

Abstract
Purpose
An active lifestyle is widely recognized as having a beneficial effect on cardiovascular health. However, no clear consensus exists as to whether exercise training increases overall physical activity energy expenditure (PAEE) or whether individuals participating in regular exercise compensate by reducing their off-exercise physical activity. The purpose of this study was to evaluate changes in PAEE in response to aerobic training (AT), resistance training (RT), or combined aerobic and resistance training (AT/RT).
Methods
Data are from 82 participants in the Studies of Targeted Risk Reduction Interventions through Defined Exercise—Aerobic Training versus Resistance Training study, a randomized trial of overweight (body mass index = 25–35 kg·m−2) adults, in which participants were randomized to receive 8 months of AT, RT, or AT/RT. All subjects completed a 4-month control period before randomization. PAEE was measured using triaxial RT3 accelerometers, which subjects wore for a 5- to 7-d period before and after the exercise intervention. Data reduction was performed with a previously published computer-based algorithm.
Results
There was no significant change in off-exercise PAEE in any of the exercise training groups. We observed a significant increase in total PAEE that included the exercise training, in both AT and AT/RT but not in RT.
Conclusions
Eight months of exercise training was not associated with a compensatory reduction in off-exercise physical activity, regardless of exercise modality. The absence of compensation is particularly notable for AT/RT subjects, who performed a larger volume of exercise than did AT or RT subjects. We believe that the extended duration of our exercise training program was the key factor in allowing subjects to reach a new steady-state level of physical activity within their daily lives.
Keywords: ACCELEROMETER, CALORIC EXPENDITURE, AEROBIC TRAINING, RESISTANCE TRAINING, COMPENSATION
Exercise has long been identified as an important means of health maintenance in individuals of all ages. However, controversy exists as to whether individuals who exercise regularly compensate by being less active during other nonexercise daily activities. Multiple studies have demonstrated that increased total energy expenditure by itself is associated with significantly lower all-cause morbidity and mortality (11,14). Therefore, exercise that is compensated for by reduced off-exercise physical activity may lessen improvements in health.
A clear consensus has yet to emerge from existing studies that examine the association between off-exercise energy expenditure and exercise training. A literature review addressing this topic (24) posited that older subjects are more likely to compensate for exercise training by lowering off-exercise energy expenditure. This conclusion is supported by data from multiple exercise training studies examining the effect of aerobic training (AT) alone (2,15,16,19), as well as studies with a resistance training (RT) component (17,26). However, there have also been prior studies of exercise training in older individuals (>60 yr old) in which no compensatory decrease in off-exercise physical activity is demonstrated (3,9,10). Lastly, one previous study found a nonsignificant increase in off-exercise physical activity in younger men in response to AT (18).
STRRIDE AT/RT (Studies of Targeted Risk Reduction Interventions through Defined Exercise—Aerobic Training vs Resistance Training) was designed in part to define the ambiguous relationship between exercise training and total energy expenditure. An additional purpose was to compare the effects of AT, RT, and the combination of the two (AT/RT) on both total and off-exercise energy expenditure. To our knowledge, this study is the first to directly compare the effect of different exercise training modalities on energy expenditure.
METHODS
Study subjects
Research teams at Duke University and East Carolina University (ECU) recruited a total of 234 subjects from communities in and surrounding Durham and Greenville, NC. Written informed consent was obtained from all subjects using a consent form approved by the institutional review board of both institutions. Of these, 196 subjects completed the 4-month control/run-in period and were randomized to one of the three exercise groups. Out of 196 subjects, 144 subjects completed the full exercise training intervention. Of these 144, there were 92 subjects with usable accelerometer data at both the pre- and postexercise time points. Reasons for unusable accelerometer data include device malfunction or loss, insufficient amount of time when the device was worn (data excluded when device was worn <12 h·d−1), and implausible energy expenditure values (data excluded when >20,934 kJ were recorded per day). Of these 92 subjects, 10 additional subjects were excluded because of implausible data for change in physical activity energy expenditure (PAEE) (decrease >100 kJ·h−1 or increase >200 kJ·h−1). Thus, 82 subjects completed the study with plausible accelerometer data before and after exercise, and these are included in the present analysis. Importantly, of the 144 completers, there were no significant differences in age, height, weight, body mass index (BMI), peak , or fat percentage between the 82 included and the 62 who were not included in the analyses (all P > 0.10). Study inclusion criteria included age 18–70 yr, sedentary (exercising <1–2 times per week), overweight or moderately obese (BMI = 25–35 kg·m−2), and with mild to moderate dyslipidemia (either LDL cholesterol = 130–190 mg·dL−1 or HDL cholesterol <40 mg·dL−1 for men or <45 mg·dL−1 for women). Subjects were excluded if they used tobacco; had a history of diabetes, hypertension, musculoskeletal disorders, or CAD; were currently dieting or intending to diet; taking confounding medications; or were unwilling to be randomized into any group.
