

Abstract
The purpose of this study was to describe psychological effects and exercise adherence during a multicomponent exercise training intervention. A sample of 42 patients with heart failure (HF) were randomized into an exercise (INV) group, (n=22) and an attention control (AC) group (n=20). The exercise protocol included two 12-week phases, a structured phase and a self-managed phase. The psychological responses assessed were mood states and exercise self-efficacy. To meet the second purpose of the study, the exercise group was dichotomized based on the number of sessions completed to create two adherence subgroups. Results indicate self-efficacy improved for the INV group and was maintained during the self-management phase. The adherence subgroups demonstrated different patterns for weekly exercise. Depression and confusion scores improved for the high adherence group in contrast to worsening for the low adherence group. Results suggest the need for further study of the psychological responses of exercise adherence for patients with HF.
Keywords: Heart failure, exercise, frequency, psychological, adherence
Little is known about the psychology of exercise adherence in heart failure (HF). It has been reported that exercise can improve emotional moods in HF but the relationship of exercise adherence to psychological outcomes remains unclear (Karapolat et al., 2009). Understanding the psychological responses and the process of adherence would help in the design of exercise programs that are both beneficial and sustainable by patients with HF. The purpose of this study was to examine psychological responses to exercise and to explore the relationship between adherence and changes in psychological responses during two, 12-week phases of an exercise intervention for patients with HF.
Background
Results from the multi-site, 5-year exercise trial HF-ACTION demonstrated that adherence does impact the efficacy of exercise (Flynn et al., 2009). Patients with HF report that adhering to exercise is more difficult than other HF treatment recommendations including diet, medication, and smoking cessation (Evangelista, Berg, & Dracup, 2001). Several psychological factors contribute to patients’ difficulty with exercise. Reports indicate 63% of patients experience anxiety and nearly 20% are clinically depressed (Haworth et al., 2005; Rutledge, Reis, Linke, Greenberg, & Mills, 2006). These conditions can decrease interest in and motivation to exercise. The physiological effects of exercise can also impact psychological responses. During exercise, commonly reported HF symptoms such as dyspnea and fatigue are experienced which can increase feelings of fear, anxiety, and powerlessness. These feelings can erode confidence and lead to decreased exercise participation (Gary, 2006; Schweitzer, Head, & Dwyer, 2007); McGrady, McGinnis, Badenhop, Bentle, & Rajput, 2009). Lack of confidence is especially problematic during self-managed, home-based exercise where access to support is withdrawn (Hwang, Redfern, & Alison, 2008).
Exercise is a recommended treatment for several psychological disorders but in HF studies, findings have been conflicting. Exercise participation is reported to improve psychological responses including self-efficacy in HF (Evangelista, Hamilton, Fonarow, & Dracup, 2010; Gary, 2006; Karapolat et al., 2009). Conversely, other research has failed to identify improved psychological outcomes with exercise training in patients with HF(Chien, Lee, Wu, & Wu, 2011; Dracup et al., 2007; Gary, Dunbar, Higgins, Musselman, & Smith, 2010).
Few exercise trials report adherence data other than total number of sessions completed at study end points. The emphasis on adherence as an outcome prevents understanding the psychological process inherent in adherence (Evangelista et al., 2010). Understanding psychological changes that occur during exercise training can provide insight into the processes of adapting to exercise and lead to long term adherence.
Purpose
The purposes of this study were: 1) To compare the psychological responses to a multicomponent exercise training program for an exercise group (INV) and attention control group (AC) during two 12-week phases differing in levels of program support, and 2) To examine the exercise group (INV) in order to describe weekly exercise adherence patterns and to compare changes in psychological responses between a high adherence and low adherence group.
Methods
This study reports data for one of the aims from a randomized clinical trial (RCT) of a multicomponent exercise training intervention called Heart Failure Exercise Training Camp (HEART Camp ) to address the purposes of this exploratory study (Pozehl, Duncan, Hertzog, & Norman, 2010).
Sample
HEART Camp was funded as a pilot study, with the samples size justified as sufficient for the aims of assessing feasibility of the intervention and estimating effect sizes to use in planning a subsequent fully powered study. The sample was recruited from a Midwestern HF clinic. Inclusion criteria were a minimum age of 21 yrs, able to speak and read English, left ventricular ejection fraction of less than 40%, and on stable, optimal HF medication for a minimum of 30 days. The sample for HEART Camp consisted of 42 subjects randomized into two groups: an AC group (n=20) and an exercise intervention (INV) group (n=22). Two patients did not complete both phases of the 24-week study (one patient died and one could no longer exercise) and one patient who was treated for a new psychological condition and was not included in the current analysis. Therefore, the sample for this report was 39 patients who completed the 24-week study, 19 patients in the INV group and 20 in the AC group.
