

Abstract
Background
Fractures which need urgent or emergency treatment are common in children and adolescents. This study investigated the incidence patterns of pediatric and adolescent orthopaedic fractures according to age groups and seasons in South Korea based on population data.
Methods
Data on the number of pediatric and adolescent patients under the age of 18 years who utilized medical services due to fractures were retrieved from the Health Insurance Review and Assessment service in South Korea. The data included four upper extremity and two lower extremity fractures according to four age groups (0-4 years, 5-9 years, 10-14 years, and 15-18 years). Incidences of the fractures were calculated as the incidence per 10,000 per year, and patterns according to age groups and seasons were demonstrated.
Results
The annual incidence of clavicle, distal humerus, both forearm bone, distal radius, femoral shaft and tibial shaft fractures were 27.5, 34.6, 7.7, 80.1, 2.5, and 9.6 per 10,000 per year in children and adolescents, respectively. Clavicle and distal radius fractures showed significant seasonal variation for all age groups but femoral shaft fracture showed no significant seasonal variation for any of the age groups.
Conclusions
The four upper extremity fractures tended to show greater variations than the two lower extremity fractures in the nationwide database in South Korea. The study results are believed to be helpful in the planning and assignment of medical resources for fracture management in children and adolescents.
Keywords: Incidence, Seasonal variation, Pediatric and adolescent, Fracture
Fractures are common orthopaedic problems in children and adolescents, which require urgent or emergency management in most cases. These unpredictable emergencies can place a significant burden on medical resources, and often results in the excessive workload of medical personnel and a shortage of hospital rooms for admission. This may be a systematic factor in the delivery of inappropriate medical care.
Previous studies have reported the incidence of specific fractures differs according to age, season, weather, and day of the week, etc.1-17) These studies provide information on the risk factors for fractures, and possible preventive measures for fractures. On the other hand, most studies have been confined to specific fractures, specific age groups and specific hospitals,1,2,4,7,9,11,13-18) and there is insufficient population-based data given by these studies, particularly data covering the nationwide population.
This study examined the incidence of several pediatric and adolescent orthopaedic fractures including clavicle, distal humerus, both forearm bone, distal radius, femoral shaft, and tibial shaft fractures based on nationwide population data, as well as the incidence patterns according to seasonal variations and age groups.
METHODS
The institutional review board at our hospital waived approval for this study because it did not involve human subjects as materials.
Study Population
The data of this study originated from the nationwide population of South Korea, which has a total population of 48,219,000 as of 2009. Approximately 10 million children and adolescents aged 18 years and under who were enrolled in the national health insurance system comprised the study population.
Data Collection
Data on the number of pediatric and adolescent patients who utilized medical services due to fractures were retrieved from the Health Insurance Review and Assessment (HIRA) service. This institute reviews the suitability of payments from the national health insurance scheme to medical institutes, and also mediates in disputes between producers and consumers of medical services, assesses the adequacy of medical practice, and assists in the development of government health policy in South Korea.
The data obtained from the HIRA contained the monthly number of pediatric and adolescent patients between 2005 and 2009 according to four age groups (0-4 years, 5-9 years, 10-14 years, and 15-18 years) with diagnostic codes of S42.0, S42.4, S52.4, S52.5, S72.3, and S82.2 (in International Classification of Diseases 10), which represent clavicle fractures, fractures of the distal humerus, both forearm bone fractures, distal radius fractures, femoral shaft fractures and tibial shaft fractures.
Incidences of Fractures and Seasonal Variation
The annual incidence of each fracture was calculated by dividing the total number of children and adolescents that were enrolled in the national insurance system by the total annual number of children and adolescent patients with the fracture. The incidences were represented as the incidence per 10,000 per year with 95% confidence intervals (CI). The seasonal incidences were also presented per 10,000 per year. Incidence variation was calculated by dividing the highest incidence by the lowest incidence.