Exercise training protocols
All subjects were asked to maintain their current lifestyle for a control period of 4 months, followed by randomization into one of three exercise training groups: 1) RT: 3 d·wk−1, 3 sets per day on 8 different major muscle groups, 8–12 repetitions per set; 2) AT: 14 kcal·kg−1 body weight per week, calorically equivalent to approximately 12 miles·wk−1, at 65%–80% peak ; and 3) AT/RT: the combination of the full AT and the full RT programs. All three groups completed a total of 8 months of exercise training.
A ramp period of 8–10 wk, designed to gradually increase the amount of aerobic exercise done over time, was prescribed to all subjects in the AT and AT/RT groups. An HR range corresponding to approximately 75% of peak was determined using data from the maximal treadmill test. Subjects were instructed to maintain their HR within this range during AT using a downloadable HR monitor (Polar Electro, Inc., Woodbury, NY) that stored HR data for each subject. Exercise modes included treadmills, elliptical trainers, and cycle ergometers. The majority of training sessions were conducted on-site at Duke and ECU, and some exercise took place off-site. All sessions were verified using the Polar HR monitors. Caloric expenditure was calculated for each subject and was used to prescribe a total number of AT minutes per week, with a goal of expending 58.6 kJ·kg−1 body weight, equivalent to 14 kcal·kg−1·wk−1.
The RT groups were prescribed three sessions per week, three sets each session of 8–12 repetitions, for eight different weight lifting exercises designed to target all major muscle groups. The ramp period began with one set during weeks 1–2 and two sets during weeks 3–4, building up to the prescribed three-set amount on week 5. CYBEX machines (Medway, MA) were used for the majority of the exercises. For each exercise, subjects used the maximum amount of weight that they could lift 8–12 times with proper form. The weight for each exercise increased under the direction of the exercise trainers by 5 lb each time the participant could complete 12 repetitions for all three sets on two consecutive sessions. All RT sessions were verified by direct trainer supervision (at ECU) or use of the FitLinxx Strength Training Partner™ (FitLinxx, Norwalk, CT) at Duke. FitLinxx is a state-of-the-art computer system using an infrared laser to capture information on the amount of weight lifted and number of repetitions completed. A small touch screen monitor also provided instruction to participants regarding the proper speed at which to execute repetitions and amount of resting time to take between sets. The validity and reliability of the FitLinxx system were determined by comparing the online computer results with those obtained from direct observation and recordings of weight lifted, number of repetitions, sets, etc., for each weight machine. The directly observed and hand-recorded data corresponded exactly (100%) with that obtained from the computer for each set and for each machine.
Cardiopulmonary exercise test
Cardiopulmonary exercise tests with a 12-lead ECG and expired gas analysis were performed on a treadmill using a TrueMax 2400 metabolic cart (ParvoMedics, Sandy, UT). Gas volume (via a 3-L syringe pumped at flow rates approximating 30, 80, 120, 180, and 300 L·min−1) and gas concentrations (calibration gas = 4% CO2 and 16% O2) were calibrated before each test. The graded treadmill test consisted of 2-min stages that progressed as follows: 3 mph at 0% grade, 3 mph at 5%, 3 mph at 7.5%, 3 mph at 10%, 3.4 mph at 10%, 3.4 mph at 12%, 3.8 mph at 12%, 4.0 mph at 12%, 5.0 mph at 9.5%, and 5.5 mph at 9.5%. The two highest consecutive 15-s readings from each test were averaged to determine absolute peak (L·min−1). A maximal RER of ≥1.10 was considered a successful max test. In some cases, the peak RER did not achieve the 1.10 criteria. In these cases, if the pre- and posttest peak RER were not similar, the data were not used. Max tests were conducted between 8:00 a.m. and 5:00 p.m.
Accelerometers and data reduction
As Hollowell et al. described in a previous study (7), subjects wore a triaxial RT3 accelerometer (Stayhealthy, Inc., Monrovia, CA) at three separate time points: at the start and end of the control period (i.e., before exercise training) and during the final week of the exercise training program. At each time point, subjects were instructed to wear the device continuously (including exercise time) for 5–7 d, except for bathing and sleeping. Free-living PAEE determined via the RT3 accelerometer has been shown to correlate significantly (r = 0.67, P < 0.05) with that obtained via doubly labeled water in overweight/obese adults, with no significant differences found between the two methods (12). The RT3 has also been found to be sensitive to changes in treadmill speed over varying speeds with no significant differences found between PAEE from RT3 versus indirect calorimetry for any walking speed (12).
The RT3 accelerometer estimated the amount of activity kilocalories expended during each minute that it was worn, on the basis of the subject's weight and recorded movement in the three planes of motion. The approach described by Hollowell et al. (7) was used to sum this activity data for each day. We excluded days in which the accelerometer was worn for <12 h and days in which it recorded >20,934 kJ (5000 kcal) of energy expenditure, believing that this represented the upper limit of plausible daily energy expenditure for subjects in this study. Daily activity was expressed in terms of kilojoules per hour of recorded data, to normalize for subjects wearing the device for different amounts of time each day. The resulting variable was labeled PAEE.
