

Abstract
Objective
Ex vivo HIV-1 challenge has been proposed as a bio-indicator of microbicide product effectiveness. The objective of this study was to establish optimal parameters for use of female genital tract tissue in this model.
Design
Ex vivo challenge involves in vivo product use, followed by tissue biopsy, and exposure of the tissue to HIV-1 in the laboratory.
Methods
Paired ectocervical and vaginal biopsies were collected from 42 women and 28 had additional biopsies from each site collected after 5% lidocaine (n=14) or chlorhexidine (n=14) treatment. Tissues were transported immediately to the laboratory and exposed to HIV-1. HIV-1 infection was followed by p24 ELISA on culture supernatants and at study end after weighing and fixing the tissue for immunohistochemistry (IHC) to detect p24 expressing cells.
Results
While both tissue types were equally infected with HIV-1 based on IHC results, ectocervical tissues had significantly higher HIV-1 replication than vaginal tissues (P < .005). Lidocaine and chlorhexidine had minimal impact on HIV-1 infection and replication. Point estimates for p24 levels were defined for 95% probability of p24-positive tissues and were 3.43 log10 for ectocervical tissue and 2.50 log10 for vaginal tissue based on weight-adjusted cumulative p24 endpoints.
Conclusions
While similar proportions of ectocervical and vaginal tissues support HIV-1 infection, higher levels of HIV-1 replication were observed in ectocervical tissues. Defining point estimates for HIV-1 infection in fresh ectocervical and vaginal tissues provides valuable information for the evaluation of HIV-1 preventative treatments during early clinical studies.
Keywords: Microbicides, pre-exposure prophylaxis, HIV prevention, explants, mucosal tissue susceptibility, bio-indicator
INTRODUCTION
Microbicides are products intended to be applied to the vaginal or rectal mucosa to prevent the sexual transmission of HIV-1 and potentially other sexually transmitted pathogens. One of the greatest challenges in assessing the suitability of an active agent for use as a microbicide is the lack of surrogate markers of efficacy. In HIV-1 treatment, one of the early achievements was changes in patient viral load proved to be a surrogate for the patient’s clinical response to antiretroviral treatment. However, in HIV-1 prevention research, there have been no recognized surrogates of efficacy which are relevant for clinical trial outcomes. Preclinical laboratory assays and animal models used to evaluate products for activity against HIV-1 have been poor predictors of effectiveness in HIV prevention trials. Both ectocervical and colorectal tissues obtained from surgical specimens have been used to evaluate the impact of drugs in tissues for preclinical drug testing [1–4]. The tissue is exposed to drug and HIV-1 in the laboratory to follow HIV-1 infection, or lack thereof, as an indicator of treatment efficacy. These explant models rely on human tissue which retain the architecture and relevant immune cells and thus provide a model which closely resembles intact female genital tract and colonic tissues.
The explant model was further developed by Anton and his colleagues during their phase 1 studies where vaginal microbicides were applied rectally prior to sampling colonic tissue by endoscopy [5, 6]. After product use, the biopsy tissue was then challenged with HIV-1 in the laboratory. This model was termed “ex vivo challenge”. The ex vivo challenge model is considered to be one of the closest surrogates to in vivo infection. Therefore, it is a potential bio-indicator of microbicide product effectiveness. The participants in these studies used UC781-containing, tenofovir-containing, or placebo gels daily for up to 1 week. At the end of the week, colonic biopsies were taken and the ones designated for ex vivo challenge were brought to the laboratory and exposed to HIV-1. Colonic tissue taken from the 2.5% UC781 and 1% tenofovir gel participants showed a significant reduction in HIV-1 p24 release compared to the colonic tissue taken from the placebo gel participants. These encouraging results with colonic tissues are tempered by the high levels of inter- and intra-subject variability in HIV-1 replication [7]. Increasing the reliability of the ex vivo challenge model will provide better predictions of clinical trial outcomes. To do this, evaluating the effects of assay methods and biopsy collection techniques on variability in tissue infection is needed. First, the capacity of HIV-1 to replicate in ectocervical versus vaginal tissue is unknown. Because the vagina has a greater surface area than the ectocervix, some investigators recommended using only vaginal tissue biopsies, while others suggested that the greater numbers of CD4+ immune cells in the ectocervix would make it a better choice. Secondly, the impact of female genital tract pre-procedure preparation which includes biopsy site disinfection and the application of topical anesthetic needs to be evaluated. It is unknown if either procedure would have an impact on HIV-1 infection of tissue. The effects of biopsy location (vaginal or ectocervical) and pre-procedure topical anesthesia (lidocaine) and disinfectant (chlorhexidine) on ex vivo biopsy infection were tested on both weight adjusted and non-weight adjusted viral replication as measured by p24 in culture supernatant and viral infection as measured by p24 immunohistochemistry (IHC). The goal of the present study was to define the optimal tissue and collection procedures for use of female genital tract tissue in the ex vivo challenge assay for future incorporation into early clinical trials.
