

Abstract
This case reports a rare condition of scurvy which posed a diagnostic difficulty. However, a thorough medical and diet history, along with clinical and histopathological examination aided in prompt diagnosis and successful management of the case. Occurrence of scurvy in today's contemporary society is said to be rare. Lack of fresh fruits and vegetables in the diet can lead to this condition. Diagnosis may be difficult due to its rarity and presence of non specific symptoms, which may pose a challenge to the clinician. A comprehensive history, clinical examination along with clinical and histopathological features led to arrive at a proper diagnosis. Local procedures and systemic therapy aided in the successful management of the case. A marked improvement in the gingival status and in the physical well being of the patient resulted after treatment. This case report describes the various manifestations of scurvy that posed a diagnostic challenge to the clinician. This condition which can be fatal if untreated can be easily prevented with inclusion of healthy food in the diet and modification in the lifestyle.
Keywords: Gingiva, scorbutic siderosis, scurvy, vitamin C
INTRODUCTION
Nutrition is the first need of man; his general health and well being are much dependent on his nutritional status. Nutritional deficiency disorders are well documented throughout history. The most commonly occurring disorders are those associated with protein calorie malnutrition or with vitamin deficiencies. Among the vitamin deficiencies, vitamin A, B-Complex, and vitamin D deficiencies are frequently encountered.[1]
Vitamin C deficiency is rarely found which causes Scurvy. This condition was seen with extended sea voyagers in 16th, 17th, and 18th centuries due to nutrition depletion when they were on sea.[2] It was not until about 300 years later that ascorbic acid was identified as main antiscorbutic substance in foods. Man, primates, the guinea pig, the red vested bul-bul bird and the fruit eating bat cannot synthesize vitamin C by means of metabolizing enzymes and they all rely on exogenous sources for the vitamin C needed in the diets.[3]
Vitamin C is abundantly distributed in the plant kingdom. The richest sources are vegetables and citrus fruits which include guava, grapes, oranges, and lemon.[4]
Vitamin C is the co-factor in diverse biological processes including collagen synthesis, neuromodulation, immune responses-chemotaxis, oxidative metabolism, scavenging of damaged free radicals along with other functions.[1]
Among human tissues, the highest concentration of ascorbic acid is found in pituitary and adrenal gland. It is also found in millimolar concentration in circulating neutrophiles.[1,5]
In scurvy, it affects hydroxylation of proline leading to lack of collagen formation. This lack of connective tissue support to the capillary walls leads to vascular fragility resulting in bleeding tendency which produces petechiae and ecchymoses in the tissues.[3]
Generalized manifestations of scurvy include bleeding abnormalities like petechiae, perifollicular and subperiosteal hemorrhage, ecchymoses, purpura, bleeding gums, and hemarthrosis. Other manifestations are bone pain, osteoporosis, arthralgias, myalgias, edema, ascites, cardiomegaly, and electrocardiographic abnormalities suggestive of cardiac disease. Fatigue, lassitude, and emotional changes (depression and hypochondriasis) sometime may precede the development of frank scurvy.[6]
Oral scurvy is characterized by intense red, painful swollen gingiva that bleeds spontaneously on slightest provocation, resulting in hemorrhages/purpuras/bruising. The general discoloration that results from bleeding and blood breakdown is called scurvy siderosis.[3]
Severe vitamin C deficiency is well known to lead to a severe periodontal syndrome called “scorbutic gingivitis” which is characterized by ulcerative gingivitis and rapid periodontal pocket development with tooth exfoliation.[7] It is often associated with fetid odor and poor oral hygiene.[3]
Most of the times, scurvy is misdiagnosed as vasculitis, blood dyscrasias, ulcerative gingivitis.[2] However, a thorough general physical examination, past medical history, diet history along with blood examination and histopathological examination can aid in formulating a proper diagnosis. Hence, such a case of scurvy is reported that posed a diagnostic challenge to the clinician.
CASE REPORT
A 32-year-old male, farmer by occupation, presented to Dept of Periodontics ACPM Dental College and Hospital, Dhule district of Maharashtra, India, with severe pain and bleeding gums since 1 month.
According to the patient, bleeding gums were associated with severe enlargement and pain that caused difficulty in speech, inability to eat, chew and carry out his routine oral hygiene practice. He also revealed that he had literally stopped consuming his regular diet and was only on liquids for the past 15 days owing to pain. Severe halitosis was noticed as he conversed about his problem.
Medical history revealed that he was not on any medication known to induce gingival hyperplasia, but he admitted of having been hospitalized few years back owing to severe joint pain involving knees and elbows which had caused limitation of movements. Presently there were no medical reports available regarding it.
From his diet history, he appeared to be a heavy tea drinker, consumed around 8-10 glasses of tea per day. His main diet included bread and milk.
General physical examination revealed some skin lesions resembling keratotic patches on the temple of face, abdomen and back of neck. His palms too revealed small red dots resembling petechiae, for which he had not consulted any dermatologist [Figures 1a–d].
Figure 1a.