At each of the three time points (before control period and before and after exercise), the PAEE (kJ·h−1) values from all days with full accelerometer data were averaged. Our primary analysis variable was PAEE change. The records of study participants with implausibly large PAEE changes that could potentially have resulted from accelerometer malfunction were eliminated. Cutoff values were a PAEE decrease of >100 kJ·h−1 or a PAEE increase of >200 kJ·h−1. In comparison, the 14-kcal·kg−1·wk−1 AT program corresponds to approximately 55.8 kJ·h−1 (assuming 12 h of accelerometer wearing per day for 7 d), for an 80-kg individual averaged during a full week. We reasoned that because the subjects in the present study were already sedentary physically inactive individuals, a further decrease of 100 kJ·h−1 would be a very large change and so quite unlikely. Similarly, we reasoned that because the aerobic exercise prescription corresponds to approximately 56 kJ·h−1, an increase of 200 kJ·h−1 (almost 3.6 times as large as the aerobic exercise prescription) was very unlikely, especially for nonexercisers. We believe that these were very conservative assumptions for data exclusion. Importantly, these criteria were used consistently across all three groups and would therefore not result in any bias effect on any group.
Removal of exercise data
To examine the effect of exercise training on off-exercise physical activity, we removed all known exercise data from the raw accelerometer files. As described by Hollowell et al. (7), 30 min of data both before and after all identified exercise periods were also removed to exclude warm-up and cool-down time, as well as time spent commuting to and from the exercise facility.
At Duke, multiple data sources (gym check-in, HR monitor, and FitLinxx™ data and direct observation by exercise training staff) allowed for verification of specific times that exercise took place. In addition, AT has a characteristic fingerprint on RT3 data (Fig. 1), and this fingerprint allowed us to verify that data being removed was indeed from an AT workout.
FIGURE 1.
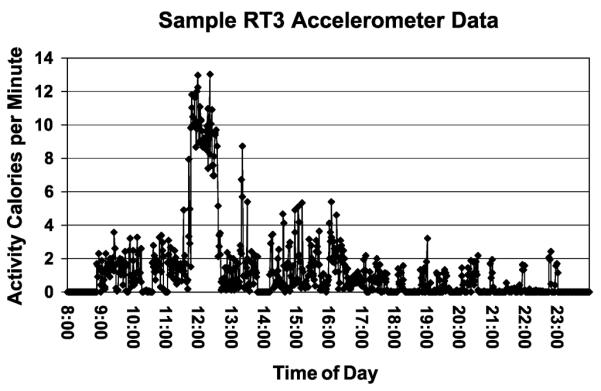
Graphical representation of a typical day's accelerometer data.
Subjects who completed their training at the ECU facility did not have automated data with which to identify specific times at which exercise training sessions occurred. However, detailed logs of the specific days on which study participants completed exercise training sessions were maintained. In the case of AT subjects, we closely examined accelerometer data on exercise training days for the distinct AT fingerprint and removed the corresponding exercise data along with 30 min before and after that session. We were unable to identify a distinct RT fingerprint with RT3 accelerometer data and thus could not remove RT sessions from the accelerometer data of ECU research subjects. Therefore, data from RT and AT/RT subjects at ECU were not used in this portion of our final analysis.
Measuring RT energy expenditure
To compare the accuracy of the RT3 for measuring energy expenditure during the RT sessions, we experimentally measured caloric expenditure during a typical RT workout in a smaller group of five study participants, using indirect calorimetry (TrueMax 2400 metabolic cart; ParvoMedics). Oxygen consumption and caloric expenditure were assessed continuously throughout one complete RT session. Subjects performed all three sets for each exercise with 45 s of rest between each set. The subject and the metabolic cart (plugged into a long extension cord) moved together from one weight station to the next with no interruption in data collection. In addition, 5 min of resting metabolic data before and upon completion of the workout were collected.
Statistical methods
Data were analyzed using ANOVA (StatView or SAS Software; SAS Institute, Cary, NC). When the ANOVA was significant (P < 0.05), a Fisher protected least significant difference post hoc analysis was performed to determine differences between exercise groups (Fig. 2). Three pairwise comparisons (i.e., between the three exercise groups: AT, RT, and AT/RT compared with each other) were of interest. P < 0.05 was considered significant in post hoc testing. In addition, paired two-tailed t-tests were used to determine whether the after versus before score for changes within each group differed. There were no a priori power calculations because the variables in the present article were not primary outcome variables for the STRRIDE AT/RT study. Finally, to determine whether older individuals were more likely to compensate for increases in exercise PAEE by decreasing off-exercise PAEE, we tested for the effect of age in this analysis. Age was added as a covariate to the ANOVA with group as the independent variable and change in off-exercise PAEE as the dependent variable. In addition, a simple correlation between age and off-exercise PAEE was performed.
FIGURE 2.

Change score by group for total PAEE (A) and off-exercise PAEE (B). Error bars indicate SE. Although the control period (which includes the change that occurred during the run-in period in all 82 subjects) has been included in this figure for visual comparison only, there were no statistical comparisons between the control period data and the exercise groups. The only statistical comparisons were between the three independent exercise training groups. †Significant difference from RT (P < 0.05).
