

Abstract
There is increasing attention to medical problems of musicians. Many studies find a high prevalence of work-related musculoskeletal disorders in musicians, ranging from 73.4% to 87.7%, and string players have the highest prevalence of musculoskeletal problems. This paper examines the various positions and movements of the upper extremities in string players: 1) basic postures for holding instruments, 2) movements of left upper extremity: fingering, forearm posture, high position and vibrato, 3) movements of right upper extremity: bowing, bow angles, pizzicato and other bowing techniques. These isotonic and isometric movements can lead to musculoskeletal problems in musicians. We reviewed orthopedic disorders that are specific to string players: overuse syndrome, muscle-tendon syndrome, focal dystonia, hypermobility syndrome, and compressive neuropathy. Symptoms, interrelationships with musical performances, diagnosis and treatment of these problems were then discussed.
Keywords: Upper extremities, String players, Musculoskeletal problems
INTRODUCTION
Work-related medical problems in musicians have received increasing attention in recent years. This is because 1) the prevalence of playing-related disorders has increased with the growth of music industry, 2) epidemiological studies consistently support an increased prevalence of medical problems of musicians, 3) occupational medicine is engaged in active research on occupational overuse syndrome, and 4) medicine for musicians is currently being established as a specialty. This specialized medical field is called 'Musicians' Medicine' in English and 'Musikermedizin' in Germany. When it includes vocalists and dancers, as well, it is referred to as 'Performing Arts Medicine' in English and 'Medecine des Arts' in French. The establishment of these terms shows that there is vigorous research in this area in many countries.
Musicians can be classified as instrumentalists and non-instrumentalists. The medical problems of instrumentalists include those that are caused directly by playing the instrument, and those that are unrelated to playing. The latter include incidental accidents and problems caused by activities of daily life.
The present article focuses on the playing-related medical issues of string players. Playing an instrument demands repetitive precise and/or delicate movements in prolonged non-ergonomic posture. This process makes musicians susceptible to musculoskeletal disorders.
Given the growing interest in the musculoskeletal problems of musicians, academic musicians' medicine societies have been organized, and clinics specializing in treating professional players and students have been established in the United States and Europe. As a result, the demand for musicians' medicine has increased in every country. However, there are few studies on musicians' musculoskeletal problem. We will provide basic information about playing string instruments, after which the orthopedic disorders that are specific to string players will be discussed.
OVERVIEW OF MUSICIANS' MEDICINE
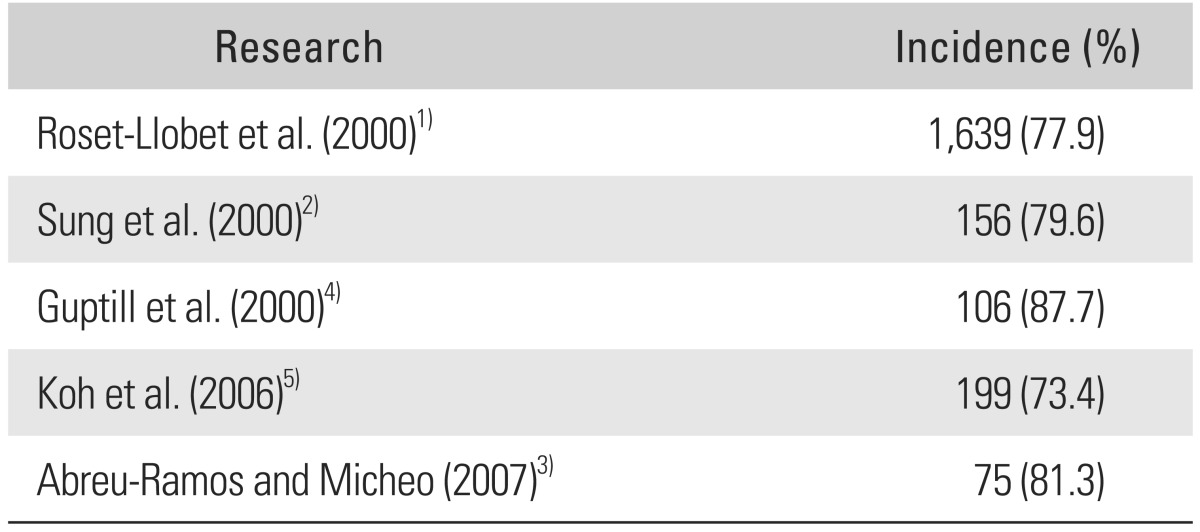
The prevalence of musculoskeletal disorders in instrumentalists is relatively high, ranging from 73.4% to 87.7% (Table 1).1-5) At least 75% experience upper extremity symptoms, most of which relate to overuse.6) A study by Roset-Llobet et al.1) showed that 77.9% of instrumentalists had playing-related symptoms and 37.3% were affected by the symptoms in their performance. A survey in Korea revealed that 79.6% of orchestral players had musculoskeletal disorders and the most frequently affected body parts were the shoulders (59.6%) and back (48.1%).2)
Table 1.