Statistical Methods
No specific statistical analysis was used other than descriptive statistical analysis because this study included the whole population. The distribution of fracture onset within the four seasons was tested for homogeneity in the total fracture population for each fracture type, using the chisquare test for goodness of fit with Bonferroni's correction.
RESULTS
The annual incidence of clavicle fractures, distal humerus fractures, both forearm bone fractures, distal radius fractures, femoral shaft fractures and tibial shaft fractures were 27.5 (95% CI, 27.2 to 27.8), 34.6 (95% CI, 34.2 to 34.9), 7.7 (95% CI, 7.5 to 7.9), 80.1 (95% CI, 79.6 to 80.6), 2.5 (95% CI, 2.4 to 2.6), 9.6 (95% CI, 9.4 to 9.7) per 10,000 per year in 2009, respectively. Both forearm bone and tibial shaft fractures showed a slightly decreasing trend and femoral shaft fractures showed a slightly increasing trend between 2005 and 2009 (Fig. 1).
Fig. 1.

Annual incidences of pediatric and adolescent orthopaedic fractures between 2005 and 2009. The incidence of distal radius fracture was the highest, followed by distal humerus, clavicle, tibial shaft, both forearm bone, and femoral shaft fractures. Both forearm bone and tibial shaft fractures showed a slightly decreasing trend and femoral shaft fractures showed a slightly increasing trend between 2005 and 2009.
In 2009, clavicle fractures showed a peak incidence of 46.0 (95% CI, 45.1 to 46.9) in age group 0-4 years and a decreasing incidence with age. Distal humerus fractures showed peak incidence of 71.0 (95% CI, 70.0 to 72.0) in the 5-9 year age group, followed by the 0-4 year age group. The peak incidence of both forearm bone fractures was 11.1 (95% CI, 10.8 to 11.5) in the 10-14 year age group, showing a similar incidence of 10.7 (95% CI, 10.3 to 11.1) in the 5-9 year age group. Distal radius fractures showed the greatest variation according to the age group: 148.1 (95% CI, 146.8 to 149.4) in the 10-14 year age group and 19.0 (95% CI, 18.5 to 19.6) in the 0-4 year age group. Femoral shaft fractures showed the least variation according to age groups; the incidence was 1.9 (95% CI, 1.8 to 2.1) in the 10-14 year age group and 3.6 (95% CI, 3.3 to 3.8) in the 15-18 year age group. Tibial shaft fractures showed a decreasing incidence with increasing age; incidence was 13.5 (95% CI, 13.0 to 14.0) in the 0-4 year age group and 5.7 (95% CI, 5.5 to 6.0) in the 15-18 year age group (Fig. 2).
Fig. 2.

This figure depicts the annual incidence of each fracture according to age groups in 2009. Distal radius fractures showed the greatest variation according to age groups, while femoral shaft fractures showed the least variation.
In terms of seasonal variations in 2009, clavicle fractures, distal humerus fractures, both forearm bone fractures, and distal radius fractures showed the highest incidence in summer, followed in order by autumn, spring and winter. Femoral shaft fractures and tibial shaft fractures showed a peak incidence in winter. Distal humerus fractures showed the highest seasonal variation with the highest and lowest incidence in summer (44.5) and winter (24.9), respectively, whereas femoral shaft fractures showed the lowest seasonal variations with the highest and lowest incidence in winter (2.8) and spring and autumn (2.3), respectively (Fig. 3).
Fig. 3.

Seasonal variation of pediatric and adolescent fracture incidences in 2009. The four upper extremity fractures showed the highest incidence in summer, while the two lower extremity fractures showed the highest incidence in winter. Distal humerus fractures showed the highest seasonal variations and femoral shaft fractures showed the lowest seasonal variations.
Seasonal variation of each fracture was significant. However, in the subgroup analysis, none of the age subgroups showed significant seasonal variation in femoral shaft fracture. Clavicle and distal radius fractures showed significant seasonal variation for all age subgroups (Table 1).
Table 1.
