

Abstract
Background:
Anthropometric and socioeconomic factors are known to influence peak expiratory flow rate, but the effect of altitude has not been established decisively, due to conflicting results of various studies.
Aim:
This study was conducted to evaluate the effect of altitude on peak expiratory flow rate of healthy school children.
Materials and Methods:
A cross-sectional study was conducted in which the peak expiratory flow rate of a group of 290 school children (140 male and 150 female), aged 7-14 years, residing in Shimla (altitude 2150 meters), were compared with the results obtained in an age- and sex-matched control group, consisting of 280 school children (138 male and 142 female), residing in Patiala (altitude 278 meters). Mini Wright Peak Flow Meter was used for the study.
Results:
The mean peak expiratory flow rate value of boys at high altitude (265 ± 92.6 L/min) was significantly higher than those in plain areas (245 ± 82.1 L/min). Similarly, the mean peak expiratory flow rate of highlander girls (250.4 ± 70.2 L/min) was significantly higher than girls of plains (232.6 ± 65 L/min).
Conclusion:
The study suggests that besides anthropometric and socioeconomic factors, altitude is an important determinant of lung function.
Keywords: Altitude, Lung function, Peak expiratory flow rate, School children
Introduction
The peak expiratory flow rate (PEFR) is an effort-dependent parameter, emerging from the large airways within about 100-120 msec of the start of forced expiration. It remains at its peak for 10 msec.[1] It is well documented in literature that a wide range of geographical, climatic, anthropometric, nutritional, and socioeconomic conditions of India are associated with regional differences in lung function.[2]
Millions of people in the world live permanently at high altitude and are thus exposed to a mosaic of harsh environmental conditions such as hypoxia, cold, high solar radiation, and rugged terrain. This leads to striking differences between high- and low-altitude human populations with respect to various biological traits, including anthropometric and respiratory differences.[3] At high altitudes, a number of acute and chronic airway mechanisms are activated, which are aimed at optimizing oxygen availability.[4]
Many studies have clearly demonstrated the effect of gender and various anthropometric parameters like age, height, and weight on lung function in normal children.[5,6,7,8] However, there is a dearth of studies which have attempted to investigate the effect of altitude on lung function. Although a few studies have attempted to compare the PEFR values of highlander and lowlander populations, the effect of altitude on lung function has still not been decisively established, due to the conflicting results reported by these studies.
The aim of the present study was to compare the PEFR values of healthy school children, from these two contrasting geographical locations, and investigate the effect of altitude on the lung functions of humans.
Materials and Methods
The study was conducted during March-August 2010 on 570 school children, aged 7-14 years, studying in various high schools in Shimla (altitude 2150 meters) and Patiala (altitude 278 meters), during their school hours. The study was approved by the ethical committee of the institute and was as per the Helsinki declaration. Prior permission of the school authorities was taken and written consent from the parents/guardians of all children was also obtained after clearly explaining them the purpose of the study.
A detailed history, followed by a thorough clinical examination was done as per the latest guidelines laid down by the American Thoracic Society.[9] For the study, all available healthy children were included, except those with wheezing, visible bony, and muscular deformities of the chest wall, history of cardiac and respiratory disease, history of medications like anti-asthmatics, history of recurrent hospital admission or respiratory infection within three weeks prior to the study, family history of asthma, etc.
For all subjects, age was calculated to the nearest completed year. Weight (in kg) was measured without shoes and with light clothing, on a standard calibrated bathroom scale. Height (in cm) was measured with a standard portable stadiometer.
PEFR values were then recorded in standing position, using the Mini Wright Peak Flow meter (Clement Clarke International Limited, U.K.). The maneuver was explained and demonstrated to them before the actual recording. Each child was asked to take a deep breath and then blow into the peak flow meter as hard and quickly as possible. The marker was returned to zero after every measurement. Every child was given two trial runs and encouraged to blow harder each time. Three measurements were taken and the highest reading was recorded. A tight seal was maintained between the lips and the mouthpiece. The mouthpiece was washed and sterilized for each subject.[10]
The measured values of PEFR of all children were standardized to Body Temperature and ambient Pressure Saturated (BTPS), before analyzing them statistically, by applying the following correction equation for PEFR, suggested by Pederson et al.[11]
![]()
where,
PEFm is the measured PEFR value.
PEFc is the corrected PEFR value.
D is density of air.
A0, K1, and K2 are constants, whose values are 0.25 cm2, 1.42 kPa/cm2, and 435 L/min/cm2, respectively.