Exercise and adherence intervention
The exercise protocol included three aerobic sessions and two resistance sessions per week. Aerobic exercise included walking on the treadmill and use of a bike and elliptical trainer. Duration for aerobic sessions was 30 minutes at an intensity of 11–12 on the Borg rating of perceived exertion (RPE). Resistance exercise consisted of eight upper and lower body exercises. Access to a Midwestern hospital exercise facility was provided to the exercise group for 24 weeks without charge.
The exercise intervention included strategies designed to support adherence and foster exercise self-efficacy (i.e., goal setting, exercise logs, feedback, heart rate watch, group support, and a web-site). The strategies were derived from Bandura’s Social Cognitive Theory. Social Cognitive Theory posits that self-efficacy is derived from the interrelationship of behavior, cognition, personal and environmental influence (Bandura, 1997). The following describes the use of the adherence strategies for this study.
Participants were given weekly exercise goals for frequency of exercise (number of sessions), duration and intensity. Weekly exercise logs were provided to participants to record exercise participation. Feedback was provided by graphs of each person’s weekly exercise participation (frequency, duration, intensity). Graphs were provided every 3 weeks. Each exerciser was given a watch to wear with exercise that records heart rate. Group sessions were conducted by the investigators during Phase 1 at weekly or biweekly intervals. Group sessions addressed HF education topics (medications, diet, symptoms, and lifestyle management). The sessions also included questions on exercise and the adherence strategies and lasted for a one hour time period. A website was available to the participants with contact information for the investigators and links to education resources. A full description of the strategies has been previously reported (Duncan, Pozehl, Norman, & Hertzog, 2011).
Attention control
An attention control (AC) group was used to control for the influence of contact time with study personnel. During Phase 1, the AC and the INV groups both participated in small, cohort group educational sessions on the HF related topics. The AC group did not participate in the exercise protocol and only the INV group received information on exercise and exercise adherence in the group sessions. Otherwise, the format and frequency of the group sessions were equivalent in content and time spent with the investigators.
Study Protocol
Following IRB approval, consent was obtained and patients were randomized into two groups (INV and AC). The protocol and measures to address intervention fidelity have been previously described (Pozehl et al., 2010).
The study period was 24 weeks, completed in two, 12-week phases. Phase 1, weeks 1–12, was a structured program in which both groups attended weekly or bi-weekly group sessions for education and the INV group received exercise training and adherence strategies. Phase 2, weeks 13–24, was the self-management phase, during which there were no meetings for either the INV or the AC group and exercise and adherence was self-managed.
Instruments
Adherence
Adherence was defined as frequency (number of sessions completed), aerobic duration (mean number of minutes), and intensity (mean RPE ratings) of exercise. Data on exercise participation were obtained from weekly exercise logs completed at the exercise site. Patients recorded the number of aerobic sessions, duration and intensity (RPE) of aerobic exercise, and number of resistance sessions. Only the intervention group completed the exercise program and provided exercise adherence data.
Profile of Mood States (POMS)
The POMS was used to assess psychological mood states (McNair, Lorr, & Dropleman, 1992). The POMS is a 65-item instrument that contains 6 subscales to gauge the moods of anger-hostility, tension-anxiety, depression-dejection, vigor-activity, fatigue-inertia, and confusion-bewilderment through self-report. Participants are asked to respond on a 5-point Likert scale (from 0 = “not at all” to 4 = “extremely”) to words that reflect these mood states. A total mood disturbance score is computed based on subscale scores. Higher scores indicate more negative mood disturbance or distress, except for the vigor-activity subscale where higher scores indicate greater vigor-activity. Cronbach’s alpha for the six sub-scales and total disturbance score at all three data collection time periods was > .75 (range .76 to .94).
Self-efficacy to Exercise
The 16-item Cardiac Exercise Self-Efficacy Instrument (CESEI) by Hickey, Owen &Froman (1992) was revised to measure perceived self-efficacy (SE) to exercise. Items from the original tool that referred to pre-hospital activity were revised for the HF population. A 5-point Likert response scale of 1 (“very little confidence”) to 5 (“quite a lot of confidence”) from the original instrument was utilized. Cronbach’s alpha for the revised instrument in this study ranged from .97 to .98 for the three time points.