RESULTS
Table 1 shows baseline demographics and exercise prescription statistics for individuals randomized to the three exercise groups. There were no significant differences between groups at baseline in any of the descriptive statistics. Adherence was slightly lower for each portion of the AT/RT group than for either AT or RT, but the total time accumulated for the AT/RT group remained almost double that of the other two groups.
TABLE 1.
Baseline demographics and exercise prescription details.
| AT Only (n = 28) | AT/RT (n = 26) | RT (n = 28) | P | |
|---|---|---|---|---|
| Male | 14 | 10 | 8 | — |
| Female | 14 | 16 | 20 | — |
| Age (yr) | 51.8 ± 9.2 | 47.5 ± 11.0 | 50.6 ± 12.4 | 0.41 |
| Height (cm) | 170.2 ± 8.7 | 170.6 ± 9.0 | 168.2 ± 12.1 | 0.64 |
| Weight (kg) | 88.4 ± 2.2 | 90.0 ± 12.4 | 86.3 ± 16.9 | 0.62 |
| BMI (kg·m−2) | 30.5 ± 3.1 | 30.9 ± 3.2 | 30.3 ± 3.1 | 0.60 |
| (mL·kg−1·min−1) | 27.3 ± 5.6 | 26.9 ± 5.5 | 25.9 ± 6.3 | 0.81 |
| Body fat (%) | 38.4 ± 7.3 | 39.9 ± 7.8 | 39.3 ± 8.7 | 0.73 |
| PAEE (kJ·h−1) | 225.6 ± 89.8 | 188.9 ± 47.7 | 194.6 ± 68.5 | 0.38 |
| Aerobic Exercise | ||||
| Intensity (% peak ) | 65–80 | 65–80 | N/A | — |
| Rx amount (kcal·kg−1·wk−1)a | 14 | 14 | N/A | — |
| Rx time (min·wk−1) | 132.7 ± 24.8 | 134.6 ± 24.8 | N/A | — |
| Adherence (%) | 89.9 ± 10.2 | 83.8 ± 16.6 | N/A | — |
| Actual frequency (sessions per week) | 3.1 ± 0.5 | 3.0 ± 0.6 | N/A | — |
| Actual time (min·wk−1)b | 120.6 ± 21.2 | 111.3 ± 28.9 | N/A | — |
| Resistance Exercise | ||||
| Intensity | N/A | Progressive | Progressive | — |
| Rx amount (sets per week)c | N/A | 72 | 72 | — |
| Rx time (min·wk−1) | N/A | 180 | 180 | — |
| Adherence (%) | N/A | 81.6 ± 14.7 | 84.0 ± 11.9 | — |
| Actual frequency (sessions per week) | N/A | 2.45 ± 0.44 | 2.52 ± 0.36 | — |
| Actual amount (sets per week)d | N/A | 58.8 ± 10.6 | 60.5 ± 8.6 | — |
Values are means ± SD. Significance testing performed using ANOVA.
All data were collected before the 8-month exercise intervention.
Rx amount (14 kcal·kg−1·wk−1) is approximately calorically equivalent to 12 miles of jogging per week.
Actual time (min·wk−1) = Rx time × adherence.
Rx amount (72 sets per week) = 3 d·wk−1, 3 sets of 8–12 repetitions, on 8 different machines.
Actual amount (sets per week) = Rx amount × adherence.
N/A, not applicable; , relative peak oxygen consumption Rx, prescription.
Figure 2A shows the mean change in total PAEE, before and after exercise intervention, for each exercise group. Data for the change during the control run-in period for all 82 subjects are also included for visual comparison only because no statistical comparisons are made between the changes during the control period and any exercise group change. AT and AT/RT both demonstrated a significant increase in total PAEE (Table 2), and the ANOVA main effects showed a significant difference in total PAEE change among groups (P = 0.012). Fisher post hoc testing indicated that the total PAEE changes in AT and AT/RT were different from that in RT (P = 0.053 and P = 0.003, respectively). There were no significant differences between AT and AT/RT (P = 0.26). Figure 2B shows the mean change in off-exercise PAEE for each exercise group. Again, data for the change during the control run-in period for all 82 subjects are also included for visual comparison only because no statistical comparisons are made between the changes during the control period and any exercise group. No group demonstrated a significant change in off-exercise PAEE, and ANOVA main effects failed to show a significant difference in off-exercise PAEE change among groups (P = 0.42). Baseline and change scores for total and off-exercise PAEE for each group are shown in Table 2.
TABLE 2.
