

Abstract
The purpose of this study was to assess, the effects of continuous and intermittent exercise training on lactate kinetic parameters and maximal aerobic speed (MAS) using field tests. Twenty-four male sport students were equally divided into continuous (CT) and intermittent (IT) physically trained groups. Another six participants acted as non-trained controls (CG). The trained participants practiced 6-days per week for 6 weeks. Before and after training, all participants completed an incremental exercise test to assess their MAS, and a 30- second supra-maximal exercise followed by 30 minutes of active recovery to determine the individual blood lactate recovery curve. It was found that exercise training has significantly increased MAS (p < 0.001), the lactate exchange and removal abilities as well as the lactate concentrations at the beginning of the recovery ([La]-(0)); for both CT and IT groups; this was accompanied by a significant reduction of the time to lactate-peak. Nevertheless, the improvement in MAS was significantly higher (p < 0.001) post-intermittent (15.1 % ± 2.4) than post-continuous (10.3 % ± 3.2) training. The lactate-exchange and removal abilities were also significantly higher for IT than for CT-group (P<0.05). Moreover, IT-group showed a significantly shorter half-time of the blood lactate (t-½-[La]) than CT-group (7.2 ± 0.5 min vs 7.7 ± 0.3 min, respectively) (p < 0.05). However, no significant differences were observed in peak blood lactate concentration ([La]peak), time to reach [La]peak (t-[La]peak), and [La]-(0) between the two physically-trained groups. We conclude that both continuous and intermittent training exercises were equally effective in improving t-[La]peak and [La]peak, although intermittent training was more beneficial in elevating MAS and in raising the lactate exchange (γ1) and removal (γ2) indexes.
Key points.
Coaches and athletes need to be aware of the potentiality positive effects of exercise intensity.
Improvements in physical fitness are associated with a concomitant increase in the lactate removal ability.
In order to reduce lactate accumulation and increase maximal aerobic speed maximally, interval training method, with work speeds equal to 90% - 100% of MAS, may be the effective way when compared with continuous training method.
Key words: Biexponential mathematical model, recovery, supra-maximal exercise.
Introduction
The effects of exercise training and training methods on lactate kinetics have been widely studied, but the conclusions remain controversial and unclear. For instance, some investigators reported that whereas endurance exercise training enhances blood lactate clearance capacity (Freund et al., 1992), intermittent exercise training is a more effective method to improve aerobic capacity and to increase lactate threshold (LT) (Evertsen et al., 2001; Gorostiaga et al., 1991). Other studies have yielded conflicting results suggesting that both continuous and intermittent exercise training were equally effective in augmenting LT (Edge et al., 2005; Poole and Gaesser, 1985). The difference between methodological approaches and experimental procedures such as the lactate sampling-times and the use of monoexponential rather than biexponential curves to describe lactate recovery might account for some of the mentioned discrepancies. Moreover, differences in lactate clearance capacity between endurance-trained and untrained individuals have been often assessed during recovery from exercise at the same relative intensity rather than at the same level of blood lactate accumulation. Although, Bassett and collaborators (1991) attempted to manage this issue by adjusting individual workloads to produce the same blood lactate concentration. Their finding of no difference in peak lactate between the groups supported the need for further research. Several investigations have reported that endurance training had no significant effect on peak lactate at the maximal aerobic speed (MAS) (Billat et al., 2004; Laffite et al., 2003), maximal lactate steady state concentration (MLSSc) (Billat et al., 2004), blood lactate clearance (Mayes et al., 1987), LT (Slawinski et al., 2001) or velocity at the LT (Laffite et al., 2003). Other investigators report that endurance exercise training improves lactate clearance capacity (Messonnier et al., 2006), raises LT (Edge et al., 2005; 2006; Evertsen et al., 2001; Poole and Gaesser, 1985), enhances maximal lactate steady state velocity (MLSSv) (Billat et al., 2004) and increases the velocity at the lactate threshold (vLT) (Billat et al., 2004; Evertsen et al., 2001).