Data Analysis
Because group sizes were small and several of the outcome distributions appeared non-normal, nonparametric tests were used to compare across groups and times. The Friedman twoway analysis of variance by ranks was used to test change within each intervention group across the three times (baseline, 12 weeks, and 24 weeks). Significant differences were followed up with the Wilcoxon signed-ranks test to determine which pairs of times differed. Differences between groups were tested using the Mann-Whitney U test, with change from baseline to 12 weeks, 12 to 24 weeks, and baseline to 24 weeks used as dependent variables in separate analyses. Alpha was set at .05 for all tests. As this was a pilot study, no adjustments for multiple tests were made. Effect sizes for pairwise comparisons were estimated as a mean difference, standardized using the baseline standard deviation pooled across groups. As a rough guidefor interpretation, Cohen’s (1988) suggestions of .2 (small), .5 (moderate), and .8 (large) for effect size were used.
At completion of the study, debriefing sessions were conducted with participants in the exercise group. During debriefing, patients made informal comments about their psychological responses during the exercise program indicating that they had experienced various psychological responses during the study period. These informal comments led to a secondary analysis exploring the relationship between adherence and psychological responses in a subgroup analysis within the exercise group. Subgroup analysis is an appropriate method to determine if intervention effectiveness differs for subjects with specific characteristics (Conn, Algase, Rawl, Zerwic, & Wyman, 2010).We used subgroup analysis to determine if subjects in the exercise group who completed more sessions (adhered at a higher frequency level) differed in psychological responses over time from subjects who adhered at a lower frequency.
The total number of aerobic and resistance exercise sessions completed during 24 weeks was used to dichotomize subjects as low frequency or high frequency. The decision to use 24-week exercise frequency to create groups was based on differences in adherence management inherent in the 2 phases of the study (Phase 1, structured and Phase 2, self-management). A total of 120 sessions were recommended during 24 weeks. A completion rate of 75% of the maximum number of sessions equates to 90 sessions, or a mean of 3.75 sessions/week. A weekly frequency of 3 or more sessions is consistent with physical activity recommendations for older adults with heart disease, and with a review of exercise training protocols in HF (Davies et al., 2010; Nelson et al., 2007). A completion rate of 75% of the 120 sessions (90 sessions) was used to divide the groups. Patients were thereby grouped as high (n=12) if they completed more than 90 sessions (range 92–135 sessions) and as low (n=7) if they completed fewer than 90 sessions (range 44–76 sessions) in 24 weeks. The statistical analysis within and between the high and low groups was the same as described above for the INV and AC comparisons.
Results
Purpose 1
Compare the psychological responses to exercise for an exercise (INV) and attention control (AC) groups during two 12-week phases.
There were no baseline differences (p>.05) between the INV and AC groups in gender, EF, duration of diagnosis, or type of HF (See Table 1). The full sample was primarily Caucasian with one African American. There were no significant changes in emotional mood states (POMS) within the exercise (INV) group during the study period (See Table 2). Self-efficacy scores increased significantly in the INV group (χ2=13.31, p<.005) but not in the AC group (χ2=3.48, p=.175). Pairwise comparisons within the INV group using the Wilcoxon signed-ranks test indicated significant change from baseline to 12 weeks (z=2.82, p=.005) and from baseline to 24 weeks (z=3.39, p=.001), but no significant change from 13 to 24 weeks (z=1.50, p=.133). The exercise group increased 0.9 points (d=1.38) by the end of Phase 1, then an additional .2 point by the end of Phase 2. The AC group had a smaller increase of .3 points (d=.46) during Phase 1, with no further increase during Phase 2. Comparisons of the intervention (INV) and attention control (AC) groups on amount of change using the Mann-Whitney U test were significant only for self-efficacy from baseline to 12 weeks (p=.049, d=.92) and from baseline to 24 weeks (p=.010, d=1.23). All other effects sizes (both within and between-group) were .37 or smaller.
Table 1.
Baseline demographic means (SD) and percentages for intervention (INV) and attention control (AC) groups and adherence groups, high and low.
| Groups Characteristics | Attention Control (n=20) | Intervention (n=19) | Invention Adherence Subgroups | |
|---|---|---|---|---|
| High (n=12) | Low (n=7) | |||
| Age | 63.0 (15.1) | 56.1 (12.3) | 59.2 (13.1) | 50.7 (9.5) |
| Ejection fraction | 32.3 (5.5) | 33.9 (6.4) | 34.2 (7.0) | 33.6 (5.6) |
| Duration of HF (mos) | 35.2 (30.0) | 36.0 (23.4) | 30.8 (22.7) | 44.9 (23.6) |
| Gender (%) | ||||
| Female | 8 (40%) | 10 (52.6%) | 6 (50.0%) | 4 (57.1%) |
| Male | 12 (60%) | 9 (47.4%) | 6 (50.0%) | 3 (42.9%) |
| New York Heart Assoc Class (%) | ||||
| II | 9 (45%) | 13 (68.4) | 9 (75.0%) | 4 (57.1%) |
| III | 11 (55%) | 6 (31.6) | 3 (25.0%) | 3 (42.9%) |
| Type of heart failure (%) | ||||
| Ischemic | 13 (65%) | 6 (31.6%) | 4 (33.3%) | 2 (28.6%) |
| Nonischemic | 7 (35%) | 13 (68.4%) | 8 (66.6%) | 5 (71.4%) |
Table 2.