Seasonal Variation of Each Fracture. Conventional χ2 Statistics
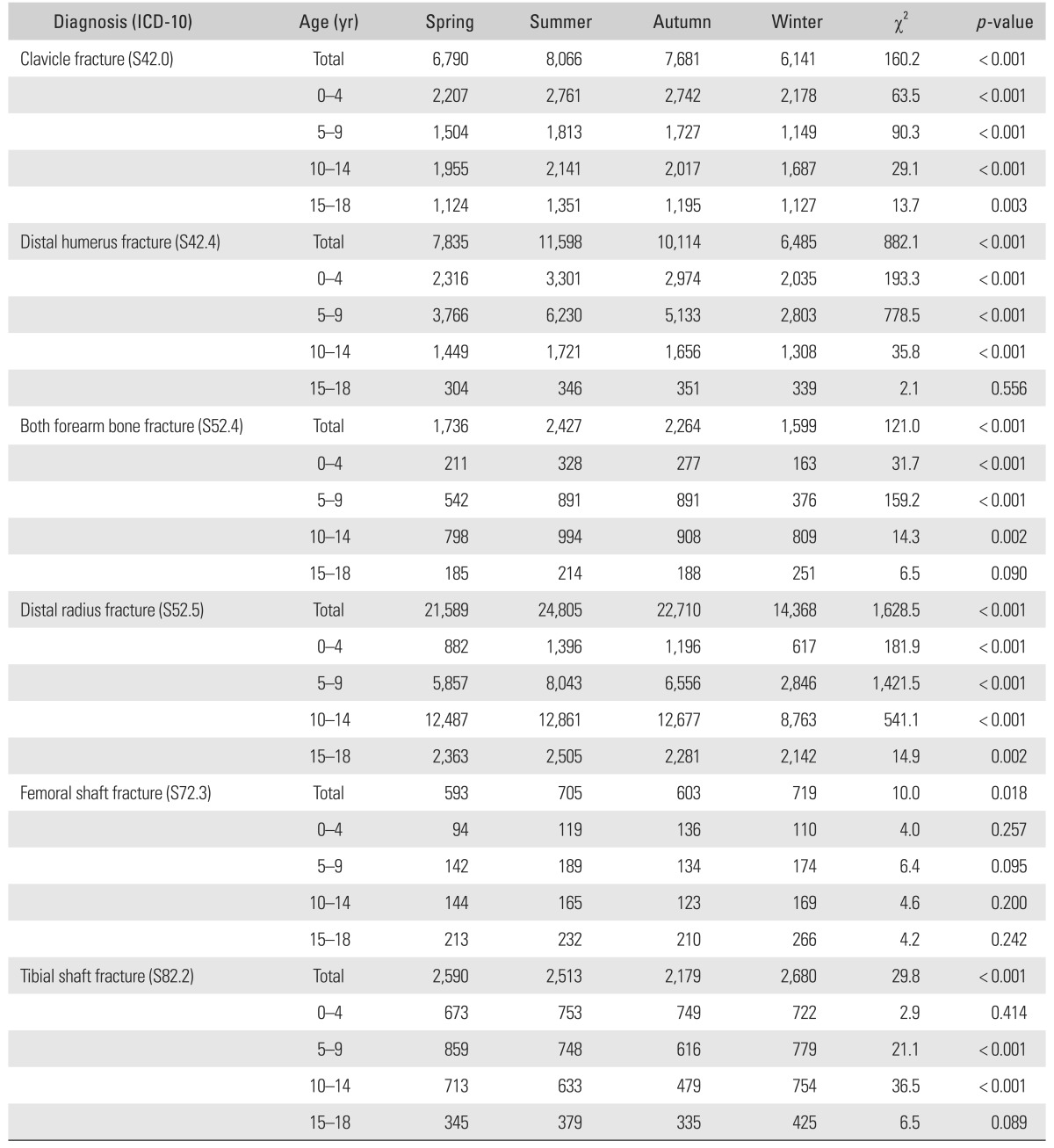
Seasonal variation was calculated by dividing the highest incidence by the lowest incidence.