Furthermore, the density of air (D) was calculated from another equation suggested by Pederson et al.:
![]()
where,
Constant 1.293 is the density of air in kg/m3 (at a temperature of 273 Kelvin and a pressure of 101.3 kPa)
B is the ambient pressure (kPa; measured with a portable aneroid barometer)
T is the ambient temperature (measured in Kelvin with a portable, wall-mountable, alcohol-based room thermometer).
Statistical analysis
The data comprised PEFR values, which were processed for mean and standard deviation. Age, height, and weight were the independent variables, while PEFR value was the dependent variable. Student's unpaired T-test was used to compare the PEFR values between various groups. P < 0.05 were considered statistically significant, while P < 0.001 were considered statistically highly significant. Regression equations based on age, height, and weight were constructed for both highlander and lowlander boys and girls. Correlation between age, height, weight, and PEFR was done using Pearson's correlation. The statistical analysis was carried out with SPSS version 13.0 (Chicago IL, USA).
Results
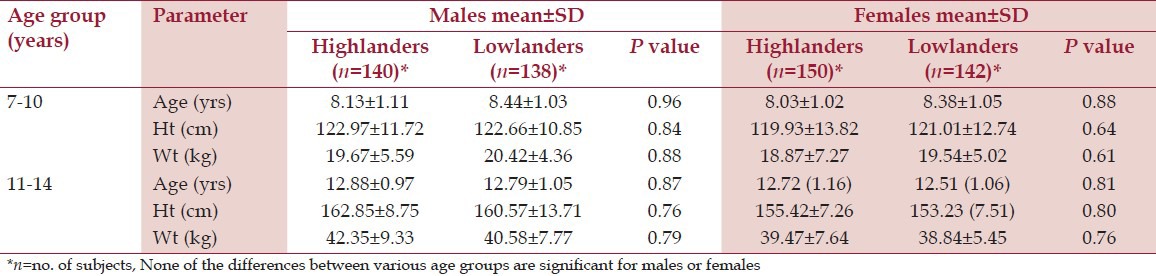
Both highlander and lowlander children were divided age-wise into two groups (i.e., 7-10 years and 11-14 years). Table 1 shows the comparison of mean ± SD of age, height, and weight of highlander and lowlander children of both sexes, for both age groups. It is clear from this table that there is no statistically significant difference in the values of above parameters between highlanders and lowlanders, of both sexes, in any of the two age groups, indicating that both the groups are comparable.
Table 1.
Comparison of mean±SD of age and anthropometric parameters of male and female children of various age groups
Furthermore, a highly significant positive correlation of PEFR was observed with age, height, and weight in both male and female highlander and lowlander children [Table 2], indicating that an increase in any of these three parameters results in a subsequent rise in PEFR values as well. In both highlander and lowlander males and females, PEFR showed the highest correlation with height.
Table 2.
Coefficient of correlation (r) between PEFR and age, height, and weight in male and female children

Gender-wise comparison of mean PEFR values was also done separately for highlanders and lowlanders, as shown in Table 3. For both highlanders and lowlanders, males had higher PEFR values than females, the difference being significant in 7-10 years age group, and highly significant in 11-14 years age group.
Table 3.
Comparison of mean±SD values of PEFR between males and females of highlands and lowlands

An overall comparison of mean PEFR values between 7- to 14-year-old highlander and lowlander children [Table 4] showed that the difference between mean PEFR of highlander males and lowlander males and the difference between mean PEFR of highlander females and lowlander females were both statistically highly significant.
Table 4.
Comparison of PEFR between highlander and lowlander children, aged 7.14 years, for both genders, as per their mean±SD value

Further, on doing a similar, but age group-wise comparison of mean PEFR values [Table 5], it was seen that in the 7-10 year age group, the difference between mean PEFR of highlander males and lowlander males was statistically significant, while a similar difference in the 11-14 years age group, i.e., between highlander males and lowlander males, was highly significant statistically. Also, while the difference between mean PEFR values of 7- to 10-year-old highlander females and lowlander females was significant, the difference in mean PEFR values of 11- to 14-year-old highlander females and lowlander females was highly significant statistically. Therefore, Tables 4 and 5 clearly show that high-altitude residents have better values of lung function.
Table 5.