METHODS
Reagents
Unless otherwise indicated, tissue culture base medium was purchased from Mediatech, Inc., Manassas VA; supplements were purchased from Gemini Bio-products, West Sacramento, CA or Lonza, Walkersville, MD; and IL-2 was purchased from Roche, Indianapolis, IN. The optimal challenge dose of HIV-1 may vary with virus strain and the laboratory growing the virus and determining the viral titer. The challenge virus should be empirically determined before using in a clinical study. For the current work, concentrated HIV-1BaL was purchased from Advanced Biotechnologies Inc., Columbia, MD. Dilutions of HIV-1BaL were made in RPMI-1640 and stored at −80°C. Tissue culture infectious dose 50% (TCID50) was determined by the Reed and Muench method for phytohemagglutinin-activated PBMCs [8].
Mucosal tissue collection
Paired ectocervical and vaginal tissue biopsies were collected from healthy women who consented to the procedure (University of Pittsburgh IRB PRO10110377). Forty two women had paired ectocervical and vaginal tissue biopsies collected. Of these, 28 women total, 14 women per group, had two additional biopsies from each site collected without 5% lidocaine or chlorhexidine treatment. For women who underwent four biopsies with and without a topical preparation, after insertion of the speculum, attention was turned to the right vaginal wall. A tischler biopsy instrument was positioned over a fold of vaginal tissue in the proximal vagina and a full thickness biopsy was collected. The tischler instrument was then positioned at the external os with one arm resting in the os, and a biopsy was obtained. The topical preparation was then applied to the left vaginal wall and cervical face and the second set of vaginal and cervical biopsies were obtained. Silver nitrate was applied to the vaginal biopsy sites and Monsels was applied to the cervical biopsy sites for hemostatis. The tissue was placed in a conical tube with transport medium (L-15 medium supplemented with 10% FBS, 100 μg/ml streptomycin, 100 U/ml penicillin, 100 mM L-glutamine, and 2.5 μg/ml Amphotericin B), placed on wet ice, and brought to the laboratory within 30 minutes of collection.
Ex vivo challenge assay
Tissues were placed into individual wells of a 48-well plate with 1 ml complete medium (DMEM supplemented with 10% human AB serum, 100 μg/ml streptomycin, 100 U/ml penicillin, 100 mM L-glutamine, 1% non-essential amino acids, and 100 U/ml IL-2) with 5×104 TCID50 HIV-1BaL and cultured in a humidified incubator at 37°C, 5% CO2. After 2 hours, the tissue was washed by passing through four changes of HBSS without calcium/magnesium, and then placed in a new well of a 48-well plate with 1 ml of fresh complete medium without HIV-1. Every 3 to 4 days of culture, 700 μl of medium was collected and saved at −80°C and fresh complete medium was replenished. Cultures were maintained for 21 days based on our work with ectocervical explants [2]. However, maintaining cultures through earlier time points, such as 14 days of culture, can also be done [4]. After 21 days of culture in this study, the tissue was weighed and placed in formalin to process for HIV-1 infected cells expressing p24 by IHC. The culture supernatant was evaluated for soluble HIV-1 p24 by ELISA (Perkin-Elmer Life Sciences, Inc., Boston, MA).
Statistical analysis
Weight-adjusted (pg/mg) and non-weight adjusted (pg/ml) p24 measurements were summed across test days 4 through 21 to provide cumulative p24 pg/mg and cumulative p24 pg/ml endpoints. The soft endpoint was calculated for weight-adjusted and non-weight adjusted p24 endpoints [9] and its calculation template is available at http://www.alphastatconsult.com/id3.html. Cumulative and soft p24 endpoints (pg/ml and pg/mg) were log10 transformed prior to analyses. IHC endpoints were provided for 36/42 ectocervical and 40/42 vaginal biopsy tissue. The weight was compared between paired ectocervical and vaginal tissue using the Wilcoxon matched-pairs signed rank test.
A randomized block design ANOVA (PROC MIXED) was used to compare the log transformed virus growth measurements for paired ectocervical vs. vaginal biopsy challenge results, and at each biopsy location, both with and without either lidocaine or chlorhexidine. Demographic and behavioral measures were included as covariates, i.e. binary behavioral measurements of age, smoking, hormonal oral contraceptive pill (OCP) use, condom use, intra-uterine devise use, and sexual activity were provided. IHC rates were compared by a 2×2 Fisher Exact test between ectocervical vs. vaginal biopsies, and for each biopsy type, ± lidocaine and ± chlorhexidine. Inter-correlations between biopsy endpoints were performed using Pearson and logistical analyses. An alpha value of 0.05 and SAS® (version 9.3; Cary, NC) was used for all analyses.
