

Abstract
Pasteurella multocida is an inhabitant of the oral cavity of a variety of livestock and domestic pet species, especially cats and dogs. The case reported illustrates a 60-year-old, immunocompetent female patient who presented with P. multocida sepsis and aortic valve endocarditis. This required surgical bioprosthetic aortic valve replacement. Investigation also found infection-induced rhabdomyolysis and permanent hearing loss, both previously unassociated with P. multocida infection.
Keywords: Endocarditis, Pasteurella multocida, Rhabdomyolysis
1. Introduction
Pasteurella multocida is found worldwide and is a small, Gram-negative, coccobacillus. It often exists as a normal flora in the upper respiratory tracts of fowls and domesticated species, especially felines and dogs.1 P. multocida can cause infections in humans, usually as results of cat scratches, or cat or dog bites. In this report, we discuss a case of P. multocida induced endocarditis infecting an immunocompetent patient, further complicated by rhabdomyolysis and permanent hearing loss.
2. Case report
A 60-year-old female without a significant past medical history presented with altered mental status preceded by a week history of fever, chills, and generalized malaise and weakness. The patient lives alone, has dogs and cats at home, and denied any animal bite. On physical examination, she was confused and disoriented. The patient was hypoxic (oxygen saturation 90% on room air), tachypneic, and tachycardic with a heart rate of 110 beats per minute. She was noted to be febrile with a temperature of 100.7 °F. Her blood pressure was a borderline 88/50 mmHg.
Gingivostomatitis was observed at the base of the tongue and around the lips. Also observed was a large area of skin ulceration (10 × 10 cm) surrounded by vesicles above the buttocks. There was no obvious skin lesion to suggest a recent or remote animal bite. She had right hip swelling and tenderness. The patient was also noted to have a diastolic murmur at the right upper sternal border.
Laboratory studies revealed mild leukocytosis with a left shift and thrombocytopenia. Her creatine phosphokinase (CPK) level was elevated 10 times more than normal, with an increased lactate dehydrogenase (LDH) level of 684 IU/L. There was evidence of acute renal failure with a creatinine level of 5.3 mg/dL (creatinine clearance of 15 mL/min). Blood cultures grew P. multocida sensitive to penicillin. Her urine tested positive for hemoglobin and bacteria. A lumbar puncture was not performed due to patient refusal.
A clinical diagnosis of P. multocida sepsis and acute renal failure secondary to rhabdomyolysis was made. In addition, the patient suffered sudden onset hearing loss without evidence of tinnitus or vertigo. After taking aggressive fluid resuscitation and a course of ampicillin/sulbactam, the patient's renal function improved within a few days. A specimen of joint aspiration from the patient's right hip was collected for a culture. However, the culture was unrevealing. Screenings for human immunodeficiency virus (HIV), Hepatitis B and C, and varicella zoster virus (VZV) were all negative. The viral vesicular culture was also unremarkable. Audiological evaluation of the patient showed severe to profound sensorineural hearing loss in both ears.
A transthoracic echocardiogram showed severe aortic regurgitation with decreased left ventricular ejection fraction of 40%. A subsequent transesophageal echocardiogram demonstrated a mobile echodensity on the non-coronary cusp of the aortic valve prolapsing into the left ventricle outflow tract (Fig. 1). There was severe aortic valve regurgitation associated with holodiastolic flow reversal in the descending thoracic aorta (Fig. 2). The echocardiographic findings along with the patient's blood culture results are consistent with aortic valve endocarditis.
Fig. 1.
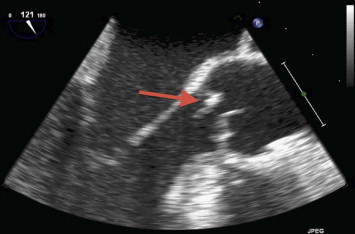
Transesophageal echocardiogram demonstrating (arrow) a mobile echodensity on the non-coronary cusp of the aortic valve prolapsing into the left ventricle outflow tract.
Fig. 2.