Prevalence of Playing Related Musculoskeletal Disorder in String Players
The stress-inducing movements in playing can be divided into two categories: 1) isotonic movements: these are sophisticated and fast movements that are designed to produce sound (these movements include touching the fingerboard, playing the piano or keyboard and bowing); and 2) isometric movement: these movements serve to stabilize the instruments for prolonged periods in unstable postures. Repetitive movements associated with increased muscle activity that stabilizes the wrist, elbow and shoulder girdle load stress on the surrounding tendons; over time, this can lead to pain due to chronic tendinopathy.7) In addition, prolonged maintenance of a static posture where the shoulders and neck are elevated or fixed laterally to hold instruments results in muscle imbalance, which may progress to chronic myofascial pain.8)
To specify by instruments, violinists and violists complain frequently of neck and upper extremity pain because of their posture, which involves holding their instrument between chin and shoulder, flexing their elbow with extreme supination of the forearm and wrist for prolonged periods, and repetitive bowing with the right arms. Contrabassists complain of back pain because they have to stabilize their instruments with their trunk and play with their trunk leaned forward. Pianists often present pain around the scapula and wrist due to overuse. Clarinetists and oboists often complain of symptoms on the joint of the right thumb especially at the metacarpophalangeal joint, because they hold their instruments mostly with their right thumbs. Flutists usually complain of left neck, shoulder and wrist pain due to the non-ergonomic playing shoulder abduction position. Percussionists may have left wrist symptoms due to the repeated snapping of the wrists and fingers.
Various methods have been used to treat musculoskeletal symptoms of instrumentalists. In some cases, rest and medication such as analgesics or non-steroidal anti-inflammatory drugs (NSAIDs) with adjunct treatment such as physical therapy (ice or hot pack, transcutaneous electrical stimulation, ultrasound) should be considered first. These can alleviate symptoms enough to return to the previous healthy condition.9) If symptoms are severe, such as in overuse syndrome, absolute rest is needed.10) In cases where there is no response to pain control management, rehabilitation may be helpful. This involves stretching and strengthening exercise for stabilizing the muscles of the symptomatic areas; surface electromyogram (EMG) that helps to relax unnecessarily contracted muscles while playing; and the exercise called 'Groningen Exercise' have been developed for the symptomatic musicians.11-13) Surgical treatment should be considered in the case with nerve compression syndromes or the degenerative conditions when the non-surgical treatment fails.14)
MEDICAL PROBLEMS OF STRING PLAYERS
String instruments are the generic term of the instruments that make sound with the vibration of strings. Although they include guitars, harps, pianos in the broad meaning, the violin family; violin, viola, cello, and contrabass, which are most widely used in modern orchestra will be the focus of this article. This section will describe how musicians play these instruments and which playing-related medical problems can develop.
The instruments in the violin family have a similarly shaped body and four strings. The strings are located on the fingerboard and there is a bridge beneath the strings to raise them. They have a common feature of playing method: place left fingertips on the fingerboard to decide the pitch, and right hand to hold a bow and move it to make a sound. The fact that each hand has different roles is a distinguishing feature of strings from wind, keyboard and percussion instruments.
