

Abstract
Glaucoma drainage devices (GDDs) have been used in the management of complicated glaucomas. GDDs are associated with various complications such as tube migration, tube or plate exposure or extrusion, ocular motility disturbance and infection. Erosion of conjunctiva and exposure of the GDD remains a risk factor for the development of endophthalmitis. A wide range of materials have been used for this purpose, including sclera, dura, pericardium, fascia lata and cornea. However, there is no evidence to prove that any of these methods is superior to another for providing tectonic durability in the long term. In this report, we present a case of neovascular glaucoma, who developed conjunctival melting over the tube of an Ahmed Glaucoma Valve implant and was successfully managed with Cap Doxycycline.
Keywords: Ahmed Glaucoma Valve, conjunctival erosion, Doxycycline
Glaucoma drainage devices (GDDs) have been used in the management of complicated glaucomas, with a success rates of 22–97% in neovascular glaucoma (NVG).[1,2] Amongst the various complications associated with GDD,[3] erosion of conjunctiva and exposure of the GDD remains a risk factor for endophthalmitis. In a series of 542 eyes, conjunctival erosion overlying the Ahmed Glaucoma valve AGV was present in six of the nine eyes that developed endophthalmitis,[4] thereby emphasizing on providing a durable coverage for exposed GDD. Hence, it is critical to choose an ideal material for the coverage of exposed GDD amongst the wide range of materials available,[5,6,7] with no evidence to prove the superiority of any for providing tectonic durability in the long term.[8]
In this, we present a case of NVG who developed conjunctival melting over the tube of an Ahmed Valve implant and was successfully managed with Cap Doxycycline.
Case Report
A 69-year-old male, known case of chronic angle closure glaucoma with advanced glaucomatous neuropathy, was on medical management for his raised intraocular pressures. He was highly noncompliant with his medications and subsequently went on to develop vascular occlusions (superotemporal branched retinal vascular occlusion in the right eye and central retinal vascular occlusion in the left eye) due to sustained high intraocular pressures in both his eyes in a sequential manner followed by NVG in the left eye.
The patient had undergone phacotrabeculectomy with Mitomycin C MMC in both the eyes for chronic angle closure glaucoma 6 months back. There was a diffuse functional bleb with an intraocular pressure of 12 mmHg in right eye. The bleb was flat and vascularized in the left eye and intraocular pressure in the left eye was 36 mmHg. Ahmed Glaucoma Valve with donor scleral patch graft was implanted along with intravitreal Inj Avastin for NVG in the left eye. One month postoperative follow-up of the patient revealed a well-functioning implant with an exposed scleral graft and overlying conjunctival melt [Fig. 1]. The patient was put on Cap Doxycycline (100 mg bd) orally, eye drop Prednisolone acetate 8 times/day, E/D Tear substitute 8 times/day and continued eye drop Moxifloxacin 4 times/day, with a review on alternate days. After 2 weeks, there was complete epithelial healing over the exposed scleral graft [Fig. 2], anterior chamber was deep and the tube was functioning well. Doxycycline was continued once daily orally further for a period of 4 weeks and then stopped. During the 4 months follow-up period, the tube remained covered by intact conjunctival epithelium. On the last follow-up visit, the patient had a visual acuity of 6/18 in the left eye, the tube remained covered by intact conjunctival epithelium, and intraocular pressure was 13 mmHg on eye drop Brimonidine and the patient was advised a 3-monthly review [Fig. 3].
Figure 1.
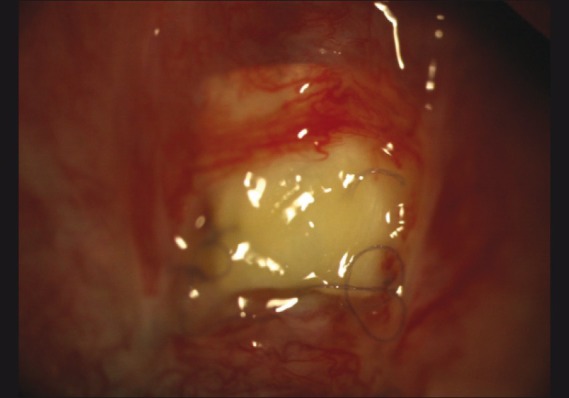
Avascularized and exposed scleral patch with functional implant
Figure 2.
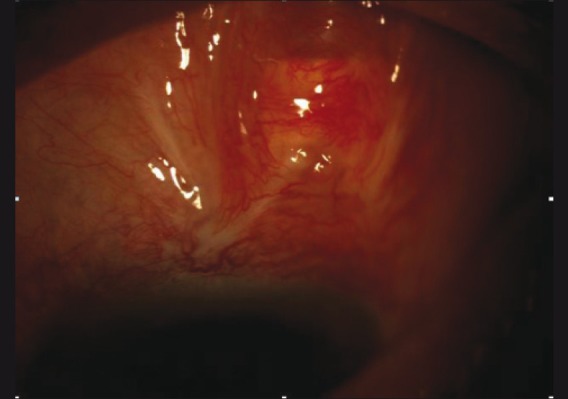
Showing total epithelialization over the exposed sclera
Figure 3.