Means (SDs) of Psychological Outcomes by Intervention Group
| Group | N | Baseline | 12 weeks | 24 weeks | Friedmana p value - Within Groups | Mann-Whitney Ub p-value – Between Groups | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline – 12 weeks | Baseline – 24 weeks | 12 – 24 weeks | |||||||
| CES | INV | 17 | 2.8 (0.7) | 3.7 (1.1) | 3.9 (1.0) | <.005 | .049 | .010 | .684 |
| AC | 16 | 2.3 (0.6) | 2.6 (1.0) | 2.6 (0.8) | .175 | ||||
| Tension/Anxiety | INV | 18 | 6.6 (4.4) | 5.6 (3.2) | 5.1 (3.2) | .209 | .771 | .707 | .782 |
| AC | 16 | 8.8 (5.0) | 8.1 (6.5) | 7.3 (5.3) | .448 | ||||
| Depression/Dejection | INV | 18 | 5.8 (5.9) | 4.6 (5.9) | 5.8 (5.0) | .617 | .718 | .515 | .630 |
| AC | 14 | 8.9 (7.5) | 7.6 (6.1) | 6.9 (7.6) | .601 | ||||
| Anger/Hostility | INV | 18 | 3.9 (4.4) | 3.0 (3.4) | 3.1 (3.9) | .476 | .942 | .515 | .630 |
| AC | 14 | 4.0 (5.1) | 4.6 (5.8) | 4.0 (6.4) | .908 | ||||
| Vigor/Activity | INV | 18 | 13.8 (4.9) | 15.4 (6.4) | 14.5 (5.6) | .724 | .317 | .286 | .873 |
| AC | 14 | 14.7 (5.3) | 15.1 (3.2) | 14.5 (4.7) | .835 | ||||
| Fatigue/Inertia | INV | 18 | 8.3 (5.8) | 7.3 (5.8) | 7.7 (6.1) | .956 | .557 | .537 | 1.00 |
| AC | 14 | 9.6 (6.6) | 8.2 (5.5) | 8.1 (6.3) | .183 | ||||
| Confusion/Bewilderment | INV | 18 | 4.9 (2.8) | 4.7 (2.6) | 5.4 (3.4) | .785 | .404 | 843 | .667 |
| AC | 12 | 7.8 (5.7) | 6.7 (4.6) | 7.3 (4.2) | .975 | ||||
| Total POMS | INV | 18 | 15.7 (16.0) | 9.7 (17.6) | 12.6 (17.6) | .412 | .988 | .811 | .682 |
| AC | 12 | 24.1 (27.7) | 19.5 (25.5) | 18.9 (28.1) | .607 | ||||
Note. Patients in INV group received exercise interaction; those in AC group received an attention-control intervention. Means and SDs are calculated using only cases having data on given subscale for all three time points.
The Friedman test compared scores at the three times within each group.
Change scores were calculated for pairwise combinations of times and compared between groups using the Mann-Whitney U tests. All available cases were used in calculations of difference scores.
Purpose 2
Examine the exercise group (INV) in order to describe weekly exercise patterns and psychological responses between a low adherence, and a high adherence subgroup.
During debriefing, exercise participants in this study indicated that frequency of exercise was the most difficult component of the exercise program and over time, the adherence groups demonstrated different patterns in exercise participation. In week 3, the low adherence group decreased in exercise frequency to less than 4 sessions, fell below 3 sessions in week 9, declined below 2 sessions in week 17, and averaged less than one session the last week of the study. Average weekly frequency for the high adherence group reflects 4 weeks at greater than the recommended 5 sessions per week, and only 1 week with fewer than 3 sessions. Weekly mean frequency for the high group was 4.5 sessions/week and 2.2 sessions/week for the low group (p<.001). (Figure 1) During self-management in Phase 2, the number of completed sessions declined for the low group (p=.002). There was no decline in frequency for the high group in Phase 2. During the 24-week study period, the high group achieved a frequency adherence rate of 91.0±10.6% to the recommended 120 sessions as compared to the low group adherence rate of 52.1±10.2% (p<.001).
FIGURE 1.