ICD: International Classification of Diseases.
DISCUSSION
Tibial shaft fractures showed a slightly decreasing annual incidence, whereas femoral shaft fractures showed an increasing incidence during the recent five years between 2005 and 2009. Clavicle fractures, distal humerus fractures, both forearm bone fractures and distal radius fractures did not demonstrate any notable increasing or decreasing tendency. Distal humerus fractures showed the greatest age and seasonal variations, and femoral shaft fractures showed the smallest age and seasonal variations. After stratifying the fracture incidence according to age group, distal radius fractures in the 5-9 year age group showed the highest seasonal variation, and tibial shaft fractures in the 0-4 year age group showed the lowest seasonal variation in 2009.
Before discussing the study results, some limitations need to be addressed. First, the age groups were based on administrative factors rather than clinical considerations. If the age groups had been made on a clinical basis, the study results could have had more useful implications in terms of the treatment choice (conservative or surgical) and prognosis. Second, the data of this study was retrieved on a diagnosis basis and not on a subject basis. Therefore, concurrent injuries or other causative factors could not be evaluated. Subject based data is expected to provide more valuable clinical information in a future study.
The variation in the fracture incidence according to age groups is an important issue. This has clinical significance in that the fracture incidence can be affected by developmental factors. The considerable variations in fracture incidence in this study, particularly for distal humerus fractures and distal radius fractures, suggest that the development of anatomical structures or certain types of activity and behavior can be causative factors in terms of the fracture mechanism, fracture sites and fracture pattern.
Many studies have examined the seasonal variation of specific fractures.1-4,6,19) Previous studies have suggested different causes for the seasonal variations in fracture incidence, and these include change in outdoor activity due to weather, change in vitamin D metabolism due to a change in the length of daytime, increase in the slippery load in winter, visual acuity changes in winter due to early sunset, etc.5,9,11,20-28) For the six pediatric and adolescent orthopaedic fractures examined in this study, the highest incidence was observed in summer except for femoral shaft fractures and tibial shaft fractures. Femoral shaft and tibial shaft fractures showed the highest incidence in winter but lower seasonal variation. Therefore, the higher incidence of the four upper extremity fractures in children and adolescents in summer can probably be explained by children and adolescents engaging in outdoor sports activity more often, and sustaining low-energy traumatic injuries that cause the fractures. On the other hand, the higher incidence of the two lower extremity fractures in winter can partly be explained by seasonal factors, such as the higher slippery load, decreased visual acuity and decreased vitamin D metabolism in winter. A considerable portion of femoral shaft fractures and tibial shaft fractures are believed to be caused by high-energy trauma, such as traffic accidents, which are less affected by seasonal factors, but this issue requires further investigation.
A previous study reported a comprehensive survey of the fracture incidence of children in the 0 to 15 years age group.29) Although the age of the study population was slightly different from that of the present study, the incidence of both forearm bone fractures, distal radius fractures and femoral shaft fractures shown in that study was comparable to that obtained in the present study. On the other hand, the incidence of clavicle fractures, distal humerus fractures, and tibial shaft fractures in the present study was much higher than that of the previous study, showing a 2.7 to 3.9 fold increase in incidence. It is believed that ethnic or cultural factors can also play a role in fracture incidence, which is a factor researchers and clinicians should consider.
In conclusion, the four upper extremity fractures tended to show greater variations than the two lower extremity fractures in children and adolescents in a nationwide database of South Korea. The study results are believed to be helpful in the planning and assigning of medical resources for fracture management in children and adolescents.
ACKNOWLEDGEMENTS
The authors wish to thank Mi Sun Ryu, BS, for data collection. This work was supported by the Ministry of Trade, Industry & Energy (grant number, 10045220).