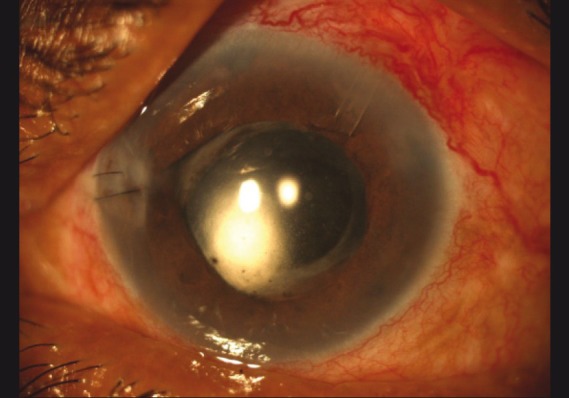
Last follow-up showing a completely covered tube with deep anterior chamber
Discussion
With the advent of donor autologous tissue for covering glaucoma drainage tubes, the incidence of tube erosion has decreased from 30% to less than 5%. In these handful of patients, mere observation is not advisable as the tube may serve as a nidus for infection, necessitating the removal of the tube. The causes of conjunctival erosion, though not well defined, probably comprise poor tissue turgor and mechanical rubbing of the eyelid margin against the tissue patch graft, excessive conjunctival tension over the tube, tube malposition, lack of a smooth tapered surface between the patch graft and host with poor ocular lubrication and minute amounts of absolute alcohol retained in the donor sclera.[9]
Doxycycline is a broad-spectrum antibiotic that chelates metal ions and is frequently used as part of the treatment of ocular surface diseases. Its therapeutic value has been attributed to an ability to inhibit matrix metalloproteinase (MMP) activity and both MMP and interleukin (IL)-1 synthesis. In a recent published report, rapid resolution and further recurrence of corneal erosions were prevented with a combination of Doxycycline and steroids.[10]
We presume in our case the therapeutic effects of Doxycycline and corticosteroids may be primarily the result of inhibition of metalloproteinase-9, or they may be secondary to their anti-inflammatory activity. The rapid clinical response to Doxycycline and corticosteroids in our patient could probably be the result of direct inhibition of inflammation or inflammation-induced metalloproteinase activity, along with an improved ocular surface with the use of frequent lubrication thereby reducing the mechanical rubbing force.
There is paucity of literature with regards to the best method to resolve the challenging problem of conjunctival erosion following GDD. Repeated surgical attempts at repair may be required and surgeons may find it intuitive to perform direct closure of dehisced conjunctiva. However, scarring at the implant site and poor conjunctival status due to chronic use of medications greatly reduces the chances of success. Conjunctival, scleral and amniotic membrane grafts have been reportedly used in the repair of exposed GDD. Our patient was managed conservatively with an impressive postoperative outcome. This adds to our knowledge on the pre-existing practices on the management of NVGs and may serve as a feasible alternative option to the current management practices. Thus, simple conservative measures can be attempted before resorting to complex surgeries.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Molteno AC. New implant for drainage in glaucoma: Clinical trial. Br J Ophthalmol. 1969;53:606–15. doi: 10.1136/bjo.53.9.606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Assaad MH, Baerveldt G, Rockwood EJ. Glaucoma drainage devices: Pros and cons. Curr Opin Ophthalmol. 1999;34:349–52. doi: 10.1097/00055735-199904000-00012. [DOI] [PubMed] [Google Scholar]
- 3.Nguyen QH. Avoiding and managing complications of glaucoma drainage implants. Curr Opin Ophthalmol. 2004;15:147–50. doi: 10.1097/00055735-200404000-00016. [DOI] [PubMed] [Google Scholar]
- 4.Al-Torbak AA, Al Shahwan S, Al Jadaan I, Al-Hommadi A, Edward DP. Endophthalmitis associated with Ahmed Glaucoma Valve implant. Br J Ophthalmol. 2005;89:454–8. doi: 10.1136/bjo.2004.049015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Freedman J. Scleral patch grafts with molteno setons. Ophthalmic Surg. 1987;18:532–4. [PubMed] [Google Scholar]
- 6.Raviv T, Greenfield DS, Liebmann JM, Sidoti PA, Ishikawa H, Ritch R. Pericardial patch grafts in glaucoma implant surgery. J Glaucoma. 1998;7:27–32. [PubMed] [Google Scholar]
- 7.Brandt JD. Patch grafts of dehydrated cadaveric duramater for tube shunt glaucoma surgery. Arch Ophthalmol. 1993;111:1436–9. doi: 10.1001/archopht.1993.01090100144042. [DOI] [PubMed] [Google Scholar]
- 8.Lankaranian D, Reis R, Henderer JD, Choe S, Moster MR. Comparison of single thickness and double thickness processed pericardium patch graft in glaucoma drainage device surgery: A single surgeon comparision of outcome. J Glaucoma. 2008;17:48–51. doi: 10.1097/IJG.0b013e318133fc49. [DOI] [PubMed] [Google Scholar]
- 9.Enzenauer RW, Sieck EA, Vavra DE, Jacobs EP. Residual etanolcontent of donor sclera after storage in 95% ethanol and saline rinse of various durations. Am J Ophthalmol. 1999;128:522–4. doi: 10.1016/s0002-9394(99)00190-7. [DOI] [PubMed] [Google Scholar]
- 10.Durson D, Kim MC, Solomon A, Pflugfelder SC. Treatment of recalcitrant recurrent corneal erosions with inhibitors of matrix metalloproteinase-9, doxycycline and corticosteroids. Am J Ophthalmol. 2001;132:8–13. doi: 10.1016/s0002-9394(01)00913-8. [DOI] [PubMed] [Google Scholar]