Endurance training induces adaptations in several physiological systems (i.e. metabolic, cardiovascular, muscular, etc.). One of the significant effects of these adaptations is the modification of lactate kinetic parameters (Edge et al., 2005; Evertsen et al., 2001; Gorostiaga et al., 1991; Messonnier et al., 2006; Poole and Gaesser, 1985). Poole and Gaesser, 1985 and Edge and coworkers (2005) have reported that intermittent and continuous exercise training have a similar, positive effect on LT. Conversely, other studies have shown greater improvements in aerobic fitness and LT after intermittent than after continuous exercise training (Evertsen et al., 2001; Gorostiaga et al., 1991).
A unique mathematical descriptive model that includes two exponential terms to describe the kinetics of lactate can be used to represent blood lactate recovery curves after exercise. A two- compartmental model consisting of the previously working muscles and the remainder of the lactate space provides the simplest, most realistic explanation of the lactate profile (Oyono-Enguelle et al., 1993). The advantage of this mathematical model is that it can be applied to supra-maximal exercise and supply information on the overall ability of lactate exchange and removal.
To our knowledge, this modelling approach had never been applied to single out differences in lactate exchange and removal abilities after intermittent and continuous training. Therefore, the objective of this current work was to use the biexponential model in order to investigate the possible differential benefits from intermittent and continuous physical training on lactate exchange and removal abilities.
Methods
Subjects
Thirty male sports students from the same sport academy participated in the study. Twelve subjects were recruited for each of the two experimental groups and the remaining 6 subjects were assigned as control. None of the students practiced any physical activity outside the academy. The average (± SD) age, height, and body mass of the participants was 20 (2) years, 1.72 (0.02) m, and 72 (3.2) kg, respectively. The subjects were divided into three homogeneous groups according to their MAS. The physically trained groups performed their continuous and intermittent exercise programs simultaneously. Each participant gave his written informed consent knowing, the potential benefits, and the study associated-risks. The study protocol was approved by the research ethics committee of the Hospital Farhat Hached, Sousse Tunisia.
Protocol
Two running field tests were conducted before as well as after the six-week training program with 48-h in-between.
The first session was a maximal continuous graded exercise test performed to measure the maximal aerobic speed (MAS) (Chtara et al. , 2005). It consisted of a running trial around a 200 m track calibrated by reference marks placed every 20- m. Goal speed was indicated using calibrated sound signals from a tape recorder. The speed started at 8-km/h and increased by 0.5 km/h every minute. The last completed stage reached by the subject corresponded to his maximal aerobic speed (MAS).
The second session was designed to assess the individual blood lactate recovery curves and recovery peak-lactate concentrations. The test began with 20-minutes warm-up exercise at 60-% MAS, then subjects performed a supramaximal exercise (140% of MAS) for 30 seconds, followed by 30 minutes of active recovery running at 30% of their MAS. The intensity of the active recovery was chosen to be within the range of those recommended to withdraw blood samples to measure lactate concentration (Gorostiaga et al., 1991). Blood samples were taken at rest, at the end of the exercise (t0) and during the recovery periods. The running velocity during supramaximal exercise and active recovery was controlled by placing marks at every 20 meters and using a sonorous signal to determine the running rhythm. When this test was performed after the training period, new MAS values were used (i.e. MAS values of the re- test).
Training
Each pair of matched subjects was required to complete the same amount of work during a training session. Training intensity was set as a percentage of MAS. The subjects in the two experimental exercise groups performed six physical training sessions per week with the seventh day as rest day for six consecutive weeks. Group 1 performed moderate-intensity training in a continuous manner (CT), whereas group 2 performed high-intensity training in an intermittent manner (IT). The subjects in the control group did not participate in the training program, and they were instructed to keep their normal daily activity during this study. All training sessions were completed on the field.