Characteristics of the Playing of Stringed Instruments
Basic posture
Although soloists of violin or viola may play standing, the majority of orchestra players sit. Violins and violas are placed between left shoulder and chin, and there can be a shoulder rest and a chin rest to assist the placement. Left hand holds the instrument gently, as left fingers needs to move freely to pinch the note. The right thumb, middle and ring finger grip the bow and the index and little finger are placed gently on the bow. The right thumb should not be extended, as it may cause more stress and muscle tension. Cellists always play sitting. The body of cello is placed between the player's knees while the fingerboard is at the left side of head, and an endpin is used to support the instrument. The finger position and bow grab are similar to violin and viola. Contrabass players in orchestra may sit on a high stool or stand due to the size of the instrument. Back pain is major complaint of contrabassist, as they often need to bend their backs during the whole performance. Also carrying basses may be a risk factor for back pain. The grip of the bow in contrabass is different from other strings; bass players grip bow with supine position of forearm.
Movement of left upper extremity
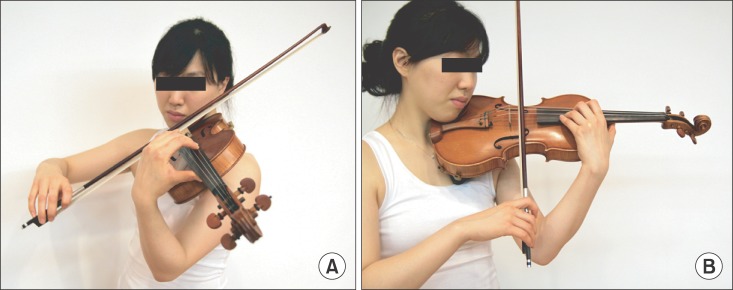
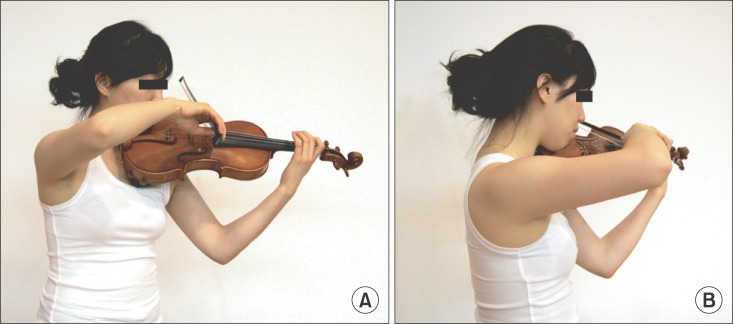
Left hand regulates the length of the strings by pressing the strings, thus pinching a note. This is called 'fingering'. String players press the string in a highly precise manner so that the right pitches are achieved consistently; by contrast, pianists or wind players play fixed notes. Therefore, string players have to keep their left fingers as vertical as possible to minimize the dispersion of the sound (Fig. 1). To make high tones, players place their fingertip on the fingerboard near the bridge by controlling their elbow and forearm: this is called 'high position' (Fig. 2). This can require the hyperflexion of the player's left elbow and wrist and the forearm can be extremely supinated. When they play music that requires fast and repetitive movements between high position and low position for an extended period, forearm pain can develop. The vibrato, the vibration sound generated by wrist and finger joints movements, can result in the wrist and finger joint symptoms.
Fig. 1.

Basic posture of the violist's left upper extremity. (A) An anterior view of the basic posture of the violinist's left hand and wrist. (B) The left fingers have to be as vertical as possible to minimize the dispersion of the sound.
Fig. 2.
When the players make high tones, they place their fingertips on the fingerboard near the bridge by controlling their elbow and forearm, which is called 'high position'. (A) A photograph showing the left elbow and wrist are hyperflexed. (B) A photograph showing the forearm is extremely supinated.
Movement of right upper extremity
The right hand holds the bow and makes sound by inducing friction of the strings: this is called 'bowing'. Unlike the left hand, the range of motion of the right upper extremity is wide, as the players are sometimes required to use the entire bow. In this process, extreme movements of upper extremity may lead to joint problems. 'Pizzicato' is a way to make a sound by plucking strings, without bow. This may cause a joint problem of right fingers. Each of four strings is played with their own bow angles so that only one string vibrates at a time. When a player bows the string on the left side of the player, it is necessary to abduct and internally rotate the shoulder (Fig. 3). When players are required to play quickly under the conditions described above, accumulation of stress can make microdamage to tendons. When the players lose control of their posture because they have to produce difficult notes or use demanding bowing techniques (staccato, spiccato, portato, etc.), the activities of the shoulder and forearm muscles increase and the players use wrist snapping unnecessarily. This can aggravate symptoms of the right extremity.