Keratotic patch on abdomen
Figure 1d.

Palms showing small petechiae
Figure 1b.

Hyperkeratotic patch at back of neck
Figure 1c.
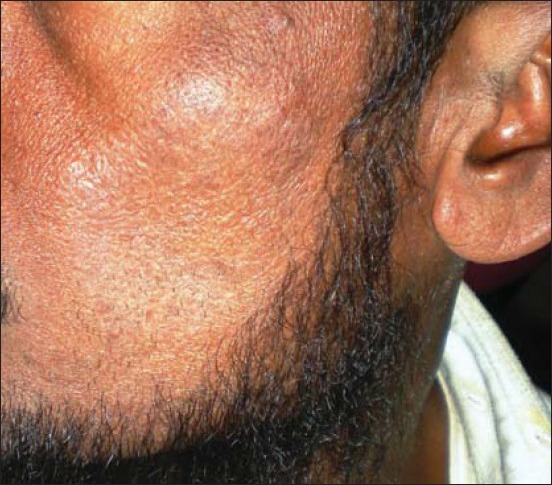
Keratotic patch on cheek region
Clinical examination of the periodontium revealed generalized intense dark red colored, painful gingiva with severe inflammation, involving mainly interdental papilla and the margins extending up to mucogingival junction. The gingiva appeared shiny bulbous with soft and spongy consistency [Figures 2a and b]. There appeared whitish pseudo membranous slough over the cervical and interdental regions, revealing either poor oral hygiene or negligence. There appeared spontaneous bleeding on slightest provocation which persisted for few minutes (3-5 min). With these presenting features, a provisional diagnosis of necrotizing ulcerative gingivitis was thought of until there happened to appear a blackish discoloration at the provocated sites [Figure 2c]. This observation stopped us from further detailed periodontal examination. The patient was advised for medical referral with complete blood examination and an orthopantomogram (OPG). The hemogram report, showed all the clinical parameters to be within normal limits except for platelet count which was 80,000/cu mm. After obtaining consent from the physician, a gingival biopsy was planned.
Figure 2a.

Clinical picture showing frontal view at initial visit
Figure 2b.

Clinical view of left side at first visit
Figure 2c.

Clinical picture showing blackish discoloration at the provocated sight
The next day, under the cover of antibiotics, anti inflammatory and vitamin C supplements, (Antibiotics - Amoxicillin 500 mg, Metronidazole 400 mg, and anti-inflammatory Ibuprofen-400 mg for five days, along with vitamin C supplements-250 mg q.i.d for 2 weeks) slow and gentle removal of necrotic slough with cotton swabs soaked in 3% hydrogen peroxide solution, was carried out, after application of topical anesthesia [Figure 3]. This was followed by irrigation with solution containing povidone and iodine. The superficial accretions were slowly removed with curettes without hurting the gingiva. An incisional biopsy was taken under local anesthesia. Further, a venous blood sample was drawn and sent to the laboratory to detect the neutrophil function. The patient was discharged with the advice of adequate rest and inclusion of a variety of nutritional supplements in his diet.
Figure 3.