The IT-group trained at an intensity of 90% MAS and increased 5% every two weeks (reaching 100% MAS for the last two weeks). Intervals were of 2 min duration, with 1 min recovery (work-to-rest ratio 2:1). Progression was controlled by altering the workload and the number of intervals performed in a training session.
The CT-group performed exercise at an intensity of 60% (weeks 1 and 2), 65% (weeks 3 and 4), and 70% (last two weeks) of MAS. The training was continuous (running, with no rest periods). Progression was controlled by increasing the workload and exercise duration to equal the total work performed by their matched pair in the IT-group. Due to the training intensities chosen and the matching of groups on total work, the duration of a training session was similar between both groups. For example, when a subject with a MAS of 17 km·h-1 (training at 90% MAS during week 1 = 15.3 km·h-1) from the IT-group performed eight 2 min intervals (+1 min rest periods), the subject with a MAS of 17 km·h-1 (training at 60% MAS during week 1 = 10.2 km·h-1) from the CT-group (matched pair) ran for 24 min matching the total distance covered.
Training duration for the continuous and intermittent groups were increased from 35 minutes the first week to 75 minutes the sixth week (warm up excluded).
These two types of physical training were preceded by 15 minutes of warming-up at 50% MAS. After the training, the subjects underwent the same experimental protocol as during the pre-training period to assess the adaptations induced by training. No subjects withdraw from the study before the achievement of the post-training tests evaluation and none complained from health complications throughout the study.
Blood lactate measurements and analysis
Blood samples from the subjects' fingers were analyzed using an automated lactate analyzer (Accutrend, Boehringer Mannheim, Mannheim, Germany), which had been previously validated (Fell et al., 1998). Resting-blood lactate concentration was determined on a sample drawn prior to warm-up. Further blood samples were drawn to plot the individual blood lactate recovery curve. Blood lactate was measured at rest, at the end of the 30 sec-bout of exercise (time zero of recovery), and at the 2nd, 4th, 6th, 9th, 12th, 15th, 20th, 25th, and 30th minute of recovery and the mathematical model interests only the first fifteen minutes.
This standardised protocol allowed assessing the peak blood lactate concentration ([La]peak) and the time to reach [La]peak (t-[La]peak). The half-time of the blood lactate removal (t-½-[La]) was determined using the linear regression fit between blood lactate concentration and recovery time (McLellan and Skinner, 1982). The t-½-[La] represents the time to that the lactate concentration return to the half of the delta value between the peak concentration and resting concentration.
Each individual curve was fitted using the following biexponential equation (Freund and Gendry, 1978):
Where: [La](t) and [La](0) (mmol/l) are the measured blood lactate concentrations at time t after the end of the exercise and at the beginning of the recovery, respectively.
A1 and A2 (in mmol/l) are the amplitudes of the two exponential components γ1 and γ2 (per minute) are the time constants.
The individual parameters of the biexponential function were fitted by means of an iterative nonlinear technique, using Microcal Origin 5.0 Software to determine the values of A1, A2, γ1 and γ2.
Statistical analysis
All results are expressed as mean (± SD). After checking the normality of the distribution with the Komolgorov-Smirnov test, we used a two-way ANOVA for repeated measures in order to assess the differences between groups and between the tests before (pre) and after (post) training period within each group. LSD post-hoc tests were used to determine where significant differences
occurred. Pearson correlations were used to assess the relationships between variables. Statistical significance was set at p < 0.05.
Results
Table 1 illustrates the mean pre- and post-test absolute and relative changes in MAS. The mean values of the parameters from the fits and the application of the model are summarized in Table 2 and Figure 1. No significant differences were found between groups for any variable before training (Figure 1, Table 1 and 2).
Table 1.
