

Abstract
A 60-year-old diabetic man presented with a history of decrease in vision in both eyes since 2 weeks. At presentation, best corrected visual acuity (BCVA) in the right eye (RE) was 20/30 and that in the left eye (LE) was 20/80. The right fundus revealed a grayish reflex, yellowish crystalline deposits and retinal pigment epithelial hyperplasia at the macula. The left fundus showed subretinal fluid and temporal subretinal hemorrhage near a grayish reflex at the macula. A diagnosis in both eyes of idiopathic macular telangiectasia (IMT) type 2A with RE stage 4 and LE stage 5, choroidal neovascularization (CNVM) was made. The patient was treated with photodynamic therapy (PDT) in LE. The visual acuity improved to 20/40 over the next 6 months. At a 4-year follow-up, he developed decreased vision in RE diagnosed as IMT with CNV and was treated with intravitreal ranibizumab. At 6-month follow-up post injection, the vision was 20/40p.
Keywords: Choroidal neovascular membrane, idiopathic macular telangiectasia, photodynamic therapy, ranibizumab
Idiopathic macular telangiectasia (IMT) was first described by Gass et al.[1] They described three groups of the disease: Group 1 being congenital familial, Group 2 being acquired and Group 3 being obliterative associated with central nervous system vasculopathy. Yannuzzi termed this entity as idiopathic macular telangiectasia with two distinct types (type I or aneurysmal telangiectasia and type II or perifoveal telangiectasia) for better understanding of the disease.[2] The third type, obliterative telangiectasia, was omitted. Most patients retain excellent visual acuity for many years. As less than 5% of all cases of IMT undergo significant visual loss, observation is prudent in most cases. Multiple treatment modalities for treatment of choroidal neovascularization (CNV) secondary to IMT have been reported. We report a case of bilateral IMT with successive development of CNV in both the eyes. The patient was treated with photodynamic therapy (PDT) in one eye and with intravitreal ranibizumab in the other with satisfactory visual outcomes in both the eyes.
Case Report
A 60-year-old man presented with a history of decrease in vision in the left eye (LE) for last 15 days. He was a known diabetic on treatment since past 10 years. On examination, his best corrected visual acuity (BCVA) in the right eye (RE) was 20/30 and that in LE was 20/80. Anterior segment examination was unremarkable except nuclear sclerosis grade 1 in both eyes (BE). Fundus examination RE revealed grayish retina temporal to fovea, about 500 μm wide, with multiple yellowish crystalline deposits and pigments. The left fundus examination showed the presence of subretinal fluid with subretinal hemorrhage measuring about 400 μm in width. A clinical diagnosis of RE type 2A stage 4 IMT and LE type 2A stage 5 IMT was made. The clinical findings were confirmed on optical coherence tomography (OCT) and fundus fluorescein angiography (FFA) [Fig. 1]. The patient underwent PDT (greatest linear dimension of 1310 μm, a spot size of 2310 μm) as per the standard protocol.
Figure 1.
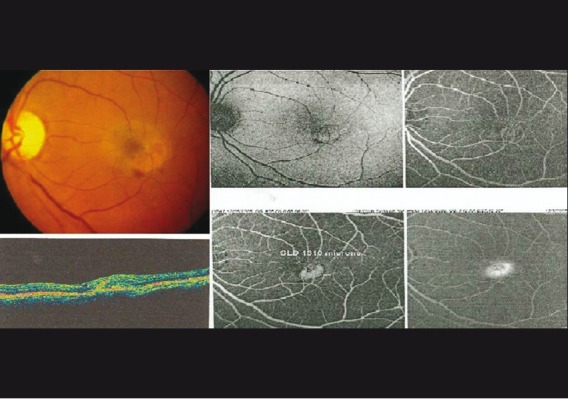
Left eye fundus photograph showing stage 5 idiopathic macular telangiectasia (IMT) confirmed on optical coherence tomogram (OCT) and fundus fluorescein angiography (FFA)
At 1 month of follow-up, LE BCVA was maintained at 20/80 with resolution of subretinal fluid and hemorrhage on fundus examination. FFA showed no signs of activity in the LE. The patient was on regular follow-up with stable findings [Fig. 2]. At 4 years of follow-up, he presented with complaints of decrease in vision in RE since the past 4 weeks. The BCVA in the RE was 20/80 and in the LE was 20/40. RE fundus examination revealed the presence of subretinal hemorrhage temporal to the fovea about 300 μm in size and LE scarred membrane. FFA confirmed the activity in RE and scarring in LE [Fig. 3]. The patient received two consecutive monthly intravitreal ranibizumab (Lucentis) injections 0.5 mg/0.05 ml in RE. At 1-month follow-up following the second injection, his RE BCVA improved to 20/40 with decrease in retinal thickness on OCT. Improved visual acuity and clinical findings including bilateral macular scar with a vision of 20/40 was maintained till the 6th month follow-up [Fig. 4].
Figure 2.