Gentle removal of slough with cotton pellet swabbed with hydrogen peroxide 3%
Meanwhile, histopathological examination of the biopsy specimen confirmed it to be a case of scorbutic gingivitis. It showed presence of intra-epidermal vesicles and spongiosis in the squamous epithelium. The superficial areas of squamous epithelium show koilocytic change. The deeper connective tissue revealed marked vascularity and acute or chronic inflammatory exudates. Few of the areas also revealed subepithelial hemorrhages and capillaries revealed fibrin thrombi [Figures 4a and b].
Figure 4a.
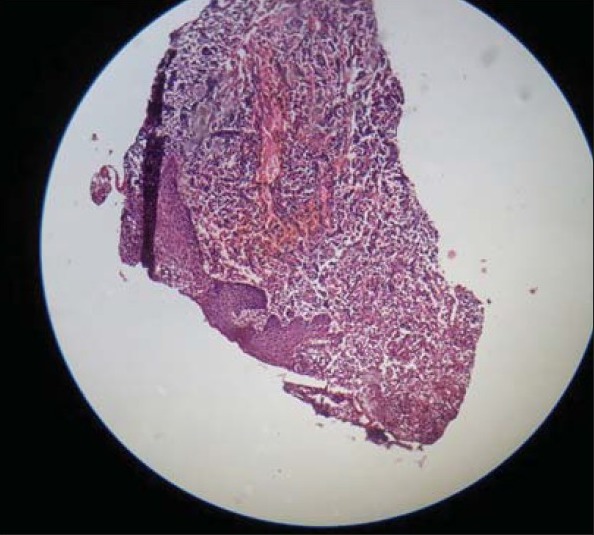
Histopath picture showing hemorrhage
Figure 4b.
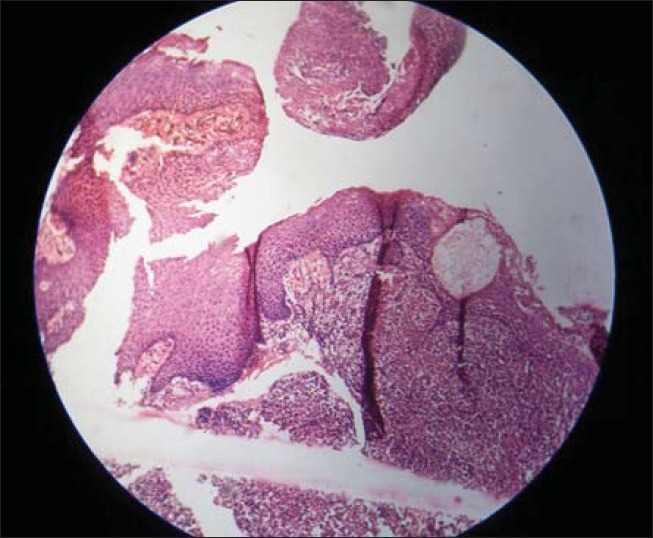
Histopathological section showing spongiosis
A confirmed diagnosis of scorbutic siderosis of gingiva was made based on the collected information regarding clinical, histopathological, and medical examination.
Meanwhile the neutrophil defect assay showed reduced chemotaxis and reduced phagocytosis activity. Phagocytic activity was depicted by reduced mean particle number of ingested Candida (Most probable number (MPN)-3). Neutrophil chemotaxis response towards N-formyl-methionyl-leucyl-phenylalanine was −1.1 mm in the present case. The values for the respiratory burst activity and intracellular killing activity by NBT (Nitroblue Tetrazolium) assay and candid cidal assay were within normal limits [Table 1].
Table 1.
Neutrophil defect assay of the patient showing reduced phagocytosis and defective chemotaxis

After 1 week, the patient returned and there was marked improvement at the site of the gingiva and at this time blood examination revealed the platelet count to be 1,30,000/cu.mm. Now a detailed periodontal examination was carried out, which revealed, grade three mobility with 31 and grade two mobility with 41. OPG revealed mild to moderate generalized bone loss [Figure 5]. The patient was advised for extraction of 31 for which he did not agree and insisted on retaining the teeth, therefore, a partial supragingival scaling was carried out. The patient was recalled after one week for subgingival scaling and root planning. At this time provisional splinting of the lower anterior teeth was carried out. The patient was counseled for proper oral hygiene maintenance and the importance of inclusion of fruits and vegetables in his diet were once again stressed. The clinical picture of the gingiva at the end of 2 weeks [Figures 6a and b].
Figure 5.

OPG showing mild to moderate generalized bone loss
Figure 6a.

Frontal view after 1 week
Figure 6b.

Clinical picture after 1 week post treatment
The patient returned after 3 months and there was remarkable improvement at the site of gingiva [Figures 7a and b]. Bleeding on probing was minimal with no discoloration at the provocated site. Meanwhile the skin disorder was diagnosed as hyperkeratosis with ringworm infection (Tinea corporis), by the dermatologist and was advised vitamin C supplements, topical application of a steroid ointment and an antifungal cream. The patient is being followed up regularly for 1 year with no recurrence of the lesion so far.
Figure 7a.

Post treatment view of left side after 3 months
Figure 7b.