Mean (SD) maximal aerobic speed (km·h-1), before and after 6 weeks of training.
| Group | Pre-test | Post-test | ∆ | %∆ |
|---|---|---|---|---|
| CT | 15.3 (1.3) | 16.8 (.9) *† | 1.54 (.37) # | 10.3 (3.2) † |
| IT | 15.0 (1.2) | 17.2 (1.1) *‣ | 2.25 (.19) ‣‡ | 15.2 (2.5) †‡ |
| CG | 15.2 (1.3) | 15.4 (1.0) | .13 (.30) | 1.0 (2.0) |
CT, continuous training; IT Intermittent training; CG, control group; ∆ = post-test - pre-test; %∆ = ((post-test - pre-test)/ pre-test) × 100.
* p < 0.001 for differences with the pre-test value
† p < 0.05 and # p < 0.001 significantly greater than CG
‡ p < 0.001 significantly greater than CT.
Table 2.
Mean (±SD) blood lactate characteristics and lactate kinetics parameters for 3 groups.
| CT | IT | CG | ||
|---|---|---|---|---|
| t-½-[La] (min) | Pre | 8.75 (.39) | 8.87 (.48) | 8.79 (.64) |
| Post | 7.77 (.39) ***† | 7.20 (.52)*** #‡ | 8.54 (.74) | |
| [La](0) (mmol·l-1) | Pre | 5.00 (.74) | 4.90 (.64) | 5.00 (.70) |
| Post | 6.00 (.64) *† | 6.20 (.60) *# | 5.10 (.60) | |
| [La]peak (mmol·l-1) | Pre | 8.75 (.70) | 8.47 (.66) | 8.40 (.50) |
| Post | 9.00 (.74) * | 9.30 (.75) * | 8.30 (.60) | |
| t-[La]peak (min) | Pre | 3.50 (.90) | 3.50 (.90) | 3.33 (1.00) |
| Post | 2.00 (.00) ***† | 2.00 (.00) ***† | 3.30 (1.00) |
CT, continuous training; IT Intermittent training; CG, control group; t ½ [La]: the half time of the blood lactate removal; [La](0): Pre-training vs. Post-training values for blood lactate concentration at the beginning of recovery; [La]peak: peak blood lactate concentration measured during the recovery; t [La] peak: time to peak lactate.
* p < 0.05
*** p < 0.001 significantly different from pre-training
† p < 0.05 and # p < 0.001: significantly difference change compared with CG,
‡ p < 0.05: Significantly different from CT.
Figure 1.
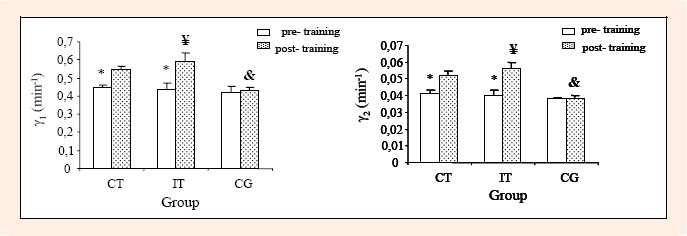
Pre-training vs. Post-training values for the velocity constants that represent the lactate exchange (γ1) and removal (γ2) abilities in the different training groups. Results are presented by mean (±SD).* p < 0.001 significantly different from post-training, & p < 0.001 significantly difference change compared with CT and IT, ¥ p < 0.05 significantly different from CT.
A significant time-effect was obtained for MAS. The LSD post-hoc indicated that MAS was significantly improved after the physical training period, whereas no changes were observed in the control group. The improvement of MAS was higher (p 0.001) for IT-group (15.19% ± 2.48) than for CT-group (10.33% ± 3.22).
Blood lactate concentration during recovery before and after the training program were fitted with Eq.1 and the different parameters of this model were analysed. At the end of the training period, γ1, γ2, and [La](0) were significantly increased, and t-½-[La] and t-[La]peak were significantly decreased, for both CT and IT-groups. But, no changes were observed in the control group.
The parameters of lactate exchange (γ1) and removal (γ2) abilities were found to be higher for IT-group than for CT-group (Figure 1). Additionally, IT-group showed a significantly shorter t-½-[La] than CT-group (Table 2). No significant differences were observed in [La](0), t-[La]peak and [La]peak between the two trained groups (Table 2).