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Valerio G, Galle F, Mancusi C, et al. Pattern of fractures across pediatric age groups: analysis of individual and lifestyle factors. BMC Public Health. 2010;10:656. doi: 10.1186/1471-2458-10-656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wareham K, Johansen A, Stone MD, Saunders J, Jones S, Lyons RA. Seasonal variation in the incidence of wrist and forearm fractures, and its consequences. Injury. 2003;34(3):219–222. doi: 10.1016/s0020-1383(02)00212-7. [DOI] [PubMed] [Google Scholar]
- 3.Atherton WG, Harper WM, Abrams KR. A year's trauma admissions and the effect of the weather. Injury. 2005;36(1):40–46. doi: 10.1016/j.injury.2003.10.027. [DOI] [PubMed] [Google Scholar]
- 4.Ferreira PC, Amarante JM, Silva AC, Pereira JM, Cardoso MA, Rodrigues JM. Etiology and patterns of pediatric mandibular fractures in Portugal: a retrospective study of 10 years. J Craniofac Surg. 2004;15(3):384–391. doi: 10.1097/00001665-200405000-00008. [DOI] [PubMed] [Google Scholar]
- 5.Brudvik C, Hove LM. Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop. 2003;23(5):629–634. doi: 10.1097/00004694-200309000-00010. [DOI] [PubMed] [Google Scholar]
- 6.Lyons RA, Delahunty AM, Kraus D, et al. Children's fractures: a population based study. Inj Prev. 1999;5(2):129–132. doi: 10.1136/ip.5.2.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hove LM, Brudvik C. Displaced paediatric fractures of the distal radius. Arch Orthop Trauma Surg. 2008;128(1):55–60. doi: 10.1007/s00402-007-0473-x. [DOI] [PubMed] [Google Scholar]
- 8.Rennie L, Court-Brown CM, Mok JY, Beattie TF. The epidemiology of fractures in children. Injury. 2007;38(8):913–922. doi: 10.1016/j.injury.2007.01.036. [DOI] [PubMed] [Google Scholar]
- 9.Kramhoft M, Bodtker S. Epidemiology of distal forearm fractures in Danish children. Acta Orthop Scand. 1988;59(5):557–559. doi: 10.3109/17453678809148784. [DOI] [PubMed] [Google Scholar]
- 10.Landin LA. Fracture patterns in children: analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950-1979. Acta Orthop Scand Suppl. 1983;202:1–109. [PubMed] [Google Scholar]
- 11.Thomas EM, Tuson KW, Browne PS. Fractures of the radius and ulna in children. Injury. 1975;7(2):120–124. doi: 10.1016/0020-1383(75)90009-1. [DOI] [PubMed] [Google Scholar]
- 12.Bulajic-Kopjar M. Seasonal variations in incidence of fractures among elderly people. Inj Prev. 2000;6(1):16–19. doi: 10.1136/ip.6.1.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Crawford JR, Parker MJ. Seasonal variation of proximal femoral fractures in the United Kingdom. Injury. 2003;34(3):223–225. doi: 10.1016/s0020-1383(02)00211-5. [DOI] [PubMed] [Google Scholar]
- 14.Thompson PW, Taylor J, Dawson A. The annual incidence and seasonal variation of fractures of the distal radius in men and women over 25 years in Dorset, UK. Injury. 2004;35(5):462–466. doi: 10.1016/S0020-1383(03)00117-7. [DOI] [PubMed] [Google Scholar]
- 15.Douglas S, Bunyan A, Chiu KH, Twaddle B, Maffulli N. Seasonal variation of hip fracture at three latitudes. Injury. 2000;31(1):11–19. doi: 10.1016/s0020-1383(99)00192-8. [DOI] [PubMed] [Google Scholar]