RESULTS
Study population and tolerability of the biopsy procedures
The population characteristics of the 42 volunteers who participated in the study and provided tissues are shown in Table 1. The study participants were predominately white and the median age was 29 years (range 21 to 45 years). Fewer than 10% were current smokers and the majority of women were using some form of birth control. None of the women used Depo-Provera or had a tubal ligation. Women reported that both vaginal and ectocervical biopsies were well-tolerated. For the 14 study participants who had four biopsy samples obtained with and without lidocaine, no difference in perception between the sampling procedures was noted. Thus, there was no difference in the patient acceptability of biopsy with or without anesthetic.
Table 1.
Study participant demographics and behavior measurements.
| Demographics/behavior | N | Percent |
|---|---|---|
| Race | ||
| White | 37 | 88% |
| Black | 2 | 4.8% |
| Asian | 2 | 4.8% |
| Other | 1 | 2.4% |
|
| ||
| Behavior | ||
| Current smoker | 4 | 9.5% |
| Oral contraceptive pills | 8 | 19% |
| IUD | 24 | 57% |
| Condoms* | 6 | 14% |
| Rhythm/withdrawal | 2 | 5% |
| Not sexually active with a man | 3 | 7% |
Condoms were used in conjunction with other contraceptive options.
HIV-1 infection of ectocervical and vaginal tissue
To address whether ectocervical and vaginal tissue are infected and have a similar capacity to replicate HIV-1, paired tissues from 42 participants were obtained. One participant’s tissue became contaminated during the culture period; therefore, paired tissue from 41 participants was evaluated. Because of variable tissue sizes obtained by biopsy, the p24 results were analyzed without and with correction of tissue weight at study end. The end of the 21 day culture period was chosen because mucus is often attached to the tissue at time of collection and additional manipulation was not desired at the beginning of the study. The median tissue weights were significantly different (P < .001) between ectocervical (median, 8.68 mg; range, 0 – 36.59) and vaginal (13.29; 0 – 123.56). Overall, replication of HIV-1 in ectocervical tissue was significantly higher (P < .005) than in vaginal tissue as measured by p24 release into the culture supernatant (Fig. 1a; Table 2). Weight and non-weight adjusted p24 endpoints were highly correlated (P < .0001) for the cumulative (Fig. 2a) and soft (Fig. 2b) endpoint p24 analyses. However, the weight and non-weight adjusted endpoints showed more variability at the lower p24 levels for vaginal tissue as evidenced by the increased scatter of the red data points. None of the covariate factors were found to influence HIV-1 replication for either tissue type.
Fig. 1.

HIV-1 replication and infection of fresh ectocervical and vaginal tissue. Paired ectocervical and vaginal tissue was collected from 42 participants. The tissue was exposed to HIV-1, wash, and cultured for 21 days. Supernatant was collected and replenished every 3 to 4 days. (a) HIV-1 replication was monitored by p24gag ELISA in the culture supernatant. The p24 values were summed over day 4 through 21 and presented as the mean ± SD of 41 participants (one participant’s tissue was contaminated). The p24 values were from non-weight adjusted (upper panel) or weight adjusted (lower panel) p24 values. Embedded probability values for the paired comparison of cumulative p24 at day 21. Representative immunohistochemistry staining for p24 infected cells from cervical (b) and vaginal (c) tissue collected at study end is shown.
Table 2.
HIV-1 endpoints and treatment effects on HIV-1 p24 replication from paired ectocervical and vaginal tissue.