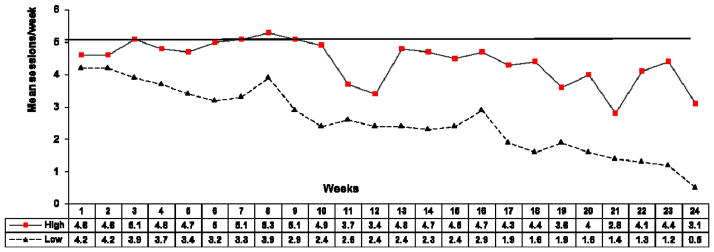
Weekly exercise frequency for high and low adherence groups
Only exercise self-efficacy changed significantly within either adherence group across the study period (Table 3). The Friedman test was significant for the high group (χ2=13.27, p=.001), but not for the low group (χ2=4.261, p=.119). Signed-ranks tests found that change in the high group from baseline to 12 weeks, (z=−2.31, p=.021, d=1.33), baseline to 24 weeks (z=2.85, p=.004, d=1.87), and 12 to 24 weeks (z=−2.63, p=.009, d=.62) were all significant. Mann-Whitney U tests for group differences in the amount of change were significant on depression/dejection (p=.030, d=.61) and for confusion/bewilderment (p=.014, d=1.29) from baseline to 12 weeks. The high group mean scores improved (decreased) during this time while the low group’s mean scores increased (worsened) on both measures. Effect sizes for the remaining between and within-group comparisons were generally very small (d≤.1) except for a moderate effect size (d=.5) for the between comparison on the POMS total score from baseline to 12 weeks and for the baseline to 12 week change on this same measure within the high frequency group.
Table 3.
Means (SDs) of Psychological Outcomes by Exercise Adherence Group
| Group | N | Baseline | 12 weeks | 24 weeks | Friedmana p value - Within Groups | Mann-Whitney Ub p-value – Between Groups | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline – 12 weeks | Baseline – 24 weeks | 12 – 24 weeks | |||||||
| CES | High | 11 | 2.7 (0.8) | 3.7 (1.1) | 4.1 (1.1) | .001 | .650 | .085 | .125 |
| Low | 7 | 3.0 (0.7) | 3.8 (1.1) | 3.6 (0.8) | .119 | ||||
| Tension/Anxiety | High | 12 | 6.6 (4.8) | 5.8 (3.3) | 4.8 (3.0) | .424 | 1.00 | .837 | .385 |
| Low | 7 | 6.7 (3.8) | 5.0 (3.0) | 5.7 (3.8) | .387 | ||||
| Depression/Dejection | High | 12 | 5.9 (6.2) | 3.5 (4.2) | 4.4 (4.7) | .103 | .030 | .100 | .750 |
| Low | 7 | 5.5 (6.0) | 6.8 (8.4) | 8.7 (4.6) | .264 | ||||
| Anger/Hostility | High | 12 | 4.3 (4.4) | 2.5 (3.0) | 3.4 (4.4) | .521 | .351 | .773 | .335 |
| Low | 7 | 3.3 (4.7) | 4.0 (4.0) | 2.5 (3.0) | .738 | ||||
| Vigor/Activity | High | 12 | 13.8 (5.4) | 15.2 (6.1) | 14.2 (4.5) | .911 | .817 | .592 | .820 |
| Low | 7 | 13.8 (3.9) | 16.0 (7.5) | 15.2 (7.9) | .727 | ||||
| Fatigue/Inertia | High | 12 | 7.6 (5.3) | 6.0 (4.2) | 6.8 (5.5) | .544 | .157 | .837 | .553 |
| Low | 7 | 9.7 (7.0) | 9.8 (7.9) | 9.3 (7.4) | .538 | ||||
| Confusion/Bewilderment | High | 12 | 5.6 (3.0) | 4.3 (2.3) | 5.0 (3.3) | .307 | .014 | .299 | .820 |
| Low | 7 | 3.7 (2.1) | 5.7 (3.1) | 6.2 (3.8) | .580 | ||||
| Total POMS | High | 12 | 16.1 (14.5) | 6.9 (10.7) | 10.3 (15.4) | .094 | .097 | .711 | .750 |
| Low | 7 | 15.0 (20.2) | 15.3 (27.4) | 17.2 (22.2) | .607 | ||||
Note. Patients in HI group completed at least 90 sessions over 24 weeks; those in the low group completed fewer than 90. Means and SDs are calculated using only cases having data on given subscale for all three time points.
The Friedman test compared scores at the three times within each group.
Change scores were calculated for pairwise combinations of times and compared between groups using the Mann-Whitney U tests. All available cases were used in calculations of difference scores..