As reported in Figure 2, the lactate exchange and removal abilities were positively and significantly correlated with MAS (r = 0.65 and r = 0.72, respectively, p 0.001). Moreover, a significant correlation was found between [La]peak and t-½-[La] (r = -0.70, p 0.001, Figure 3). Likewise, a significant correlation resulted between [La](0) and distance covered during 30s-sprint (r = 0.97, p 0.001, Figure 4).
Figure 2.
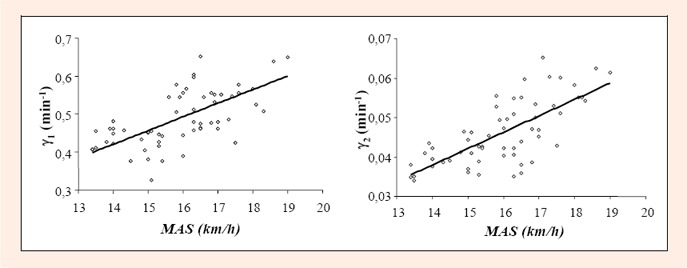
Relationship between maximal aerobic speed (MAS) and the lactate exchange (γ1) and removal (γ2) abilities. All subjects combined.
Figure 3.
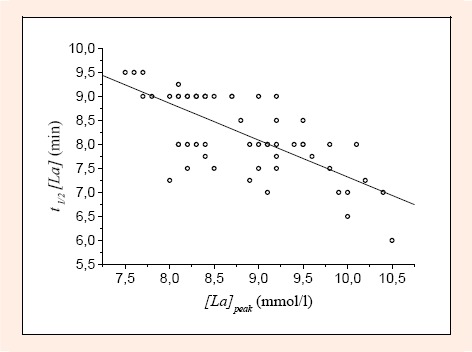
Relationship between the t-½-[La] and the [Las]peak. All subjects combined.
Figure 4.
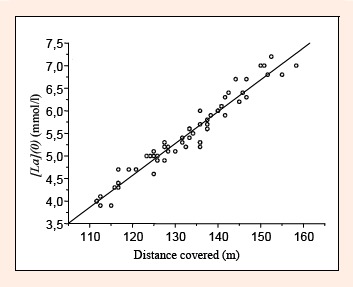
Relationship between the lactate concentration at the end of exercise ([La] (0)) and the distances covered during 30 s. All subjects combined.
Discussion
The main findings of the present study suggest that intermittent training was more effective in enhancing MAS and raising the lactate exchange (γ1) and removal (γ2) abilities than continuous training. However, both training methods were equally effective in altering t-[La]peak and [La]peak.
The improvement in MAS was 1.5-times higher for the IT than for the CT-group. Some investigators (Evertsen et al., 2001; Gorostiaga et al., 1991) have reported that intermittent physical training is an effective method to improve aerobic capacity, but other studies (Edge et al., 2006; Poole and Gaesser, 1985) do not agree with this conclusion. Our results may be explained by the consequence of an adaptation process that is the result of the mode and/or intensity of the physical training. This was corroborated by a previous study (Gorostiaga et al., 1991) showing that IT produced a higher increase in VO2max than CT, suggesting that a range of training intensities could lead to a greater improvement in VO2max (Gorostiaga et al., 1991). The magnitude of improvement in MAS after intermittent training programs might be affected by the percentage of VO2max during training and the time for which it was sustained (Tabata et al., 1997). Indeed, it might be reasonable to assume that high oxygen uptake obtained during intermittent training led to a high stress on the aerobic system and hence a large increase in VO2max (Billat et al., 2000; Tabata et al., 1997). Moreover, it is possible that the training intensity used during continuous training was not sufficiently high to maximize VO2max improvements (Weltman et al., 1992) and did not stress the oxygen delivery system maximally (Tabata et al., 1997). This continuous mode of training may therefore be less effective than intermittent training for improving MAS.
