed] [Google Scholar]
- Hackney AL, Cinelli ME. Young and older adults use body-scaled information during a non-confned aperture crossing task. Exp Brain Res. 2013b;225:419–429. doi: 10.1007/s00221-012-3382-3. [DOI] [PubMed] [Google Scholar]
- Hausdorff JM, Rios DA, Edelber HK. Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch Phys Med Rehabil. 2001;82:1050–1056. doi: 10.1053/apmr.2001.24893. [DOI] [PubMed] [Google Scholar]
- Higuchi T, Cinelli ME, Greig MA, Patla AE. Locomotion through apertures when wider space for locomotion is necessary: adaptation to artificially altered body states. Exp Brain Res. 2006;175:50–59. doi: 10.1007/s00221-006-0525-4. [DOI] [PubMed] [Google Scholar]
- Ishak S, Adolph KE, Lin GC. Perceiving affordances for fitting through apertures. J Exp Psychol Hum Percept Perform. 2008;34:1501–1514. doi: 10.1037/a0011393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaffe GJ, Alvarado JA, Juster RP. Age-related changes of the normal visual field. Arch Ophthalmol. 1986;104:1021–1025. doi: 10.1001/archopht.1986.01050190079043. [DOI] [PubMed] [Google Scholar]
- Konczak J, Meeuwsen HJ, Cress ME. Changing affordances in stair climbing: the perception of maximum climbability in young and older adults. J Exp Psychol Hum Percept Perform. 1992;18:691–697. doi: 10.1037//0096-1523.18.3.691. [DOI] [PubMed] [Google Scholar]
- Larsson L, Grimby G, Karlsson J. Muscle strength and speed of movement in relation to age and muscle morphology. J Appl Physiol Respir Environ Exerc Physiol. 1979;46:451–456. doi: 10.1152/jappl.1979.46.3.451. [DOI] [PubMed] [Google Scholar]
- Lobjois R, Cavallo V. Age-related differences in street-crossing decisions: the effects of vehicle speed and time constraints on gap selection in an estimation task. Accid Anal Prev. 2007;39:934–943. doi: 10.1016/j.aap.2006.12.013. [DOI] [PubMed] [Google Scholar]
- Lockhart TE, Woldstad JC, Smith JL, Ramsey JD. Effects of age related sensory degradation on perception of floor slipperiness and associated slip parameters. Saf Sci. 2002;40:689–703. doi: 10.1016/S0925-7535(01)00067-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lythgo N, Begg R, Best R. Stepping responses made by elderly and young female adults to approach and accommodate known surface height changes. Gait Posture. 2007;26:82–89. doi: 10.1016/j.gaitpost.2006.07.006. [DOI] [PubMed] [Google Scholar]
- Mark LS. Eyeheight-scaled information about affordances: a study of sitting and stair climbing. J Exp Psychol Hum Percept Perform. 1987;13:361–370. doi: 10.1037//0096-1523.13.3.361. [DOI] [PubMed] [Google Scholar]
- Mark LS, Baillet JA, Craver KD, Douglas SD, Fox T. What an actor must do in order to perceive the affordance for sitting. Ecol Psychol. 1990;2:325–366. [Google Scholar]
- National Center for Injury Prevention and Control CDC. Webbased injury statistics query and reporting system (WISQARS) 2010;2010 [Google Scholar]
- Nayak S, Roberts MS, Chang CH, Greenspan SL. Health beliefs about osteoporosis and osteoporosis screening in older women and men. Health Educ J. 2010;69:267–276. doi: 10.1177/0017896910364570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oudejans RR, Michaels CF, Bakker FC, Dolne MA. The relevance of action in perceiving affordances: perception of catchableness of fly balls. J Exp Psychol Hum Percept Perform. 1996;22:879–891. doi: 10.1037//0096-1523.22.4.879. [DOI] [PubMed] [Google Scholar]
- Overstall P, Exton-Smith A, Imms F, Johnson A. Falls in the elderly related to postural imbalance. Br Med J. 1977;1:261–264. doi: 10.1136/bmj.1.6056.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oxley J, Ihsen E, Fildes B, Charlton J, Day R. Crossing roads safely: an experimental study of age differences in gap selection by pedestrians. Accid Anal Prev. 2005;37:962–971. doi: 10.1016/j.aap.2005.04.017. [DOI] [PubMed] [Google Scholar]