Discussion
The exercise training intervention was designed to assist patients with HF in learning to adhere to exercise. Results indicate that self-efficacy for exercise increased for the exercise group as compared to the attention control (AC) group between baseline and the end of Phase 1, the structured phase, and between baseline and the end of Phase 2, the self-managed phase. The findings for self-efficacy during Phase 1 have been previously reported (Pozehl et al., 2010). This study found that increased self-efficacy scores were sustained for weeks 12–24, (Phase 2) the time period when patients self-managed exercise and when less adherence support was available. Adherence support was provided in the first 12 weeks for the intervention group and an increase in self efficacy in this period was anticipated. The continued increase in self-efficacy when adherence support was not provided may reflect a sustained impact from the intervention during Phase 1 on independent exercise in Phase 2.
This study found no differences in psychological moods for the exercise group (INV) as compared to the AC group over time. Research on exercise in cardiac populations has reported improved psychological responses, most notably for depression and anxiety (Evangelista et al., 2010; Herring, Puetz, O’Connor, & Dishman, 2012; Karapolat et al., 2009). Lack of improvement in mood states by exercisers (INV) in this study as compared to non-exercisers (AC) may reflect the less frequent exercise reported by the low frequency group which represented nearly 40% of the exercise sample.
Findings related to the subgroup analysis provide interesting observations on psychological responses to adherence. By the end of Phase 1, the high exercisers had improved in depression, and confusion while the low group worsened for depression and confusion. Previous research has demonstrated the importance of adherence in achievement of physiological and QOL benefits from exercise (Flynn et al., 2009). Our data support a recent review on exercise that found greater psychological benefits with higher exercise participation (Herring, et al., 2012).
Adherence groups demonstrated different patterns in exercise frequency as early as the initial three weeks of the 24-week study. These findings support previous research indicating that initial exercise frequency may be an early indicator of ability to adhere to an exercise program longer term (Corvera-Tindel, Doering, Gomez, & Dracup, 2004). Lower participation at the start of a program may foster a continual decline that is difficult to reverse.
This study found self-efficacy improved for the high group during Phase 1 and remained high during Phase 2. These results are supported by moderate to large effect sizes for self-efficacy following each phase. Self-efficacy also increased for the low group during Phase 1, though not significantly so. Previous studies support the relationship between self-efficacy and exercise adherence (Gary, 2006; Schweitzer et al., 2007). Phase 1 was the period when groups participated in sessions with the investigators which may have increased all patients’ confidence in their ability to exercise. The further increase in self-efficacy scores observed after Phase 2 for the high group may reflect this group’s continuation of exercise participation as recommended. A surprising finding for the low group was that while exercise frequency decreased, self-efficacy scores did not decline. It may be that the low group remained confident in their ability to exercise even though they were not able to meet frequency recommendations. Self-efficacy reflects a personal belief in the ability to exercise. For patients with low exercise participation, failure to meet frequency goals may be reflected by worsening of emotional moods, such as depression, rather than a loss of confidence.
Limitations and strengths
Findings for this study are preliminary. Limitations include the small, homogenous (primarily Caucasian) sample which yielded low power for the assessment of changes. The exercise and adherence intervention was delivered in cohort groups, resulting in a potential correlation in the outcomes of individuals within the same small group. This exploratory analysis created additional subgroups and the sample size was not large enough to employ methods that would have allowed us to take this dependence of observations into account. Data on exercise frequency was based on self-reports and may reflect over reporting of completed sessions. Strengths of the study include random assignment to the exercise (INV) and attention control group (AC); inclusion of an attention group in the study design to decrease the confound of investigator interaction during an exercise training trial; the use of patients’ actual exercise participation for determination of adherence groups which allowed for examination of non-manipulated exercise patterns; and weekly exercise frequency data from two different phases in adherence management.
Conclusion
This study examined psychological responses to a two-phase multicomponent exercise intervention for an INV and AC group and found an improvement in self-efficacy that was sustained over 24 weeks. Examination of data from two exercise adherence groups found different patterns of weekly exercise and positive changes in the psychological moods of depression, confusion and self-efficacy for those who exercise more often.
Much remains unknown concerning the impact of psychological effects on exercise participation in HF and this study was not able to address issues of causality between the two concepts. There is no consensus on the level of exercise participation needed to improve psychological functioning in HF. Findings from this study support further investigation of the psychological effects of exercise frequency in HF populations and examination of methods to sustain exercise participation.
Clinical Relevance
This study was one of few to explore the relationship between exercise adherence and psychological responses (Gary et al, 2010). For patients with HF, the initial three weeks of an exercise program may be a critical time period in the development of adherence. Adherence support that is targeted to patients who are unable to exercise at recommended levels in the early weeks of an exercise program may prevent a continual decline in participation. For those patients who meet or exceed exercise frequency goals in the early weeks of an exercise program, less adherence support maybe needed.