Fig. 3.
When players bow the strings located on the left side of the players, the elevation and rotation of the shoulder is demanded. (A) An anterior view of the right upper extremity. (B) A lateral view of the right upper extremity.
Diseases in String Players
The musicians' diseases can be divided into organic and non-organic problems. In organic problems, there can be tenosynovitis, hypermobility syndrome (HMS), arthritis and so on. On the other hand, non-organic problems such as overuse syndrome and focal dystonia, are more work-related. These lack specific treatment and are generally treated conservatively.
Lockwood6) reported that overuse syndrome is the most common cause of upper extremity symptoms related to playing. Winspur and Parry15) reported that there was a definite diagnosis in 41%, technical cause in 40%, and mental, emotional cause in 19% after evaluating the diagnoses of 617 instrument players who visited the hand surgery center. The definite diagnoses were hypermobility syndrome (10%), old injury (9%), tenosynovitis (6%), frozen shoulder (6%). Other diagnoses were osteoarthritis, thoracic outlet syndrome and rheumatoid arthritis, which can be easily detected by standard examinations. According to Dawson,16) muscle-tendon strain was the most common disease after evaluating the diagnosis of 167 players who underwent hand surgical practice.
Overuse syndrome
Also known as repetitive strain injury or cumulative trauma disorder, overuse syndrome was first chosen to explain the symptoms of musicians. The term of overuse syndrome is applied when there are work-related muscle and ligament symptoms associated with weakness, loss of control or speed, but objective lesions are not found.17) It is regarded as the result of fatigue from accumulative physical stress imposed by the overuse of particular parts of the body. It is different from tendinitis in the way that there is only tenderness and functional decrease, but no organic problems.11,18) Indeed, overuse syndrome holds an important place in musicians' medicine because the prevalence of organic problems such as tenosynovitis is relatively low in professional musicians.16) When the symptoms of overuse syndrome are not severe, conservative treatment may be helpful, but absolute rest is important in severe symptoms.10)
Muscle-tendon syndrome
Mechanical stress from sudden, abnormal or unfamiliar movements can result in micro-damage and inflammatory reaction of the tendon. The disease category including tendinitis, tenosynovitis, peritendinitis and so on which involves tendon thickness and the locking (trigger finger) phenomenon, is called muscle-tendon syndrome.19) The most common cause is overexertion caused by excessively fast movements or movements that stress the muscle tendon unit. Blunt trauma or sprain can also cause muscle-tendon syndrome.19) A study by Parry20) showed that only 12% of 507 musicians who had a particular diagnosis had tenosynovitis. Most cases were the result of carrying heavy instruments such as tuba or other activities not related to playing. Since inflammation conditions in string players are not always caused by repetitive movement during playing, it is important to consider this when diagnosing muscle-tendon syndrome.
Focal dystonia
Among the medical problems of musician, focal dystonia is one of the most serious and difficult medical condition to cure. Focal dystonia is characterized by abnormal involuntary sustained muscle contractions in single body part and is task-specific.21) Focal task-specific dystonia is a work-related condition because it is the result of a particular movement that is repeated forcefully over a long period. The etiology is not yet known. Although the prevalence of focal dystonia in professional musicians is only 1%, this can be frustrating in playing careers; only 38% of musicians can continue playing despite treatment.22,23) In string players, the loss of control and involuntary movements of the left fingers are the most common symptoms.23) Active management may be challenging because this can deteriorate playing skill. Medications such as antagonist to basal ganglia or muscle relaxant are advised. The strong possibility that this has psychogenic origins should be kept in mind. Reestablishment of sensorimotor organization by proprioception training can be conducted and Botox injection can be one of the treatment options.24)
Hypermobility syndrome
HMS is a musculoskeletal symptom related to the enlarged range of motion. Although it is not yet clear whether HMS correlates with the pain caused by the musical performance, HMS can increase the risk of musculoskeletal damage during specific exercise, and unnecessary pain can develop if HMS is misdiagnosed and treated inappropriately. Players often complain of idiopathic chronic unidentified wrist pain (CUWP) and HMS can be the main cause of CUWP.25) Brandfonbrener26) reported that HMS is more common in musicians (35% in women and 17% in men) compared to non-musicians. Therefore, when players complain of musculoskeletal symptoms without organic problems, HMS should be considered.