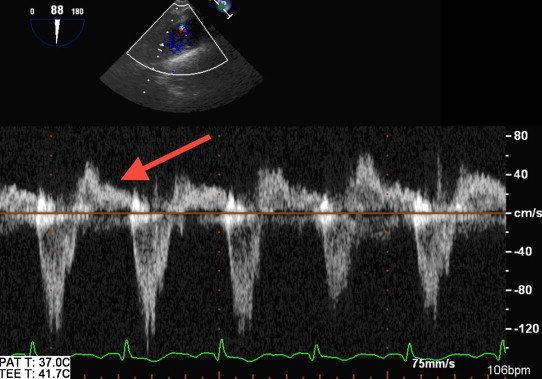
Spectral Doppler image showing (arrow) holodiastolic flow reversal in the descending thoracic aorta consistent with severe aortic insufficiency.
The patient underwent successful aortic valve replacement with a prosthetic valve. Intraoperatively, vegetations were seen on the aortic valve with extensive valvular destruction.
The postoperative course was uneventful. However, hearing loss was not improved despite steroids treatment.
3. Discussion
Infection from P. multocida can be divided into three categories. The first being cellulitis, which can lead to necrotizing soft tissue infections. Infection can also happen in the case of oral and respiratory infections, usually in the setting of chronic pulmonary disease. Finally, seriously invasive infections (often unrelated to animal bites) can lead to sepsis, meningitis, intra-abdominal infection, septic arthritis, osteomyelitis, and endocarditis.
Endocarditis is a rare complication of P. multocida sepsis, with 33 cases having been reported in the literature.1,2 Most patients have predisposing diseases including diabetes mellitus, liver dysfunction, or other immunocompromising illnesses.3
Most commonly, P. multocida induced endocarditis affects prosthetic valves in immunocompromised patients. There are several articles reported with P. multocida induced endocarditis involving native heart valves, but all the patients had predisposing medical conditions.4,5
In our patient, endocarditis affected her native aortic valve. Similar to previously reported cases of native heart valve endocarditis, she was treated with a full course of intravenous antibiotics and a prosthetic valve replacement.6 It is also important to carefully perform wound assessment in case animal bites or scratches exist. Meticulous wound irrigation and debridement, as well as wound closure in appropriate cases will often help eradicate infection.
However, associated rhabdomyolysis and permanent hearing deficiency were never previously reported in relation to P. multocida infection. Though the exact causes of these symptoms are not known, it might be possible that permanent hearing loss was related to undiagnosed meningitis. We hypothesize that catalase, oxidase and cytotoxin (for example, capsular lipopolysaccharide) released by P. multocida led to extensive skeletal muscle and nerve damage. This phenomenon may be mediated by cytotoxin specific receptors located in these tissues.
Conflicts of interest
All authors have none to declare.
References
- 1.Khan M.F., Movahed M.R., Jung J. Pasteurella multocida endocarditis. J Heart Valve Dis. 2012;21:260–262. [PubMed] [Google Scholar]
- 2.Naba M.R., Araj G.F., Kanafani Z.A., Kanj S.S. First case of Pasteurella multocida endocarditis of the tricuspid valve: a favorable outcome following medical treatment. Int J Infect Dis. 2009;13:e267–e269. doi: 10.1016/j.ijid.2008.11.004. [DOI] [PubMed] [Google Scholar]
- 3.Drenjancevic I.H., Ivic D., Drenjancevic D., Ivic J., Pelc B., Vukovic D. Fatal fulminant sepsis due to a cat bite in an immunocompromised patient. Wien Klin Wochenschr. 2008;120:504–506. doi: 10.1007/s00508-008-0992-7. [DOI] [PubMed] [Google Scholar]
- 4.Graf S., Binder T., Heger M., Apfalter P., Simon N., Winkler S. Isolated endocarditis of the pulmonary valve caused by Pasteurella multocida. Infection. 2007;35:43–45. doi: 10.1007/s15010-007-5074-7. [DOI] [PubMed] [Google Scholar]
- 5.Fukumoto Y., Moriyama Y., Iguro Y., Toda R., Taira A. Pasteurella multocida endocarditis: report of a case. Surg Today. 2002;32:513–515. doi: 10.1007/s005950200087. [DOI] [PubMed] [Google Scholar]
- 6.Fayad G., Modine T., Mokhtari S. Pasteurella multocida aortic valve endocarditis: case report and literature review. J Heart Valve Dis. 2003;12:261–263. [PubMed] [Google Scholar]