A supportive relationship between the patient and rehabilitation professionals underlies the rehabilitation process. This study found that self-efficacy increased for both the high and low adheres in the first 12 weeks of the program when patients closely interacted with exercise professionals. A continued relationship with rehabilitation professionals may also be helpful after a structured program is completed. Heart failure is a chronic disease that impacts exercise tolerance. New symptoms can occur and patients may need longer term assistance to differentiate exercise induced symptoms from exacerbation of HF.
Booster sessions are reported to support exercise adherence for patients with HF (Dracup et al., 2007). These sessions can be offered by rehabilitation nurses following completion of the structured exercise program. In this study, both high and low adherence groups trended down in exercise frequency in the self-management phase. In booster sessions, rehabilitation nurses could problem-solve barriers for patients who have stopped exercising and provide positive feedback to patients who are still exercising. The inclusion of booster sessions can provide a way for patients to continue to receive adherence support from rehabilitation nurses. Further studies of weekly exercise participation may help identify the time intervals most beneficial for these sessions.
During this exercise program the adherence groups exhibited different psychological responses for confusion and depression in the structured phase and both groups trended up for these mood states during the self-managed phase. These results suggest it may be helpful to assess patients for signs of depression and to query them about understanding their progress throughout an exercise program. This assessment can be informal and include open-ended questions that allow for further exploration. General questions such as inquiring as how the person feels about exercise progress, asking what is going well, and what is has been difficult will provide opportunities to explore emotional responses and motivational barriers. In this way, rehabilitation nurses can help patients learn to problem-solve emotional and physical obstacles to continued exercise. The inclusion of psychological responses as well as physiological responses in the evaluation of exercise progress may lead to a better understanding of exercise adherence for patients with HF.
Acknowledgments
Funding for this study was provided by NIH-NINR #R15NR009215-01
Contributor Information
Kathleen Duncan, Email: kduncan@unmc.edu, College of Nursing-Lincoln Division, University of Nebraska Medical Center, PO Box 880220, Lincoln, NE 68588-0220, 402-472-7338, Fax 402-472-7345.
Bunny Pozehl, Email: bpozehl@unmc.edu, College of Nursing-Lincoln Division, University of Nebraska Medical Center.
Melody Hertzog, Email: mhertzog@unmc.edu, College of Nursing-Lincoln Division, University of Nebraska Medical Center, Lincoln, NE 68588-0220.
Joseph F. Norman, Email: jfnorman@unmc.edu, Division of Physical Therapy Education, University of Nebraska Medical Center, 984420 Nebraska Medical Center, Omaha, NE 68198-4420.
References
- Bandura A. Self-efficacy: The exercise of control. New York: W. H. Freeman; 1997. [Google Scholar]
- Chien CL, Lee CM, Wu YW, Wu YT. Home-based exercise improves the quality of life and physical function but not the psychological status of people with chronic heart failure: A randomised trial. Journal of Physiotherapy. 2011;57(3):157–163. doi: 10.1016/S1836-9553(11)70036-4. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- Conn VS, Algase DL, Rawl SM, Zerwic JJ, Wyman JF. Publishing pilot intervention work. Western Journal of Nursing Research. 2010;32(8):994–1010. doi: 10.1177/0193945910367229. [DOI] [PubMed] [Google Scholar]
- Corvera-Tindel T, Doering LV, Gomez T, Dracup K. Predictors of noncompliance to exercise training in heart failure. The Journal of Cardiovascular Nursing. 2004;19(4):269–77. doi: 10.1097/00005082-200407000-00006. [DOI] [PubMed] [Google Scholar]
- Davies EJ, Moxham T, Rees K, Singh S, Coats AJ, Ebrahim S, et al. Exercise based rehabilitation for heart failure. Cochrane Database of Systematic Reviews (Online) 2010;(4):CD003331. doi: 10.1002/14651858.CD003331.pub3. [DOI] [PubMed] [Google Scholar]
- Dracup K, Evangelista LS, Hamilton MA, Erickson V, Hage A, Moriguchi J, et al. Effects of a home-based exercise program on clinical outcomes in heart failure. American Heart Journal. 2007;154(5):877–883. doi: 10.1016/j.ahj.2007.07.019. [DOI] [PubMed] [Google Scholar]