Compressive neuropathy
Compressive neuropathy is one of the musicians' hand and arm problems that often requires surgery. Carpal tunnel syndrome (CTS) is most common compression neuropathy in musicians. It can be detected by a provocative test such as Phalen test. In addition to clinical signs, patients complain of paresthesia and numbness at median nerve territory of the hand. However, to make a diagnosis of CTS in musicians, it must be differentiated from acute positional CTS.27) String players can present with symptoms of median nerve irritation at the wrist after playing. When the symptoms subside after rest, and clinical signs are negative this acute positional CTS can be suspected. NSAIDs and steroid injection should be considered first and surgery should be considered as a last resort.27)
Ulnar nerve neuropathy at the elbow (cubital tunnel syndrome) is the second most common compression syndrome after CTS. Risk factors for cubital tunnel syndrome in professional string musician are positions such as "hold in position" and "use elbows for support", in which case, flexed elbow increased pressure in the cubital tunnel.25) Ulnar nerve neuropathy is sometimes associated with focal dystonia. Charness et al.28) reported ulnar neuropathy was diagnosed in 28 of 73 (40%) cases of occupational cramp in musicians. Ross et al.29) also reported high prevalence of ulnar neuropathy in musicians with dystonic flexion of the little and ring fingers. Moreover, the EMG activity of musicians with ulnar neuropathy showed an abnormal pattern similar to that observed in the dystonic patients. If decompression surgery is necessary, the operation should be performed at an early stage for a rapid return to play.30)
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Roset-Llobet J, Rosines-Cubells D, Salo-Orfila JM. Identification of risk factors for musicians in Catalonia (Spain) Med Probl Perform Art. 2000;15(4):167–174. [Google Scholar]
- 2.Sung NJ, Sakong J, Chung JH. Musculoskeletal diorders and related factors of symphony orchestra players. Korean J Occup Environ Med. 2000;12(1):48–58. [Google Scholar]
- 3.Abreu-Ramos AM, Micheo WF. Lifetime prevalence of upper-body musculoskeletal problems in a professional-level symphony orchestra: age, gender, and instrument-specific results. Med Probl Perform Art. 2007;22(3):97–104. [Google Scholar]
- 4.Guptill C, Zaza C, Paul S. An occupational study of physical playing-related injuries in college music students. Med Probl Perform Art. 2000;15(2):86–90. [Google Scholar]
- 5.Koh J, Lee SJ, Kim YK, et al. The prevalence of playing-related musculoskeletal disorders of music college freshmen playing string instruments. Korean J Occup Environ Med. 2006;18(3):189–198. [Google Scholar]
- 6.Lockwood AH. Medical problems of musicians. N Engl J Med. 1989;320(4):221–227. doi: 10.1056/NEJM198901263200405. [DOI] [PubMed] [Google Scholar]
- 7.Almekinders LC. Tendinitis and other chronic tendinopathies. J Am Acad Orthop Surg. 1998;6(3):157–164. doi: 10.5435/00124635-199805000-00003. [DOI] [PubMed] [Google Scholar]
- 8.Yap EC. Myofascial pain: an overview. Ann Acad Med Singapore. 2007;36(1):43–48. [PubMed] [Google Scholar]
- 9.Potter PJ, Jones IC. Medical problems affecting musicians. Can Fam Physician. 1995;41:2121–2128. [PMC free article] [PubMed] [Google Scholar]
- 10.Fry HJ. The treatment of overuse syndrome in musicians: results in 175 patients. J R Soc Med. 1988;81(10):572–575. doi: 10.1177/014107688808101007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shafer-Crane GA. Repetitive stress and strain injuries: preventive exercises for the musician. Phys Med Rehabil Clin N Am. 2006;17(4):827–842. doi: 10.1016/j.pmr.2006.07.005. [DOI] [PubMed] [Google Scholar]