Baseline PAEE and change score by group.
| Control Period |
RT Only |
AT Only |
AT/RT |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Change Score | P | Baseline | Change Score | P | Baseline | Change Score | P | Baseline | Change Score | P | |
| Total PAEE (kJ·h−1) | 210.3 ± 77.9 | 4.8 ± 54.4 | 0.36 | 194.6 ± 68.5 | 7.7 ± 51.2 | 0.43 | 225.6 ± 89.8 | 38.4 ± 65.1 | 0.004a | 188.9 ± 47.7 | 55.8 ± 57.7 | <0.0001a |
| n | 106 | 28 | 28 | 26 | ||||||||
| Nonexercise PAEE (kJ·h−1) | 210.3 ± 77.9 | 4.8 ± 54.4 | 0.36 | 186.1 ± 61.4 | −1.8 ± 44.4 | 0.86 | 220.2 ± 86.7 | 1.6 ± 57.0 | 0.89 | 189.0 ± 46.1 | 19.1 ± 61.7 | 0.17 |
| n | 106 | 21 | 27 | 21 | ||||||||
| Peak (kg−1) | 26.77 ± 5.46 | −0.61 ± 2.19 | 0.006 | 26.00 ± 6.27 | 1.04 ± 2.4 | 0.03 | 27.18 ± 5.65 | 3.31 ± 4.16 | 0.0004 | 26.89 ± 5.54 | 3.77 ± 3.28 | <0.0001 |
| n | 106 | 28 | 28 | 28 | ||||||||
| RT strength (kg lifted per session) | N/A | N/A | N/A | 6787.6 ± 1982.2 | 3394.4 ± 1354.7 | <0.0001a | N/A | N/A | N/A | 7517.2 ± 1762.7 | 2826.2 ± 1499.3 | <0.0001a |
| n | — | N/A | — | — | 19 | — | — | N/A | — | — | 20 | — |
Values are means ± SD. Change score = postexercise PAEE minus baseline PAEE. Nonexercise PAEE was calculated from accelerometer data in which known exercise training time was removed.
Significant change score, based on a two-tailed one-sample t-test (comparing baseline and postexercise PAEE).
Figure 3 examines energy expenditure from a typical week of AT workouts compared with a typical week of RT workouts. The energy expenditure from AT workouts was calculated, given our goal of 14-kcal·kg−1·wk−1 exercise energy expenditure for each subject. Energy expenditure from RT workouts was estimated using data from both the accelerometer and indirect calorimetry. It was expected that the AT energy expenditure would exceed that of RT. And this is the case, as is shown in the figure, although it is important to point out that these data are based on very few subjects (three men and two women). We also expected that the RT3-derived energy expenditure would be much less than that obtained from the metabolic cart measurements because of the fact that many of the arm and leg movements were likely not detected by the RT3. But, in fact, they were not very different. In Table 3, energy expenditures determined from the RT3, from the metabolic cart, and from RT literature review are presented. Here we see that the energy expenditures from all three sources are comparable, albeit the RT3 data are not surprisingly the lowest. This is certainly an area in need of additional confirmation.
FIGURE 3.
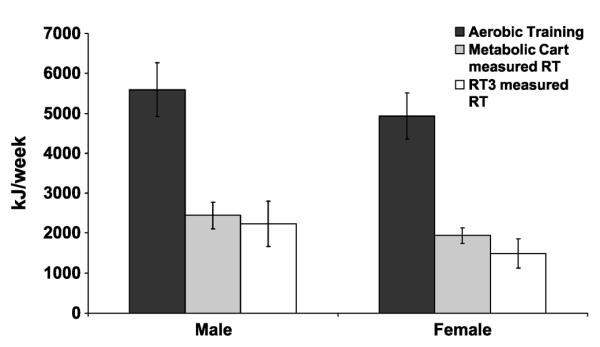
Total caloric expenditure per week in AT and RT. Average weekly energy expenditure from AT workouts was calculated, using our 14-kcal·kg−1·wk−1 target for each participant, along with the preexercise weight of each participant in our AT only and AT/RT groups (average preexercise weights of subjects in these groups were 95.4 kg for men and 84.1 kg for women). Average weekly RT energy expenditure was estimated by multiplying the average caloric expenditure from one RT workout (measured both with indirect calorimetry and RT3 accelerometer) by three, given that RT subjects were asked to complete three workouts per week.
TABLE 3.
RT energy expenditure.
| RT3 |
Metabolic Cart |
Literature Review |
||||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| Mean kilojoules per workout | 745.3 ± 189.2 | 497.8 ± 122.3 | 813.9 ± 111.7 | 646.1 ± 64.4 | 847.4–1093.2 | 576.9–875.5 |
| Mean kilojoules per kilogram per workout | 8.1 ± 1.7 | 6.2 ± 1.2 | 10.5 ± 2.7 | 8.8 ± 1.1 | 12.0–12.6 | 8.7–12.4 |
| n | 10 | 29 | 3 | 2 | — | — |
Average RT energy expenditure measured by RT3 accelerometer and metabolic cart, compared with values reported by other studies. Values are means ± SD. RT energy expenditure measurements from other studies were adjusted to account for differences in RT routine (for example, if a particular study entailed six exercises per circuit rather than eight as in our study, we multiplied the RT energy expenditure estimate by 4/3 to normalize for the number of exercises per circuit).