Age group-wise comparison of mean±SD values of PEFR between highlanders and lowlander

The regression equations for all categories of children are as follows:
-
High-altitude boys
PEFR (L/min) = −201.25 + 9.25 × Age (yrs) + 2.26 × Ht (cm) + 1.32 × Wt (kg)
R2 = 0.965, SEE = ± 18.016
-
Plain area boys
PEFR (L/min) = −150.38 + 9.19 × Age (yrs) + 1.75 × Ht (cm) + 1.74 × Wt (kg).
R2 = 0.969, SEE = ± 14.435
-
High-altitude girls
PEFR (L/min) = −222.61 + 9.42 × Age (yrs) + 2.57 × Ht (cm) + 0.11 × Wt (kg).
R2 = 0.946, SEE = ± 18.264
-
Plain area girls
PEFR (L/min) = −177.06 + 0.86 × Age (yrs) + 2.59 × Ht (cm) + 1.49 × Wt (kg).
R2 = 0.949, SEE = ± 15.661
Discussion
The present study aimed at establishing the effect of altitude on PEFR by comparing PEFR values of healthy highlander and lowlander school children. In our study, significantly higher PEFR values were observed in high-altitude native children as compared to their lowlander counterparts. Many other authors throughout the world have also reported results similar to those of the present study.[12,13,14,15]
Qazi et al.[16] reported that altitude greater than 1500 meters appears to cause measurable changes in lung volumes and flow rates; this is because the accessory muscles of respiration are far more developed in higher-altitude residents due to hypoxia. Also, the higher anthropometric ratios, e.g. chest to leg ratio (which denotes a high vertical chest size) and better lung growth due to increased physical activity, lesser population density, and low levels of environmental pollution in high-altitude areas may explain increased values of lung volumes and flow rates in residents of these areas. However, Weitz et al.[17] suggested that greater lung function at higher altitude primarily results from development of a hypoxic environment and is less likely to be caused by increased activity or lower pollution. Dr. West[18] suggested that since the air at higher altitude is less dense, airway resistance is reduced, and maximum inspiratory and expiratory flows are greater than that at sea level.
In contrast to the present study, some authors have reported no significant difference in the PEFR values of highlanders and lowlanders.
Debray et al.[19] measured the PEFR values of Nepalese young adults and compared them with their Indian counterparts. No significant difference was found either between the mean ± SD PEFR of Nepalese males (485.9 ± 49.85 L/min) and Indian males (490.4 ± 49.85 L/min) or between the mean ± SD PEFR of Nepalese females (365.2 ± 55.83 L/min) and Indian females (386 ± 48.31 L/min); this concluded that prediction equations made for Indian adults could also be used to predict PEFR of Nepalese adults.
Kashyap et al.[20] compared the PEFR values of healthy highlander tribal children with lowlander North Indian urban children, and found that mean PEFR in highlander boys (245.5 ± 74 L/min) was comparable with that in lowlander boys (248 ± 64 L/min).
Study limitations
The limitation of this study was that mini Wright's peak flow meter was used to measure PEFR values, due to its lower accuracy as compared to a computerized spirometer. However, our study method was performed strictly as per standardized guidelines, using a widely available portable instrument, thereby ensuring as much accuracy as possible.
Future directions
Clinical research should continue to assess the changes in other lung function parameters as well as in high-altitude natives (e.g., forced vital capacity, forced expiratory volume, maximum ventilatory volume). This will be of immense help in decisively establishing the influence of altitude on respiratory functions.
Conclusion
The findings of this study show a significant rise in PEFR among high-altitude residents. The increase in PEFR with altitude may be attributed to lower air density at altitude or may even be the result of better lung growth in highlanders, due to natural adaptive changes in their body, in response to hypoxia. Thus, altitude, like other factors (e.g., age, height, weight, and gender), is also an important determinant of lung function.