- Duncan K, Pozehl B, Norman JF, Hertzog M. A self-directed adherence management program for patients with heart failure completing combined aerobic and resistance exercise training. Applied Nursing Research : ANR. 2011;24(4):207–214. doi: 10.1016/j.apnr.2009.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evangelista LS, Berg J, Dracup K. Relationship between psychosocial variables and compliance in patients with heart failure. Heart & Lung : The Journal of Critical Care. 2001;30(4):294–301. doi: 10.1067/mhl.2001.116011. [DOI] [PubMed] [Google Scholar]
- Evangelista LS, Hamilton MA, Fonarow GC, Dracup K. Is exercise adherence associated with clinical outcomes in patients with advanced heart failure? The Physician and Sportsmedicine. 2010;38(1):28–36. doi: 10.3810/psm.2010.04.1759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flynn KE, Pina IL, Whellan DJ, Lin L, Blumenthal JA, Ellis SJ, et al. Effects of exercise training on health status in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA : The Journal of the American Medical Association. 2009;301(14):1451–1459. doi: 10.1001/jama.2009.457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gary R. Exercise self-efficacy in older women with diastolic heart failure: Results of a walking program and education intervention. Journal of Gerontological Nursing. 2006;32(7):31–9. doi: 10.3928/00989134-20060701-05. quiz 40–1. [DOI] [PubMed] [Google Scholar]
- Gary RA, Dunbar SB, Higgins MK, Musselman DL, Smith AL. Combined exercise and cognitive behavioral therapy improves outcomes in patients with heart failure. Journal of Psychosomatic Research. 2010;69(2):119–131. doi: 10.1016/j.jpsychores.2010.01.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haworth JE, Moniz-Cook E, Clark AL, Wang M, Waddington R, Cleland JG. Prevalence and predictors of anxiety and depression in a sample of chronic heart failure patients with left ventricular systolic dysfunction. European Journal of Heart Failure. 2005;7(5):803–808. doi: 10.1016/j.ejheart.2005.03.001. [DOI] [PubMed] [Google Scholar]
- Herring MP, Puetz TW, O’Connor PJ, Dishman RK. Effect of exercise training on depressive symptoms among patients with a chronic illness: A systematic review and meta-analysis of randomized controlled trial. Archives of Internal Medicine. 2012;172(2):101–111. doi: 10.1001/archinternmed.2011.696. [DOI] [PubMed] [Google Scholar]
- Hickey ML, Owen SV, Froman RD. Instrument development: Cardiac diet and exercise self-efficacy. Nursing Research. 1992;41(6):347–351. [PubMed] [Google Scholar]
- Hwang R, Redfern J, Alison J. A narrative review on home-based exercise training for patients with chronic heart failure. Physical Therapy Reviews. 2008;13(4):227–236. [Google Scholar]
- Karapolat H, Demir E, Bozkaya YT, Eyigor S, Nalbantgil S, Durmaz B, et al. Comparison of hospital-based versus home-based exercise training in patients with heart failure: Effects on functional capacity, quality of life, psychological symptoms, and hemodynamic parameters. Clinical Research in Cardiology : Official Journal of the German Cardiac Society. 2009;98(10):635–642. doi: 10.1007/s00392-009-0049-6. [DOI] [PubMed] [Google Scholar]
- McGrady A, McGinnis R, Badenhop D, Bentle M, Rajput M. Effects of depression and anxiety on adherence to cardiac rehabilitation. Journal of Cardiopulmonary Rehabilitation and Prevention. 2009;29(6):358–364. doi: 10.1097/HCR.0b013e3181be7a8f. [DOI] [PubMed] [Google Scholar]
- McNair DM, Lorr M, Dropleman L. Profile of mood states. 3. San Diego: Educational and Industrial Service; 1992. [Google Scholar]
- Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: Recommendation from the american college of sports medicine and the american heart association. Medicine and Science in Sports and Exercise. 2007;39(8):1435–1445. doi: 10.1249/mss.0b013e3180616aa2. [DOI] [PubMed] [Google Scholar]
- Pozehl B, Duncan K, Hertzog M, Norman JF. Heart failure exercise and training camp: Effects of a multicomponent exercise training intervention in patients with heart failure. Heart & Lung : The Journal of Critical Care. 2010;39(6 Suppl):S1–13. doi: 10.1016/j.hrtlng.2010.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutledge T, Reis VA, Linke SE, Greenberg BH, Mills PJ. Depression in heart failure a meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes. Journal of the American College of Cardiology. 2006;48(8):1527–1537. doi: 10.1016/j.jacc.2006.06.055. [DOI] [PubMed] [Google Scholar]
- Schweitzer RD, Head K, Dwyer JW. Psychological factors and treatment adherence behavior in patients with chronic heart failure. The Journal of Cardiovascular Nursing. 2007;22(1):76–83. doi: 10.1097/00005082-200701000-00012. [DOI] [PubMed] [Google Scholar]