DISCUSSION
There is growing controversy over the effects of exercise programs on nonexercise activity levels. In the present study, none of the three exercise training programs was associated with reduced off-exercise physical activity. This observation, combined with that in a previous study that failed to find evidence of decreased off-exercise energy expenditure in AT programs of varying intensity and amount (7), strongly suggests that when the exercise training period is of sufficient duration, no off-exercise compensation occurs. In the present study, this finding is particularly noteworthy for participants in AT/RT, who performed a significantly larger amount of exercise than those in the AT or RT groups.
Effect on off-exercise physical activity
The lack of a compensatory decrease in off-exercise physical activity in any exercise group runs contrary to the findings of several prior studies. Many of these studies, however, were performed on older populations and with shorter exercise training durations than the current study. For example, three specific studies that observed a compensating decrease in off-exercise physical activity were performed on populations with a mean age ranging from 58 to 63 yr and with off-exercise physical activity being measured after only 12–14 wk of exercise training (16,17,19). The mean age of subjects in STRRIDE AT/RT, by contrast, was 50.3 ± 11.2 yr, and off-exercise physical activity was measured after 32 wk (8 months) of exercise training.
The present study failed to observe a significant effect of age on the relation between exercise group and change in off-exercise PAEE (ANOVA, P = 0.23). In addition, there was no significant correlation between age and change in off-exercise PAEE. This is possibly a result of an insufficient number of younger participants to power any investigation into an age-specific effect of exercise training. However, it may also indicate that the longer duration of the exercise training program, rather than participant age, is the key driving factor for the observed lack of compensation in off-exercise activity. Hollowell et al. (7) observed a similar lack of compensation after 8 months of AT of varying amount and intensity and concluded that the extended duration of exercise training allowed subjects to reach a new steady-state level of physical activity after adjusting to the chronic effects of regular exercise training. Indeed, two exercise training studies of longer duration (25 and 26 wk) on older individuals (>60 yr) failed to observe a compensatory decrease in off-exercise physical activity (3,9). Taken together, these results suggest that when the exercise training is of sufficient duration, no activity compensation occurs, even in a population of older individuals.
Subjects in the combined AT/RT group spent approximately twice the amount of time per week exercising compared with participants in AT or RT and had significantly greater exercise energy expenditure than individuals in either AT or RT alone. Therefore, if off-exercise compensation was to occur, subjects in this group would seem more likely to reduce their off-exercise energy expenditure than subjects in AT or RT because of exhaustion. However, the current results show no statistical difference between the off-exercise activities between any of the groups. Furthermore, although not statistically different, the positive change score for the AT/RT group was larger than that of either AT or RT alone. The lack of compensation in this group, thus, is particularly noteworthy.
Effect on total physical activity
Participation in an 8-month AT or combined AT/RT program led to an increase in total PAEE, whereas participation in RT did not. Subjects in both the STRRIDE I and STRRIDE AT/RT studies experienced an increase in total PAEE of similar magnitude in response to vigorous-intensity AT of an 8-month duration, although this increase was statistically significant only in the STRRIDE AT/RT study, likely because of the larger sample size (7).
There was no significant difference in total physical activity between participants in AT and AT/RT. Participation in AT and AT/RT led to significantly larger increases in PAEE than participation in RT. Combined, these results suggest that the AT portion of our exercise intervention was the primary factor driving the increase in total daily PAEE. However, it is also possible that the accelerometers used in this study did not adequately detect physical activity during RT workouts. Prior studies have indicated that triaxial accelerometers are valid instruments for measuring overall daily physical energy expenditure at a group level (particularly exercises like walking and jogging) (12,13,20). Despite this, accelerometers have also demonstrated a tendency to underestimate energy expenditure from certain activities of daily living, particularly those requiring isolated upper body movement (e.g., window washing and vacuuming), compared with measurements based on indirect calorimetry (1,6,8) or HR (5), in some cases, by as much as 30%–60% (6). It is possible that energy expenditure from the isolated upper and lower body RT exercises in this study was similarly not fully captured by RT3 accelerometers.
RT energy expenditure
To further examine this potential shortcoming in our data, we experimentally measured caloric expenditure during a typical RT workout in a smaller group of five study participants, using indirect calorimetry (TrueMax 2400 metabolic cart; ParvoMedics). The average total energy expenditure was 814 kJ per workout for three men and 646 kJ per workout for two women. By comparison, the average RT energy expenditure measured by RT3 during known RT times was 745 kJ per workout for men and 498 kJ per workout for women (Table 3). Because of the small sample size of subjects who completed RT measured by expired gas analysis, we were unable to demonstrate a significant difference between RT energy expenditure measured by RT3 and by indirect calorimetry. However, it is still probable that RT3 accelerometers underestimate RT energy expenditure, given that other studies measuring RT energy expenditure during circuit weight training routines similar to ours provide estimates that are more closely approximated by our indirect calorimetry rather than RT3 measurements (Table 3) (4,9,21,22,25). Four of these studies (4,9,21,22) provided weight measurements of their subjects, allowing us to calculate kilojoules per kilogram per workout as well (Table 3). This parameter is also more closely approximated by indirect calorimetry rather than RT3 measurement.