- 12.LeVine WR, Irvine JK. In vivo EMG biofeedback in violin and viola pedagogy. Biofeedback Self Regul. 1984;9(2):161–168. doi: 10.1007/BF00998831. [DOI] [PubMed] [Google Scholar]
- 13.de Greef M, van Wijck R, Reynders K, Toussaint J, Hesseling R. Impact of the Groningen exercise therapy for symphony orchestra musicians program on perceived physical competence and playing related musculoskeletal disorders of professional musicians. Med Probl Perform Art. 2003;18(4):156–160. [Google Scholar]
- 14.Winspur I. Advances in objective assessment of hand function and outcome assessment of the musician's hand. Hand Clin. 2003;19(3):483–493. doi: 10.1016/s0749-0712(03)00002-7. [DOI] [PubMed] [Google Scholar]
- 15.Winspur I, Parry CB. The musician's hand. J Hand Surg Br. 1997;22(4):433–440. [Google Scholar]
- 16.Dawson WJ. Upper-extremity problems caused by playing specific instruments. Med Probl Perform Art. 2002;17(3):135–140. [Google Scholar]
- 17.Fry HJ. Overuse syndrome in musicians: prevention and management. Lancet. 1986;2(8509):728–731. doi: 10.1016/s0140-6736(86)90242-4. [DOI] [PubMed] [Google Scholar]
- 18.Semple JC. Tenosynovitis, repetitive strain injury, cumulative trauma disorder, and overuse syndrome, et cetera. J Bone Joint Surg Br. 1991;73(4):536–538. doi: 10.1302/0301-620X.73B4.1820758. [DOI] [PubMed] [Google Scholar]
- 19.Kurppa K, Waris P, Rokkanen P. Peritendinitis and tenosynovitis: a review. Scand J Work Environ Health. 1979;5(suppl 3):19–24. doi: 10.5271/sjweh.2690. [DOI] [PubMed] [Google Scholar]
- 20.Parry CB. Managing the physical demands of musical performance. In: Williamon A, editor. Musical excellence: strategies and techniques to enhance performance. New York: Oxford University Press; 2004. pp. 41–60. [Google Scholar]
- 21.Lim VK, Altenmuller E, Bradshaw JL. Focal dystonia: current theories. Hum Mov Sci. 2001;20(6):875–914. doi: 10.1016/s0167-9457(01)00076-8. [DOI] [PubMed] [Google Scholar]
- 22.Altenmüller E. Focal dystonia: advances in brain imaging and understanding of fine motor control in musicians. Hand Clin. 2003;19(3):523–538. doi: 10.1016/s0749-0712(03)00043-x. [DOI] [PubMed] [Google Scholar]
- 23.Schuele S, Lederman RJ. Long-term outcome of focal dystonia in string instrumentalists. Mov Disord. 2004;19(1):43–48. doi: 10.1002/mds.10647. [DOI] [PubMed] [Google Scholar]
- 24.Jabusch HC, Altenmuller E. Focal dystonia in musicians: from phenomenology to therapy. Adv Cogn Psychol. 2006;2(2-3):207–220. [Google Scholar]
- 25.Quarrier NF. Is hypermobility syndrome (HMS) a contributing factor for chronic unspecific wrist pain in a musician? If so, how is it evaluated and managed? Work. 2011;40(3):325–333. doi: 10.3233/WOR-2011-1239. [DOI] [PubMed] [Google Scholar]
- 26.Brandfonbrener AG. Joint laxity and arm pain in a large clinical sample of musicians. Med Probl Perform Art. 2002;17(3):113–115. [Google Scholar]
- 27.Winspur I, Parry CB. The musician's hand: a clinical guide. London: Martin Dunitz; 1998. pp. 89–93. [Google Scholar]
- 28.Charness ME, Ross MH, Shefner JM. Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle Nerve. 1996;19(4):431–437. doi: 10.1002/mus.880190403. [DOI] [PubMed] [Google Scholar]
- 29.Ross MH, Charness ME, Lee D, Logigian EL. Does ulnar neuropathy predispose to focal dystonia? Muscle Nerve. 1995;18(6):606–611. doi: 10.1002/mus.880180607. [DOI] [PubMed] [Google Scholar]
- 30.Blum J. The musician's hand: aspects of music physiology and performing arts medicine. Handchir Mikrochir Plast Chir. 2000;32(5):299–310. doi: 10.1055/s-2000-10940. [DOI] [PubMed] [Google Scholar]