| Endpoint p24 measure (Log10) | Least square mean (SE)
|
Probability | |
|---|---|---|---|
| Ectocervical (N=41) | Vaginal (N=41) | ||
| Cumulative (pg/ml) | 4.1 (.34) | 3.63 (.34) | .0011 |
| Cumulative (pg/mg) | 3.14 (.42) | 2.4 (.42) | <.0001 |
| Soft (pg/ml) | 3.67 (.41) | 3.21 (.41) | .0049 |
| Soft (pg/mg) | 2.76 (.46) | 2 (.46) | <.0001 |
| Ectocervical tissue (N=14) | Chlorhexidine
|
||
|---|---|---|---|
| (−) | (+) | ||
| Cumulative (pg/ml) | 4.27 (.43) | 4.05 (.43) | ns |
| Cumulative (pg/mg) | 3.36 (.43) | 3.32 (.43) | ns |
| Soft (pg/ml) | 3.94 (.43) | 3.65 (.43) | ns |
| Soft (pg/mg) | 3.04 (.44) | 2.92 (.43) | ns |
|
| |||
| Lidocaine
|
|||
| (−) | (+) | ||
|
| |||
| Cumulative (pg/ml) | 4.63 (.65) | 4.14 (.65) | ns |
| Cumulative (pg/mg) | 3.71 (.76) | 3.32 (.76) | ns |
| Soft (pg/ml) | 4.12 (.71) | 3.63 (.71) | ns |
| Soft (pg/mg) | 3.22 (.83) | 2.89 (.84) | ns |
| Vaginal tissue (N=14) | Chlorhexidine
|
||
|---|---|---|---|
| (−) | (+) | ||
| Cumulative (pg/ml) | 3.93 (.22) | 4.18 (.22) | ns |
| Cumulative (pg/mg) | 2.67 (.24) | 3.11 (.24) | .0058 |
| Soft (pg/ml) | 3.6 (.24) | 3.75 (.24) | ns |
| Soft (pg/mg) | 2.33 (.24) | 2.7 (.24) | .0196 |
|
| |||
| Lidocaine
|
|||
| (−) | (+) | ||
|
| |||
| Cumulative (pg/ml) | 3.87 (.28) | 4.04 (.28) | ns |
| Cumulative (pg/mg) | 2.79 (.41) | 2.95 (.41) | ns |
| Soft (pg/ml) | 3.36 (.32) | 3.53 (.32) | ns |
| Soft (pg/mg) | 2.29 (.45) | 2.45 (.44) | ns |
SE, standard error; ns, not significant; −/+, without or with treatment prior to biopsy collection.
Weight-adjusted (pg/mg) and non-weight adjusted (pg/ml) p24 measurements were summed across test days 4 through 21 to provide cumulative p24 pg/mg and cumulative p24 pg/ml endpoints. The soft endpoint was calculated for weight-adjusted and non-weight adjusted p24 endpoints. Cumulative and soft p24 endpoints (pg/ml and pg/mg) were log10 transformed prior to analyses. A randomized block design ANOVA (PROC MIXED) was used to compare the log transformed virus growth measurements for paired ectocervical vs. vaginal biopsy challenge results, and at each biopsy location; ±lidocaine or ±chlorhexidine.
Fig. 2.
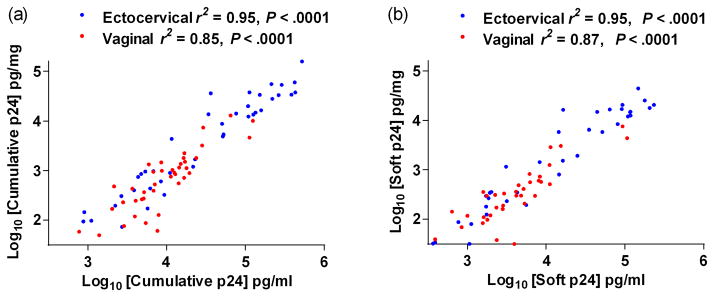
Correlation between weight and non-weight adjusted p24 endpoints. Correlation between p24 measures made per volume of supernatant (ml) and per volume of supernatant adjusted for weight of sample (mg) for (a) log10 cumulative p24 or (b) log10 soft p24 endpoints.
Detection of p24 expressing cells by IHC confirmed HIV-1 infection of the tissue. Ectocervical and vaginal tissue from 36 and 40 donors, respectively, was available at study end for IHC. No significant differences were found in IHC positive tissues; 31/36 (86%) ectocervical p24-positive (Fig. 1b) compared to 36/40 (90%) vaginal p24-positive (Fig. 1c) tissues (P = .7279).
Effect of chlorhexidine and lidocaine on HIV-1 infection
To determine whether application of disinfectant or anesthetic modified HIV-1 infection in tissue explants, a subset of women underwent additional procedures in addition to the initial two biopsies. Additional procedures included either cleaning the tissue with chlorhexidine prior to obtaining two additional biopsies (14 women), or numbing the tissue with 5% lidocaine gel prior to obtaining two additional biopsies (14 women). There was no significant effect of either procedure on HIV-1 p24 production in ectocervical tissue (Table 2). While lidocaine had no effect on HIV-1 p24 production in vaginal tissue, chlorhexidine-treated tissue showed a modest increase in HIV-1 p24 production when adjusted for tissue weight (P < .05; Table 2), but no effect on HIV-1 p24 production when not adjusted for tissue weight.
p24 endpoint correlations with IHC
To define a point estimate for HIV-1 infection of the tissue, both p24 endpoints were correlated to IHC p24-postive tissues. There were significant, positive relationships between ectocervical tissue and all p24 endpoint measurements (Fig. 3a and 3b; soft endpoint (P < .05) not shown). Vaginal tissue significantly correlated with the weight-adjusted p24 endpoint measurements (Fig. 3c; soft endpoint (P = .0359) not shown), but not the non-weight-adjusted p24 endpoint measurements (Fig. 3d; soft endpoint (P = ns) not shown). To estimate the p24 endpoints that provide a 95% probability of an IHC p24-positive tissue, logistic regression point estimates were interpolated. The p24 logistic regression point estimates for ectocervical tissue were determined to be 3.43 and 2.98 log10 (pg/mg of tissue) for cumulative p24 and soft p24 endpoints, respectively. Ectocervical p24 levels were approximately 1 log10 higher than vaginal tissue, which were determined to be 2.5 and 1.96 log10 (pg/mg of tissue) for cumulative p24 and soft p24 endpoints, respectively. Overall, the cumulative p24 was approximately 0.5 log10 higher than the soft p24 endpoints in both tissues.