Although RT3 accelerometers likely underestimated RT energy expenditure compared with indirect calorimetry, the magnitude of this difference was likely not large enough to have significantly altered estimates of total PAEE in this study (Fig. 2A). When expressed in terms of PAEE, the difference between weekly RT energy expenditure measured by indirect calorimetry and by RT3 accelerometer is 5.3 kJ·h−1 for women and 2.4 kJ·h−1 for men (assuming 84 h of accelerometer data in a week). Thus, even with a more accurate method of measuring RT energy expenditure, it is likely that we would have replicated the finding that participation in AT or AT/RT leads to a significantly larger increase in total PAEE than participation in RT.
Regardless of the method used for measuring RT energy expenditure, subjects completing a full week of RT under the guidelines of our exercise training program had far lower exercise energy expenditure than that of subjects completing a full week of AT (Fig. 3). Extrapolated over a full week, RT energy expenditure measured by indirect calorimetry represented approximately 43.7% of weekly AT expenditure for men and 39.3% for women.
Strengths and limitations
The 8-month duration of exercise training in this study allowed us to examine the long-term effects of chronic exercise. In addition, multiple verification tools (described in “Methods”) allowed us to verify that study subjects were indeed performing the prescribed exercise over this time. Direct comparison of the effects of RT and AT on total and off-exercise physical activity was a novel aspect of this study.
Limitations of our study included the previously discussed tendency for RT3 accelerometers to inadequately capture the energy expenditure from RT and certain activities of daily living. In addition, although RT3 accelerometers are generally accurate instruments for measuring overall physical activity, interdevice variability exists—particularly during high-intensity activity (23). This may have complicated our efforts to capture intrasubject change in total and off-exercise physical activity at different time points, given that we did not seek to assign each subject the same specific accelerometer at each time point.
CONCLUSIONS
Eight months of exercise training was not associated with a compensating reduction in off-exercise physical activity, regardless of exercise type or amount. Aerobic training and combined aerobic and RT both resulted in a significant increase in total physical activity. These data combined with previous research findings strongly suggest that if the exercise training duration is of sufficient length, there is no off-exercise compensatory reduction in off-exercise physical activity.
Acknowledgments
This study was funded by the National Institutes of Health (grant R01-HL057354).
Footnotes
No conflict of interest exists.
The results of the present study do not constitute endorsement by the American College of Sports Medicine.
REFERENCES
- 1.Bassett DR, Jr, Ainsworth BE, Swartz AM, Strath SJ, O'Brien WL, King GA. Validity of four motion sensors in measuring moderate intensity physical activity. Med Sci Sports Exerc. 2000;32(9 suppl):S471–80. doi: 10.1097/00005768-200009001-00006. [DOI] [PubMed] [Google Scholar]
- 2.Blaak EE, Westerterp KR, Bar-Or O, Wouters LJ, Saris WH. Total energy expenditure and spontaneous activity in relation to training in obese boys. Am J Clin Nutr. 1992;55(4):777–82. doi: 10.1093/ajcn/55.4.777. [DOI] [PubMed] [Google Scholar]
- 3.Fujita K, Nagatomi R, Hozawa A, et al. Effects of exercise training on physical activity in older people: a randomized controlled trial. J Epidemiol. 2003;13(2):120–6. doi: 10.2188/jea.13.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Haddock BL, Wilkin LD. Resistance training volume and post exercise energy expenditure. Int J Sports Med. 2006;27(2):143–8. doi: 10.1055/s-2005-865601. [DOI] [PubMed] [Google Scholar]
- 5.Ham SA, Reis JP, Strath SJ, Dubose KD, Ainsworth BE. Discrepancies between methods of identifying objectively determined physical activity. Med Sci Sports Exerc. 2007;39(1):52–8. doi: 10.1249/01.mss.0000235886.17229.42. [DOI] [PubMed] [Google Scholar]
- 6.Hendelman D, Miller K, Baggett C, Debold E, Freedson P. Validity of accelerometry for the assessment of moderate intensity physical activity in the field. Med Sci Sports Exerc. 2000;32(9 suppl):S442–9. doi: 10.1097/00005768-200009001-00002. [DOI] [PubMed] [Google Scholar]
- 7.Hollowell RP, Willis LH, Slentz CA, Topping JD, Bhakpar M, Kraus WE. Effects of exercise training amount on physical activity energy expenditure. Med Sci Sports Exerc. 2009;41(8):1640–4. doi: 10.1249/MSS.0b013e31819c71a4. [DOI] [PubMed] [Google Scholar]