Post treatment view of right side after 3 months
DISCUSSION
Causes of ascorbic acid deficiency are well documented throughout history. Scurvy, a rare condition, is said to occur especially in elderly people, alcoholics, smokers, and drug addicts. Most often, it is seen in warm and dry regions where there is lack of fresh fruit and vegetables. Socially and financially compromised people who survive on tea supplemented with toast or biscuits often develop scurvy.[3] In the present case, our patient was a non smoker and non alcoholic adult, farmer by occupation working for 10-12 hours per day. He was a heavy tea drinker and had poor dietary choice that consisted of mainly bread and milk.
There is evidence in the recent medical literature, as many scurvy cases were first misdiagnosed and mistreated before the root of the problem was discovered and treated.[2] In the present case, initially a dilemma existed regarding diagnosis based on clinical picture between necrotizing ulcerative gingivitis and scurvy. Both the entities present with features as necrosis, ulceration, spontaneous bleeding on provocation, severe fetor ex ore, severe pain, and presence of pseudo membranous slough.
The differential diagnosis of scurvy is broad and includes hematological abnormalities, medication side effects, infections, ulcerative gingivitis, collagen vascular disorder, deep venous thrombosis, vitamin deficiencies, trauma to legs and joints.[8] Ascorbic acid deficiency has also been implicated in the etiology of acute necrotizing ulcerative gingivitis. There is evidence that an increase in the gingival sulcal epithelial permeability and an impairment of polymorpho-nuclear leukocytes function precedes the appearance of periodontal lesions in ascorbate deficient animal.[9] In the present case, neutrophil defect detecting assay were carried out which showed defects in chemotaxis and reduced phagocytic activity of the neutrophils thus supporting this view [Table 1].
Etiology of low platelet count/thrombocytopenia include platelet destruction (immunologic, nonimmunologic causes) and decreased production which include abnormal marrow, hereditary disorders and vitamin deficiencies-folic acid and Vitamin B12 deficiency.[10]
A study by Wilson, et al., reported that reduced platelet adhesiveness in two patients with scurvy was rapidly corrected by administration of ascorbic acid and suggested that defect in platelet adhesiveness may be a factor in the poorly understood hemostaic defect in human scurvy.[11]
According to Johnson, et al., many studies have implicated quantitative and qualitative platelet abnormalities in scorbutic bleeding. In order to assess whether mucocutaneous hemorrhage occurring in scurvy was due to impaired platelet function, he carried out a study on platelet function and experimental human vitamin C deficiency and concluded that the abnormal platelet function in scurvy is probably not the result of vitamin C deficiency per se, but may be the consequence of co-existing nutritional deficiency.[12]
In the present case, the platelet count before the administration of medication and treatment was 80,000/cu.mm and rose to was 1,30,000/cu.mm after administration of medication and treatment. The low platelet count could be related also to the other nutritional deficiencies along with vitamin C deficiency and their repletion must be related to the correction of dietary habits of the patient by intake of nutritional supplements. This aspect needs to be further elicited as most of the case reports show normal count of platelets.[13]
Scurvy presents with severe pain thus limiting the functional activity of the oral cavity. Initially anti-inflammatory drugs were administered two hours prior to the procedure for the relief of pain. Later gentle removal of necrotic slough with cotton swabs soaked in 3% hydrogen peroxide was carried out. Hydrogen peroxide was used as it is still the medication of choice to clean necrotic areas due the effect of released oxygen on the anaerobic bacteria.
Presence of skin manifestations such as perifollicular hemorrhages, ecchymoses, petechiae, xerosis, bent coiled body hairs, in scurvy have been documented in many reports.[2,8] In the present study, the patient demonstrated with dry skin, (xerosis on back of neck, side of face and on abdomen) coiled hair, petechiae on palms.