Fig. 3.

Correlation between immunohistochemistry and cumulative p24 endpoints. Logistic regression curves where circles represent immunohistochemistry score of 1 = positive and 0 = negative on the y-axis and cumulative p24 endpoint on the x-axis for ectocervical tissue (a) weight adjusted and (b) non-weight adjusted and vaginal tissue (c) weight adjusted and (d) non-weight adjusted. The probability of a positive immunohistochemistry result is predicted for each p24 result with a logistic regression curve shown as a black solid line where the shaded area represents the upper and lower 95% confidence limits of the curve.
DISCUSSION
This study has demonstrated that freshly obtained tissue biopsy samples from the female genital tract were consistently infected with HIV-1 and so this model can be used as tissue explants to assess susceptibility to HIV-1 when challenged “ex vivo”. The ex vivo challenge assay was used to test vaginal topical microbicide candidates after rectal application [5, 6]. The initial study collected colonic tissue located 10 cm and 30 cm from the anal verge to define HIV-1 infection and replication which were similar at both anatomic sites [6]. The translation of this assay to female genital tract tissue required that vaginal and cervical tissue be evaluated for their capacity to be infected and replicate HIV-1. While both ectocervical and vaginal tissue were infected with HIV-1 at a similar frequency, ectocervical tissue replicated HIV-1 to ~1 log10 higher levels. As compared to the colonic tissue, female genital tract tissue responds to HIV-1 infection differently as seen by vaginal tissue having modest p24 levels. Moreover, pre-procedure preparation of the two mucosal tracts is quite different. Before collection of colonic tissue, the participant is asked to fast the night before and then the next morning the lumen is rinsed with an isotonic enema to remove any solid material that may remain. Before collection of female genital tract tissue, women commonly have the vaginal vault “washed” with an antiseptic solution and may have the biopsy site numbed with a topical anesthetic. Topical antiseptic solutions often contain chlorhexidine which is a potent antibacterial compound and is known to inactivate HIV-1 and HSV [10]. Because the immune and nervous systems communicate with each other, anesthetics are known to dampen the immune response [11]. Collectively, these procedures could impact the ex vivo challenge assay by interfering with HIV-1 infection of the tissue. Chlorhexidine and lidocaine pre-treatments showed no overall significant impact on HIV-1 infection or replication in ectocervical or vaginal tissue. However, chlorhexidine pretreatment had a modest increase in HIV-1 replication in vaginal tissue when adjusted for tissue weight. As the collection of tissue without these extraneous procedures was tolerated by the 42 women in this study, it is suggested that chlorhexidine and lidocaine treatments are not performed prior to tissue collection for the ex vivo challenge assay.
Despite using the same sized tischler forceps to collect the ectocervical and vaginal tissue, there was significant variability in the size of the biopsies likely due to varying thickness of the vaginal folds. Because mucus is often collected along with the biopsy and additional manipulations through washing were not desired, biopsies were weighed at study end (day 21) of culture when mucus would have dissipated. Ectocervical tissue had a significantly lower weight than vaginal tissue. Three biopsies, two ectocervical and one vaginal, had no discernible tissue at study end. Regardless of the variability in the tissue weight, the cumulative and soft p24s were highly correlated for non-weight and weight adjusted endpoints with the ectocervical tissue producing ~1 log10 more HIV-1 p24 than the vaginal tissue. While immune cells populate the lower genital tract, the cervix has more immune cells, specifically CD4+ T cells, than the vagina and the cell populations do not appear to be influenced through the menstrual cycle [12, 13]. While no systematic study has been done to compare immune cell activation between the ectocervix and vagina, the CD4+ T cell subpopulations in the cervix expressing α4β7 (mucosal homing receptor) also express higher levels of CCR5 and CD69 [14]. Although we were not able to define the immune cell populations and their activation status in this study due to the limited number of biopsies collected, the published data would support our results showing similar infection rates between ectocervical and vaginal tissue, but greater HIV-1 replication occurring in the ectocervical tissue due to more activated immune targets. Adjusting for the weight of the tissue may be beneficial, especially for vaginal tissue, as the p24 endpoint correlations to p24-positive tissue significantly correlated when weight-adjusted. To note, the two studies [5, 6] using colonic tissue for the ex vivo challenge assay did not weight-adjust their p24 results. The colon has the largest numbers of immune cells in the body and most of those cells are activated [15] so weight-adjustment may not be as critical for interpretation, similar to the ectocervical results reported here. A limitation of the work presented was not collecting the tissue weight before placing it in culture. While our intent was to eliminate washing steps which would exclude mucus from the tissue, pre- and post-culture weighing may be warranted to accurately define the impact tissue weight has on HIV-1 replication. Nonetheless, these results show the utility of both ectocervical and vaginal tissue types for the ex vivo challenge assay.