- Pitts DG. The effects of aging on selected visual function: dark adaptation, visual acuity, stereopsis and brightness contrast. In: Sekuler R, Kline DW, Dismukes K, editors. Aging and Human Visual Function. A. R. Liss; New York: 1982. pp. 131–159. [Google Scholar]
- Robinovitch S, Cronin T. Perception of postural limits in elderly nursing home and day care participants. J Gerontol Ser A Biol Sci Med Sci. 1999;54:124–130. doi: 10.1093/gerona/54.3.b124. [DOI] [PubMed] [Google Scholar]
- Rubenstein L, Josephson K, Robbins A. Falls in the nursing home. Ann Intern Med. 1994;121:442–451. doi: 10.7326/0003-4819-121-6-199409150-00009. [DOI] [PubMed] [Google Scholar]
- Schillings AM, Mulder T, Duysens J. Stumbling over obstacles in older adults compared to younger adults. J Neurophysiol. 2004;94:1158–1168. doi: 10.1152/jn.00396.2004. [DOI] [PubMed] [Google Scholar]
- Schoenborn CA, Adams PF, Barnes PM, Vickerie JL, Schiller JS. Health behaviors of adults: United States, 1999–2001. Vital Health Stat. 2004;10:1–79. [PubMed] [Google Scholar]
- Stefanucci JK, Geuss MN. Duck! Scaling the height of a horizontal barrier to body height. Atten Percept, Psychophys. 2010;72:1338–1349. doi: 10.3758/APP.72.5.1338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stel VS, Smit JH, Pluijm SMF, Lips P. Consequences of falling in older men and women and risk factors for health service use and functional decline. Age Ageing. 2004;33:58–65. doi: 10.1093/ageing/afh028. [DOI] [PubMed] [Google Scholar]
- Stoffregen TA, Yang C, Bardy BG. Affordance judgments and nonlocomotor body movement. Ecol Psychol. 2005;17:75–104. [Google Scholar]
- Suzuki M, Ohyama N, Yamada K, Kanamori M. The relationship between fear of falling, activities of daily living and quality of life among elderly individuals. Nurs Health Sci. 2002;4:155–161. doi: 10.1046/j.1442-2018.2002.00123.x. [DOI] [PubMed] [Google Scholar]
- Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319:1701–1707. doi: 10.1056/NEJM198812293192604. [DOI] [PubMed] [Google Scholar]
- Trommershäuser J, Maloney LT, Landy MS. Decision making, movement planning, and statistical decision theory. Trends Cognit Sci. 2008;12:291–297. doi: 10.1016/j.tics.2008.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van der Meer ALH. Visual guidance of passing under a barrier. Early Dev Parent. 1997;6:149–157. [Google Scholar]
- Vellas BJ, Wayne SJ, Romero LJ, Baumgartner RN, Garry PJ. Fear of falling and restriction of mobility in elderly fallers. Age Ageing. 1997;26:189–193. doi: 10.1093/ageing/26.3.189. [DOI] [PubMed] [Google Scholar]
- Wagman J, Malek E. Geometric, kinetic-kinematic, and intentional constraints influence willingness to pass under a barrier. Exp Psychol. 2009;56:409–417. doi: 10.1027/1618-3169.56.6.409. [DOI] [PubMed] [Google Scholar]
- Wagman JB, Taylor KR. Perceiving affordances for aperture crossing for the person-plus-object system. Ecol Psychol. 2005;17:105–130. [Google Scholar]
- Warren WH. Perceiving affordances: visual guidance of stair climbing. J Exp Psychol Hum Percept Perform. 1984;10:683–703. doi: 10.1037//0096-1523.10.5.683. [DOI] [PubMed] [Google Scholar]
- Warren WH, Whang S. Visual guidance of walking through apertures: body-scaled information for affordances. J Exp Psychol Hum Percept Perform. 1987;13:371–383. doi: 10.1037//0096-1523.13.3.371. [DOI] [PubMed] [Google Scholar]
- Woollacott MH. Age-related changes in posture and movement. J Gerontol. 1993;48:56–60. doi: 10.1093/geronj/48.special_issue.56. [DOI] [PubMed] [Google Scholar]
- Zivotofsky A, Eldror E, Mandel R, Rosenbloom T. Misjudging their own steps: why elderly people have trouble crossing the road. Hum Factors. 2012;54:600–607. doi: 10.1177/0018720812447945. [DOI] [PubMed] [Google Scholar]