Acknowledgment
We thank all children participating in this study, without whose active cooperation, this study would have not been possible. We also extend our warm gratitude to the all parents and school authorities for their much needed help and support.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Dikshit MB, Raje S, Agrawal MJ. Lung functions with spirometry: An Indian perspective-I. Peak expiratory flow rates. Indian J Physiol Pharmacol. 2005;49:8–18. [PubMed] [Google Scholar]
- 2.Raju PS, Prasad KV, Ramana YV, Murthy KJ. Pulmonary function tests in Indian girls- prediction equations. Indian J Pediatr. 2004;71:893–7. doi: 10.1007/BF02830828. [DOI] [PubMed] [Google Scholar]
- 3.Kapoor S, Kapoor AK. Body structure and respiratory efficiency among high altitude Himalayan populations. Coll Antropol. 2005;29:37–43. [PubMed] [Google Scholar]
- 4.Cingi C, Selcuk A, Oghan F, Firat Y, Guvey A. The physiological impact of high altitude on nasal and lower airway parameters. Eur Arch Otorhinolaryngol. 2011;268:841–4. doi: 10.1007/s00405-010-1468-8. [DOI] [PubMed] [Google Scholar]
- 5.Doctor TH, Trivedi SS, Chudasama RK. Pulmonary function test in healthy school children of 8 to 14 years age in south Gujarat region, India. Lung India. 2010;27:145–8. doi: 10.4103/0970-2113.68317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Taksande A, Jain M, Vilhekar K, Chaturvedi P. Peak expiratory flow rate of rural school children from Wardha district, Maharashtra in India. World J Pediatr. 2008;4:211–4. doi: 10.1007/s12519-008-0039-1. [DOI] [PubMed] [Google Scholar]
- 7.Vijayan VK, Reetha AM, Kuppurao KV, Venkatesan P, Thilakavathy S. Pulmonary function in normal south Indian children aged 7 to 19 years. Indian J Chest Dis Allied Sci. 2000;42:147–56. [PubMed] [Google Scholar]
- 8.Gundogdu Z, Eryilmaz N. Correlation between peak flow and body mass index in obese and non-obese children in Kocaeli, Turkey. Prim Care Respir J. 2011;20:403–6. doi: 10.4104/pcrj.2011.00061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 10.Agaba PA, Thacher TD, Angyo IA, Agaba EI. Peak expiratory flow rates in healthy Nigerian children. J Trop Pediatr. 2003;49:157–9. doi: 10.1093/tropej/49.3.157. [DOI] [PubMed] [Google Scholar]
- 11.Pederson OF, Miller MR, Sigsgaard T, Tidley M, Harding RM. Portable peak flow meteres: Physical characteristics, influence of temperature, altitude and humidity. Eur Respir J. 1994;7:991–7. [PubMed] [Google Scholar]
- 12.Havryk AP, Gilbert M, Burgess KR. Spirometry values in Himalayan high altitude residents (Sherpas) Respir Physiol Neurobiol. 2002;132:223–32. doi: 10.1016/s1569-9048(02)00072-1. [DOI] [PubMed] [Google Scholar]
- 13.Malik SL, Pandey AK. Respiratory adaptation to high altitude in adolescent Bod girls of the Western Himalayas. Ann Hum Biol. 1993;20:575–81. doi: 10.1080/03014469300002982. [DOI] [PubMed] [Google Scholar]
- 14.Malik SL, Singh IP. Lung function in highlander Bods of Ladakh. Am J Phys Anthropol. 1979;51:383–8. doi: 10.1002/ajpa.1330510309. [DOI] [PubMed] [Google Scholar]
- 15.Wood S, Norboo T, Lilly M, Yoneda K, Eldridge M. Cardiopulmonary function in high altitude residents of Ladakh. High Alt Med Biol. 2003;4:445–54. doi: 10.1089/152702903322616191. [DOI] [PubMed] [Google Scholar]
- 16.Qazi RI, Qazi S, Laharwal MA. Peak expiratory flow rates in young Kashmiri adults through electronic spirometry. JK Pract. 2003;10:279–80. [Google Scholar]
- 17.Weitz CA, Garruto RM, Chin CT, Liu JC, Liu RL, He X. Lung function of Han Chinese born and raised near sea level and at high altitude in western China. Am J Hum Biol. 2002;14:494–510. doi: 10.1002/ajhb.10063. [DOI] [PubMed] [Google Scholar]
- 18.West JB. High altitude medicine. Am J Respir Crit Care Med. 2012;186:1229–37. doi: 10.1164/rccm.201207-1323CI. [DOI] [PubMed] [Google Scholar]
- 19.Debray P, Shreevatsa BM, M G RB, Sen TK, Roy S, Saha CG. A comparative study of the peak expiratory flow rate of Indian and Nepalese young adults in a teaching institute. JNMA J Nepal Med Assoc. 2008;47:7–11. [PubMed] [Google Scholar]
- 20.Kashyap S, Puri DS, Bansal SK. Peak expiratory flow rates of healthy tribal children living at high altitudes in the Himalayas. Indian Pediatr. 1992;29:283–6. [PubMed] [Google Scholar]