- 8.Howe CA, Staudenmayer JW, Freedson PS. Accelerometer prediction of energy expenditure: vector magnitude versus vertical axis. Med Sci Sports Exerc. 2009;41(12):2199–206. doi: 10.1249/MSS.0b013e3181aa3a0e. [DOI] [PubMed] [Google Scholar]
- 9.Hunter GR, Seelhorst D, Snyder S. Comparison of metabolic and heart rate responses to super slow vs traditional resistance training. J Strength Cond Res. 2003;17(1):76–81. doi: 10.1519/1533-4287(2003)017<0076:comahr>2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 10.Hunter GR, Wetzstein CJ, Fields DA, Brown A, Bamman MM. Resistance training increases total energy expenditure and free-living physical activity in older adults. J Appl Physiol. 2000;89(3):977–84. doi: 10.1152/jappl.2000.89.3.977. [DOI] [PubMed] [Google Scholar]
- 11.Inoue M, Iso H, Yamamoto S, et al. Daily total physical activity level and premature death in men and women: results from a large-scale population-based cohort study in Japan (JPHC study) Ann Epidemiol. 2008;18(7):522–30. doi: 10.1016/j.annepidem.2008.03.008. [DOI] [PubMed] [Google Scholar]
- 12.Jacobi D, Perrin A, Grosman N, et al. Physical activity related energy expenditure with the RT3 and TriTrac accelerometers in overweight adults. Obesity (Silver Spring) 2007;15(4):950–6. doi: 10.1038/oby.2007.605. [DOI] [PubMed] [Google Scholar]
- 13.Maddison R, Jiang Y, Hoorn SV, et al. Estimating energy expenditure with the RT3 triaxial accelerometer. Res Q Exerc Sport. 2009;80(2):249–56. doi: 10.1080/02701367.2009.10599559. [DOI] [PubMed] [Google Scholar]
- 14.Manini TM, Everhart JE, Patel KV, et al. Daily activity energy expenditure and mortality among older adults. JAMA. 2006;296(2):171–9. doi: 10.1001/jama.296.2.171. [DOI] [PubMed] [Google Scholar]
- 15.McLaughlin R, Malkova D, Nimmo MA. Spontaneous activity responses to exercise in males and females. Eur J Clin Nutr. 2006;60(9):1055–61. doi: 10.1038/sj.ejcn.1602417. [DOI] [PubMed] [Google Scholar]
- 16.Meijer EP, Westerterp KR, Verstappen FT. Effect of exercise training on physical activity and substrate utilization in the elderly. Int J Sports Med. 2000;21(7):499–504. doi: 10.1055/s-2000-7419. [DOI] [PubMed] [Google Scholar]
- 17.Meijer EP, Westerterp KR, Verstappen FT. Effect of exercise training on total daily physical activity in elderly humans. Eur J Appl Physiol Occup Physiol. 1999;80(1):16–21. doi: 10.1007/s004210050552. [DOI] [PubMed] [Google Scholar]
- 18.Meijer GA, Janssen GM, Westerterp KR, Verhoeven F, Saris WH, ten Hoor F. The effect of a 5-month endurance training programme on physical activity: evidence for a sex-difference in the metabolic response to exercise. Eur J Appl Physiol Occup Physiol. 1991;62(1):11–7. doi: 10.1007/BF00635626. [DOI] [PubMed] [Google Scholar]
- 19.Morio B, Montaurier C, Pickering G, et al. Effects of 14 weeks of progressive endurance training on energy expenditure in elderly people. Br J Nutr. 1998;80(6):511–9. doi: 10.1017/s0007114598001603. [DOI] [PubMed] [Google Scholar]
- 20.Nichols JF, Morgan CG, Sarkin JA, Sallis JF, Calfas KJ. Validity, reliability, and calibration of the Tritac accelerometer as a measure of physical activity. Med Sci Sports Exerc. 1999;31(6):908–12. doi: 10.1097/00005768-199906000-00022. [DOI] [PubMed] [Google Scholar]
- 21.Ortego AR, Dantzler DK, Zaloudek A, et al. Effects of gender on physiological responses to strenuous circuit resistance exercise and recovery. J Strength Cond Res. 2009;23(3):932–8. doi: 10.1519/JSC.0b013e3181a07884. [DOI] [PubMed] [Google Scholar]
- 22.Phillips WT, Ziuraitis JR. Energy cost of single-set resistance training in older adults. J Strength Cond Res. 2004;18(3):606–9. doi: 10.1519/1533-4287(2004)18<606:ECOSRT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Powell SM, Rowlands AV. Intermonitor variability of the RT3 accelerometer during typical physical activities. Med Sci Sports Exerc. 2004;36(2):324–30. doi: 10.1249/01.MSS.0000113743.68789.36. [DOI] [PubMed] [Google Scholar]
- 24.Van Etten LM, Westerterp KR, Verstappen FT, Boon BJ, Saris WH. Effect of an 18-wk weight-training program on energy expenditure and physical activity. J Appl Physiol. 1997;82(1):298–304. doi: 10.1152/jappl.1997.82.1.298. [DOI] [PubMed] [Google Scholar]
- 25.Westerterp KR. Physical activity as determinant of daily energy expenditure. Physiol Behav. 2008;93(4–5):1039–43. doi: 10.1016/j.physbeh.2008.01.021. [DOI] [PubMed] [Google Scholar]
- 26.Wilmore JH, Parr RB, Ward P, et al. Energy cost of circuit weight training. Med Sci Sports. 1978;10(2):75–8. [PubMed] [Google Scholar]