The use of female genital tract tissues presents additional challenges compared to colonic tissues due to the number of female genital tract tissue biopsies that can feasibly be collected. Because the colon has a large surface area, taking up to 20 biopsies is typical, whereas the numbers of biopsy samples which can be obtained at a single time point for female genital tract samples is four: two vaginal and two ectocervical. This limits the within subject sampling across the genital tract for any clinical trial evaluating an HIV-1 preventative. Tissue is usually required for immune cell distribution and numbers, biomarkers such as gene arrays, drug levels (pharmacokinetics), in addition to drug protection (pharmacodynamics) so prioritization of tissue usage should be made early in the study to maximize tissue use. Additionally, healing of the biopsy area may take up to 10 days, so frequent tissue collection is limited and restricted for ethical reasons. A recent study demonstrated that taking multiple colonic biopsies did not increase uptake of radioactive small molecules – similar in size to HIV-1 particles [16]. This type of study should be conducted for the female genital tract after collection of vaginal/ectocervical biopsies to ensure epithelial trauma does not influence the normal homeostasis of the genital tract. As discussed above, there are differences in immune cell distribution through the genital tract. While the cell numbers do not appear to vary over the menstrual cycle, exogenous hormones from contraceptive use has been shown to increase activated CD4+/CCR5+ cells in the vagina [17]. In nonhuman primates, the use of progestin was shown to reduce the vaginal epithelial thickness and increase SIV susceptibility [18]. Indeed, depot medroxyprogesterone acetate injections in female macaques are done to aid in the transmission of SIV in experiments testing the effectiveness of vaccines and microbicides. While there has been some indication the use of hormonal contraception may increase a women’s risk for HIV-1 infection [19], the use of hormonal contraception by women in this study did not influence the infection or replication of HIV-1. However, further work is needed to systematically define the role of hormonal contraceptives in HIV-1 infection of mucosal tissue. While additional preparatory procedures of the vaginal vault such as the use of chlorhexidine and lidocaine had no impact on HIV-1 infection, chlorhexidine modestly increased HIV-1 replication by vaginal tissue when adjusted for weight, but not ectocervical tissue. Chlorhexidine is a potent antibacterial compound with documented anti-viral activity [10] and is a common ingredient in mouthwashes and topically applied products. Chlorhexidine was shown to enhance HSV transmission and induce prolonged susceptibility to Chlamydia in mice [20, 21]. These additional preparatory procedures should be eliminated to allow for better interpretation of ex vivo challenge assay results from clinical studies using topical microbicide products.
While this bio-indicator model has shown promise evaluating some topical formulations rectally, the incorporation of the ex vivo challenge assay may not be useful in all early clinical trials. Proximity of the clinical site location to the laboratory performing the ex vivo challenge assay and the activity of the drug candidate being tested also must be considered. Currently, only fresh tissue has been used for this assay. The use of frozen tissue for HIV-1 infection has not yielded reproducible results. Cervical tissue appears to remain intact [22], but the capacity of HIV-1 to replicate in fresh compared to frozen tissue was not tested. Another study showed colorectal tissue quickly degrades after freeze/thawing procedures [23]. These studies suggest that the freezing and thawing process of tissue needs to be optimized and standardized before using frozen tissue for the ex vivo challenge assay. Moreover, the osmotic changes that occur to the cells in the tissue during freezing and thawing may compromise the drug levels in the tissue by inadvertently flushing the cells of drug [24]. Therefore, the drug candidate being tested also needs to be considered before using the ex vivo challenge assay. For example, luminally active drugs such as PRO 2000, Griffithsin, or monoclonal antibodies would not be expected to be effective at preventing HIV-1 infection of the tissue because the drug presumably would be removed during specimen collection and transport prior to HIV-1 exposure. Non-nucleoside reverse transcriptase inhibitors which have no cellular transporters and thus freely diffuse in and out of the cell could be partially or completely removed as well. Consequently, the use of the ex vivo challenge assay is limited to laboratories in close proximity to the clinical trial site and potentially to drugs that are active within the cell.