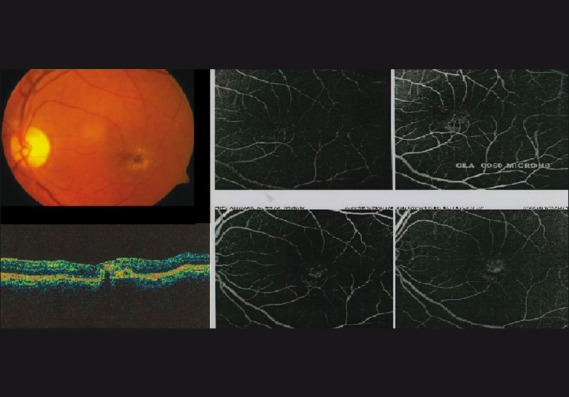
Resolution of the choroidal neovascular membrane (CNVM) post photodynamic therapy (PDT) therapy
Figure 3.
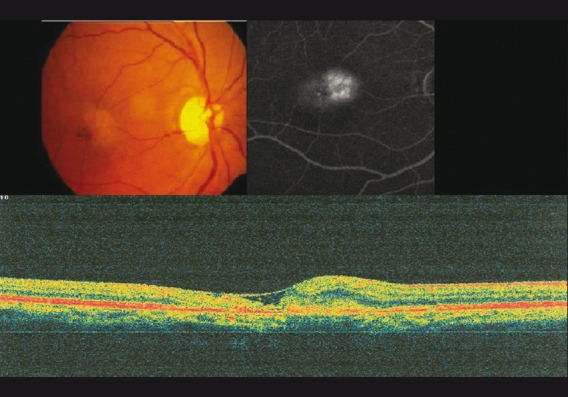
Right eye fundus photograph showing stage 5 idiopathic macular telangiectasia (IMT) confirmed on optical coherence tomogram (OCT) and fundus fluorescein angiography (FFA)
Figure 4.
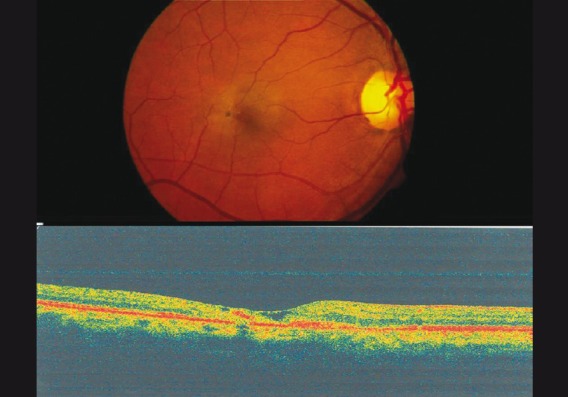
Resolution of the choroidal neovascular membrane (CNVM) post intravitreal ranibizumab
Discussion
Treatment of CNV associated with IMT has always been controversial. Multiple treatment modalities including laser photocoagulation, intravitreal triamcinolone, and transpupillary thermotherapy have been reported. Hussain et al., in a prospective interventional case series of 121 eyes with CNV due to IMT, showed effective stabilization of vision over a 1-year follow-up.[3]
Recently, antivascular endothelial growth factor (VEGF) drugs have been used in exudative macular disorders with considerable success. Issa et al. in an 18-month follow-up showed decreased fluorescein leakage, decreased central macular thickness and improved visual acuity with intravitreal bevacizumab (Avastin) although the effect was temporary with a rebound at 3–4 months post injection.[4] Combined PDT with ranibizumab for CNV following IMT has been described in an isolated case report by Rishi et al., wherein at a 16-week follow-up, there was regression of subretinal fluid with a two line vision gain on Snellen charts which was maintained till a 9-month follow-up.[5]
In this report, we describe a patient with bilateral CNV secondary to IMT treated in one eye with PDT and in the other eye with intravitreal ranibizumab (Lucentis). Both the treatment modalities were successful in visual improvement. Retinal pigment epithelium damage caused by PDT needs a concerned approach. To the best of our knowledge, this is the first case of treatment of a CNV associated with IMT with ranibizumab alone. Further studies are warranted to establish the role of anti-VEGF with or without PDT for the treatment for CNV secondary to IMT.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Gass JD, Oyakawa RT. Idiopathic juxtafoveolar retinal telangiectasis. Arch Ophthalmol. 1982;100:769–80. doi: 10.1001/archopht.1982.01030030773010. [DOI] [PubMed] [Google Scholar]
- 2.Yannuzzi LA, Bardal AM, Freund B, Chen KJ, Eandi CM, Blodi B. Idiopathic macular telangiectasia. Arch Ophthalmol. 2006;124:450–60. doi: 10.1001/archopht.124.4.450. [DOI] [PubMed] [Google Scholar]
- 3.Hussain N, Das T, Khanna R, Mohan Ram LS, Sumasri K. One year results of verteporfin therapy for subretinal neovascularization associated with type 2A parafoveal telangiectasia. Clin Ophthalmol. 2007;1:483–8. [PMC free article] [PubMed] [Google Scholar]
- 4.Issa P, Finger R, Holz F, Scholl H. Eighteen-month follow-up of intravitreal bevacizumab in type 2 idiopathic macular telangiectasia. Br J Ophthalmol. 2008;92:941–5. doi: 10.1136/bjo.2007.129627. [DOI] [PubMed] [Google Scholar]
- 5.Rishi P, Shroff D, Rishi E. Combined photodynamic therapy and intravitreal ranibizumab as primary treatment for subretinal neovascular membrane associated with type 2 idiopathic macular telangiectasia. Graefes Arch Clin Exp Ophthalmol. 2008;246:619–21. doi: 10.1007/s00417-007-0732-0. [DOI] [PubMed] [Google Scholar]