It's now well accepted that scurvy is for e.g., not a first symptom of compromised ascorbic acid status but rather represents the end result of a series of adverse biological events. The role of vitamin C in protecting the tissues of the periodontium is well established as this nutrient has a role in both as an antioxidant and is important for optimum immune function.[1] Assessment of vitamin status is said to be not very easy. Plasma vitamins concentration are often used, but their diagnostic values are questionable since they are said to be influenced by many factors such as infections, inflammation and exercise, and may not reflect true deficiencies.[1] Methods available to assess vitamin C status include dietary history and measurement of vitamin C levels in serum, leukocytes, and urine.[6] Plasma vitamin C concentration < 11 mmol/L (0.2 mg/dL.) is said to be indicative of scurvy.[2] In the present case, dietary history, and polymorphonuclear defect assay helped in assessment of vitamin C. Plasma vitamin C assessment was not carried out.
RDA of Vitamin C range from 60 mg/day to 100 mg/day, of which 80-90% is absorbed and will make adequate body pool for males and females from age 15 to 60. Consuming five servings of fruits and vegetables/day is said to not only exceed RDA (Recommended Dietary Allowance) for vitamin C but also treat many vitamin deficiencies that occur in conjunction with scurvy.
In India, most of the rural families mainly rely on cereal based monotonous diet which supply only 20-90% of RDA. Therefore, vitamin deficiencies are more frequently encountered. According to a recent study based on Indian population, vitamin C deficiency was found in a substantial proportion of the older population.[14]
CONCLUSION
Lower dietary vitamin C intake could be a reflection of different lifestyles and personalities. It is said that scurvy is rare and only occurs in the event of imbalanced diet with nutritional deficiency. It needs to be differentiated from other conditions. A comprehensive medical, diet, and histopathological examination will aid in formulating a proper diagnosis and treatment.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Enwonwu CO. Vitamin supplements and oral health. In: Wilson M, editor. Food constituents and oral health. 1st ed. New Delhi: Woodhead Publishing India Private Limited; 2009. p. 302. [Google Scholar]
- 2.Schlueter AK, Johnston CS. Vitamin C: Overview and update. J Evidence-Based Complement Altern Med. 2011;16:49–57. [Google Scholar]
- 3.Touyz LZ. Vitamin C, oral scurvy and periodontal disease. S Afr Med J. 1984;65:838–42. [PubMed] [Google Scholar]
- 4.Ramakrishnan S, Prasannan KG, Rajan R. Textbook of Medical Biochemistry. 2nd ed. Madras: Orient Longman Limited; 1989. Vitamins; p. 356. [Google Scholar]
- 5.Padayatty SJ, Doppman JL, Chang R, Wang Y, Gill J, Papanicolaou DA, et al. Human adrenal glands secrete vitamin C in response to adrenocorticotrophic hormone. Am J Clin Nutr. 2007;86:145–9. doi: 10.1093/ajcn/86.1.145. [DOI] [PubMed] [Google Scholar]
- 6.Gaby AR. Vitamin C. In: Alan R Gaby., editor. Nutritional Medicine. A Text book. Concord, New Hampshire: Fritz Perlberg Publishing; 2010. pp. 99–108. [Google Scholar]
- 7.Nishida M, Grossi SG, Dunford RG, Ho AW, Trevisan M, Genco RJ. Dietary vitamin C and the risk for periodontal disease. J Periodontol. 2000;71:1215–23. doi: 10.1902/jop.2000.71.8.1215. [DOI] [PubMed] [Google Scholar]
- 8.Allgaier RL, Vallabh K, Lahri S. Scurvy: A difficult diagnosis with a simple cure. Afr J Emerg Med. 2012;2:20–3. [Google Scholar]
- 9.Murayama Y, Kurihara H, Nagai A, Dompkowski D, Van Dyke. Acute necrotizing ulcerative gingivitis: Risk factors involving host defense mechanisms. Periodontology 2000. 1994;6:116–124. doi: 10.1111/j.1600-0757.1994.tb00031.x. [DOI] [PubMed] [Google Scholar]
- 10.Ferri FF. Practical guide to the care of the medical patient. 8th ed. New Delhi: Elsevier Publications; 2011. Diseases and disorders; p. 536. [Google Scholar]
- 11.Wilson PA, Mchicolle GP, Doughlas AS. Platelet abnormality in human scurvy. Lancet. 1967;289:975–98. [PubMed] [Google Scholar]
- 12.Johnson GJ, Hollowway DE, Hutton SW, Duane WC. Platelet function and experimental human vitamin C deficiency. Thrombosis Res. 1981;24:85–93. doi: 10.1016/0049-3848(81)90034-7. [DOI] [PubMed] [Google Scholar]
- 13.Dolberg OJ, Elis A, Lischner M. Scurvy in the 21st century. IMAJ. 2010;12:183–4. [PubMed] [Google Scholar]
- 14.Ravindran RD, Vashist P, Gupta SK, Young IS, Maraini G, Camparini M, et al. Prevalence and risk factors for vitamin C deficiency in north and south India: A two centre population based study in people aged 60 years and over. PLoS ONE. 2011;6:e28588. doi: 10.1371/journal.pone.0028588. [DOI] [PMC free article] [PubMed] [Google Scholar]