Fresh ectocervical and vaginal tissue from young, healthy women to be used for HIV-1 infection can be incorporated into early clinical trials to evaluate candidate drugs. Ectocervical tissue replicates HIV-1 ~1 log10 higher than vaginal tissue despite HIV-1 infecting the tissues equally. While the inclusion of preparatory procedures for tissue collection such as cleansing and numbing the genital tract vault had no to modest impact on HIV-1 infection and replication, the participants did tolerate the tissue collection without them. Thus, these preparatory procedures are not necessary and not including them would potentially reduce some of the variability that is inherent in the assay. We are now incorporating the ex vivo challenge assay into several clinical trials as a bio-indicator of the drug activity in the tissue after in vivo use.
Acknowledgments
Source of Funding: The work presented here was supported by the Film Antiretroviral Microbicide Evaluation (FAME) program which received funding from the NIH, Division of AIDS (U19 AI082639).
CSD, KB, and SLH planned the experiments. KB and IM recruited the participants and collected the tissue. KU performed the HIV-1 infection experiments. NRH performed the data analyses. CSD, KB, NRH, and SLH wrote the manuscript. The authors would like to thank the volunteers for their willingness to participate in research. The work presented here was supported by the Film Antiretroviral Microbicide Evaluation (FAME) program which received funding from the Division of AIDS, NIH (U19 AI082639). The work was also supported in part by a subcontract with Advanced BioScience Laboratories, Inc., Rockville, MD though a NIH/NIAID/DAIDS contract: Comprehensive Resources for HIV Microbicides and Biomedical Prevention (#HHSN272201000001C). This work was presented in part at the international Microbicides 2012 meeting in Sydney Australia, April 15 – 18 (Abstract #14)
Footnotes
Conflicts of Interest: All of the authors declare no conflicts of interest.
References
- 1.Abner SR, Guenthner PC, Guarner J, Hancock KA, Cummins JE, Jr, Fink A, et al. A human colorectal explant culture to evaluate topical microbicides for the prevention of HIV infection. J Infect Dis. 2005;192:1545–1556. doi: 10.1086/462424. [DOI] [PubMed] [Google Scholar]
- 2.Cummins JE, Jr, Guarner J, Flowers L, Guenthner PC, Bartlett J, Morken T, et al. Preclinical testing of candidate topical microbicides for anti-human immunodeficiency virus type 1 activity and tissue toxicity in a human cervical explant culture. Antimicrob Agents Chemother. 2007;51:1770–1779. doi: 10.1128/AAC.01129-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fletcher PS, Elliott J, Grivel JC, Margolis L, Anton P, McGowan I, et al. Ex vivo culture of human colorectal tissue for the evaluation of candidate microbicides. AIDS. 2006;20:1237–1245. doi: 10.1097/01.aids.0000232230.96134.80. [DOI] [PubMed] [Google Scholar]
- 4.Greenhead P, Hayes P, Watts PS, Laing KG, Griffin GE, Shattock RJ. Parameters of human immunodeficiency virus infection of human cervical tissue and inhibition by vaginal virucides. J Virol. 2000;74:5577–5586. doi: 10.1128/jvi.74.12.5577-5586.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Anton PA, Cranston RD, Kashuba A, Hendrix C, Bumpus NN, Richardson-Harman N, et al. RMP-02/MTN-006: A Phase 1 Rectal Safety, Acceptability, Pharmacokinetic and Pharmacodynamic Study of Tenofovir 1% Gel Compared to Oral Tenofovir Disoproxil Fumerate. AIDS Res Hum Retroviruses. 2012 doi: 10.1089/aid.2012.0262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Anton PA, Saunders T, Elliott J, Khanukhova E, Dennis R, Adler A, et al. First Phase 1 Double-Blind, Placebo-Controlled, Randomized Rectal Microbicide Trial Using UC781 Gel with a Novel Index of Ex Vivo Efficacy. PLoS ONE. 2011;6:e23243. doi: 10.1371/journal.pone.0023243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Richardson-Harman N, Mauck C, McGowan I, Anton P. Dose-Response Relationship Between Tissue Concentrations of UC781 and Explant Infectibility with HIV Type 1 in the RMP-01 Rectal Safety Study. AIDS Res Hum Retroviruses. 2012 doi: 10.1089/aid.2012.0073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reed LJ, Muench H. A simple method of estimating fifty per cent endpoints. Am J Hygiene. 1938;27:493–497. [Google Scholar]