- 16.Chiu KY, Ng TP, Chow SP. Seasonal variation of fractures of the hip in elderly persons. Injury. 1996;27(5):333–336. doi: 10.1016/0020-1383(95)00232-4. [DOI] [PubMed] [Google Scholar]
- 17.Jacobsen SJ, Goldberg J, Miles TP, Brody JA, Stiers W, Rimm AA. Seasonal variation in the incidence of hip fracture among white persons aged 65 years and older in the United States, 1984-1987. Am J Epidemiol. 1991;133(10):996–1004. doi: 10.1093/oxfordjournals.aje.a115819. [DOI] [PubMed] [Google Scholar]
- 18.Ogundare BO, Bonnick A, Bayley N. Pattern of mandibular fractures in an urban major trauma center. J Oral Maxillofac Surg. 2003;61(6):713–718. doi: 10.1053/joms.2003.50118. [DOI] [PubMed] [Google Scholar]
- 19.Bischoff-Ferrari HA, Orav JE, Barrett JA, Baron JA. Effect of seasonality and weather on fracture risk in individuals 65 years and older. Osteoporos Int. 2007;18(9):1225–1233. doi: 10.1007/s00198-007-0364-6. [DOI] [PubMed] [Google Scholar]
- 20.Rális ZA. Epidemic of fractures during period of snow and ice. Br Med J (Clin Res Ed) 1981;282(6264):603–605. [PMC free article] [PubMed] [Google Scholar]
- 21.Ralis ZA, Barker EA, Leslie IJ, Morgan WJ, Ross AC, White SH. Snow-and-ice fracture in the UK, a preventable epidemic. Lancet. 1988;1(8585):589–590. doi: 10.1016/s0140-6736(88)91383-9. [DOI] [PubMed] [Google Scholar]
- 22.Jacobsen SJ, Sargent DJ, Atkinson EJ, O'Fallon WM, Melton LJ., 3rd Contribution of weather to the seasonality of distal forearm fractures: a population-based study in Rochester, Minnesota. Osteoporos Int. 1999;9(3):254–259. doi: 10.1007/s001980050145. [DOI] [PubMed] [Google Scholar]
- 23.Jacobsen SJ, Sargent DJ, Atkinson EJ, O'Fallon WM, Melton LJ., 3rd Population-based study of the contribution of weather to hip fracture seasonality. Am J Epidemiol. 1995;141(1):79–83. doi: 10.1093/oxfordjournals.aje.a117348. [DOI] [PubMed] [Google Scholar]
- 24.Ivers RQ, Cumming RG, Mitchell P, Attebo K. Visual impairment and falls in older adults: the Blue Mountains Eye Study. J Am Geriatr Soc. 1998;46(1):58–64. doi: 10.1111/j.1532-5415.1998.tb01014.x. [DOI] [PubMed] [Google Scholar]
- 25.Schott GD, Wills MR. Muscle weakness in osteomalacia. Lancet. 1976;1(7960):626–629. doi: 10.1016/s0140-6736(76)90428-1. [DOI] [PubMed] [Google Scholar]
- 26.Landin LA, Danielsson LG. Children's ankle fractures: classification and epidemiology. Acta Orthop Scand. 1983;54(4):634–640. doi: 10.3109/17453678308992902. [DOI] [PubMed] [Google Scholar]
- 27.Pramyothin P, Techasurungkul S, Lin J, et al. Vitamin D status and falls, frailty, and fractures among postmenopausal Japanese women living in Hawaii. Osteoporos Int. 2009;20(11):1955–1962. doi: 10.1007/s00198-009-0910-5. [DOI] [PubMed] [Google Scholar]
- 28.Hill TR, McCarthy D, Jakobsen J, Lamberg-Allardt C, Kiely M, Cashman KD. Seasonal changes in vitamin D status and bone turnover in healthy Irish postmenopausal women. Int J Vitam Nutr Res. 2007;77(5):320–325. doi: 10.1024/0300-9831.77.5.320. [DOI] [PubMed] [Google Scholar]
- 29.Mayranpaa MK, Makitie O, Kallio PE. Decreasing incidence and changing pattern of childhood fractures: a population-based study. J Bone Miner Res. 2010;25(12):2752–2759. doi: 10.1002/jbmr.155. [DOI] [PubMed] [Google Scholar]