- 9.Richardson-Harman N, Lackman-Smith C, Fletcher PS, Anton PA, Bremer JW, Dezzutti CS, et al. Multisite comparison of anti-human immunodeficiency virus microbicide activity in explant assays using a novel endpoint analysis. J Clin Microbiol. 2009;47:3530–3539. doi: 10.1128/JCM.00673-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Baqui AA, Kelley JI, Jabra-Rizk MA, Depaola LG, Falkler WA, Meiller TF. In vitro effect of oral antiseptics on human immunodeficiency virus-1 and herpes simplex virus type 1. J Clin Periodontol. 2001;28:610–616. doi: 10.1034/j.1600-051x.2001.028007610.x. [DOI] [PubMed] [Google Scholar]
- 11.Yu HP. Role of anesthetic agents on cardiac and immune systems. Shock. 2011;36:532–541. doi: 10.1097/SHK.0b013e3182357054. [DOI] [PubMed] [Google Scholar]
- 12.Pudney J, Quayle AJ, Anderson DJ. Immunological microenvironments in the human vagina and cervix: mediators of cellular immunity are concentrated in the cervical transformation zone. Biol Reprod. 2005;73:1253–1263. doi: 10.1095/biolreprod.105.043133. [DOI] [PubMed] [Google Scholar]
- 13.Ildgruben AK, Sjoberg IM, Hammarstrom ML. Influence of hormonal contraceptives on the immune cells and thickness of human vaginal epithelium. Obstet Gynecol. 2003;102:571–582. doi: 10.1016/s0029-7844(03)00618-5. [DOI] [PubMed] [Google Scholar]
- 14.McKinnon LR, Nyanga B, Chege D, Izulla P, Kimani M, Huibner S, et al. Characterization of a human cervical CD4+ T cell subset coexpressing multiple markers of HIV susceptibility. J Immunol. 2011;187:6032–6042. doi: 10.4049/jimmunol.1101836. [DOI] [PubMed] [Google Scholar]
- 15.Anton PA, Elliott J, Poles MA, McGowan IM, Matud J, Hultin LE, et al. Enhanced levels of functional HIV-1 co-receptors on human mucosal T cells demonstrated using intestinal biopsy tissue. AIDS. 2000;14:1761–1765. doi: 10.1097/00002030-200008180-00011. [DOI] [PubMed] [Google Scholar]
- 16.Fuchs EJ, Grohskopf LA, Lee LA, Hendrix CW. Microbicide 2008. New Delhi, India: 2008. Detecting Rectal Epithelial Disruption using Radioisotopes: A Simple Test to Identify Potential HIV Microbicide Toxicity; p. Abst #209. [Google Scholar]
- 17.Chandra N, Thurman AR, Anderson S, Cunningham TD, Yousefieh N, Mauck C, et al. Depot Medroxyprogesterone Acetate Increases Immune Cell Numbers and Activation Markers in Human Vaginal Mucosal Tissues. AIDS Res Hum Retroviruses. 2012 doi: 10.1089/aid.2012.0271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Marx PA, Spira AI, Gettie A, Dailey PJ, Veazey RS, Lackner AA, et al. Progesterone implants enhance SIV vaginal transmission and early virus load. Nat Med. 1996;2:1084–1089. doi: 10.1038/nm1096-1084. [DOI] [PubMed] [Google Scholar]
- 19.Heffron R, Donnell D, Rees H, Celum C, Mugo N, Were E, et al. Use of hormonal contraceptives and risk of HIV-1 transmission: a prospective cohort study. Lancet Infect Dis. 2011 doi: 10.1016/S1473-3099(11)70247-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cone RA, Hoen T, Wong X, Abusuwwa R, Anderson DJ, Moench TR. Vaginal microbicides: detecting toxicities in vivo that paradoxically increase pathogen transmission. BMC Infect Dis. 2006;6:90. doi: 10.1186/1471-2334-6-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Achilles SL, Shete PB, Whaley KJ, Moench TR, Cone RA. Microbicide efficacy and toxicity tests in a mouse model for vaginal transmission of Chlamydia trachomatis. Sex Transm Dis. 2002;29:655–664. doi: 10.1097/00007435-200211000-00007. [DOI] [PubMed] [Google Scholar]
- 22.Gupta P, Ratner D, Patterson BK, Kulka K, Rohan LC, Parniak MA, et al. Use of Frozen-Thawed Cervical Tissues in the Organ Culture System to Measure Anti-HIV Activities of Candidate Microbicides. AIDS Res Hum Retroviruses. 2006;22:419–424. doi: 10.1089/aid.2006.22.419. [DOI] [PubMed] [Google Scholar]
- 23.McGowan I, Tanner K, Elliott J, Ibarrondo J, Khanukhova E, McDonald C, et al. Nonreproducibility of “Snap-Frozen” Rectal Biopsies for Later Use in Ex Vivo Explant Infectibility Studies. AIDS Res Hum Retroviruses. 2012 doi: 10.1089/aid.2012.0062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mazur P. Freezing of living cells: mechanisms and implications. Am J Physiol. 1984;247:C125–142. doi: 10.1152/ajpcell.1984.247.3.C125. [DOI] [PubMed] [Google Scholar]