Physical training increased γ1 by 27.7 ± 6.6% and γ2 by 32.7 ± 6.3%. The improvements in lactate exchange and removal rates respectively are in agreement with the results reported by Messonnier et al., 2006 and Bret et al., 2003. These improvements could be due to an increase in muscle capillary density (Messonnier et al., 2006), mitochondrial volume density, several enzymes of oxidative metabolism, and/or monocarboxylate transporters (MCTs) (Thomas et al., 2005).
The close significant correlations between γ1, γ2 and MAS suggest that the subjects exhibiting the higher exchange and removal abilities were also those who displayed the higher MAS (Figure 2). Therefore, in already well trained subjects (with fairly stable VO2 max and running economy), MAS testing could provide a strong indirect indication of changes in lactate exchange and removal abilities. Our results are in agreement with Messonnier et al., 2001 who reported that improvements in physical fitness are associated with a concomitant increase in the lactate removal rate. Nevertheless, others conclude that training status has no effect on the lactate removal ability during recovery from 3-min cycling exercise bouts (Bassett et al., 1991) and after high intensity exercise (Oosthuyse and Carter, 1999). The disagreement with our study is probably due to differences in the study-protocol, as the 3-min exercise bouts were not of high intensity and resulted in La-peaks lower than the present one. In addition, it is possible that the recovery mode used in these studies (passive) was not as good as full active recovery.
As reported in Table 2, the post-training t-[La]peak appeared to be reduced compared to the pre-training values. This is in agreement with previously reported results from Bassett and co-investigators (1991) who found that physically trained subjects demonstrated a faster time to peak, an indication of a faster efflux of lactate from muscle to blood (Bassett et al., 1991; Freund et al., 1992). Moreover, values of t-½-[La] were significantly reduced after training (Table 2). This result might be explained by the higher VO2 observed in trained subjects (Gmada et al., 2005) and greater peak concentration in blood lactate. The observed relationship between t-½-[La] and [La]peak (Figure 3) confirms these data.
Six weeks of either intermittent or continuous endurance exercise training induce a significant increase in [La](0) (Table 2). These changes are consistent with the results of previous reports showing that training can increase post-exercise lactate concentration (Edge et al., 2005; Juel et al., 2004). These authors suggested that the reason for the higher blood lactate release after training is a combination of an increased production of lactate and H+ transporting proteins (MCT1) with an improved blood-flow and blood-flow distribution. Hence, this could explain the increase of the distance covered during the 30s-sprint post-training. This finding could be confirmed by the positive correlation between [La](0) and the distance covered during 30s-sprint shown in Figure 4.
To be consistent, we applied exactly the same exercise-test protocols before and after training. Since MAS increased with training, there was inevitably an increase in the absolute velocity of the sprint exercise, then, the greater [La](0) production after training is probably due to the greater absolute velocity/intensity.
The fact that lactate exchange and removal abilities in IT-group were higher than in CT-group is most likely due to the circulatory and/or metabolic adaptations induced by intermittent training, since total distance covered during training was identical between groups. Indeed, it is admitted that the biochemical adaptations in slow twitch and fast twitch muscle fibres are not the same for continuous and interval exercise training (Dudley et al., 1982). Studies on rats indicated that interval training increased the oxidative capacity of slow-twitch and fast-twitch fibres (Dudley et al., 1982). In fact, ST fibres are very efficient for lactate oxidation during exercise and recovery (Donovan and and Pagliassotti, 2000). From a standpoint of the training mode effects on the lactate transporters, Evertsen et al., 2001 reported that interval training maintained the concentration of MCT1, while its concentration decreased after continuous training. It was concluded that the enhanced ability to take up lactate by the trained muscles was due to the increase in MCT1 transporters (Bonen, 2000). It is well established that the concentration of MCT1 increases by chronic stimulation or intensive training; while less intensive training may have little effect on human skeletal muscle MCT1 (Pilegaard et al., 1999). Consequently, IT-group with the highest intensity compared to CT-group would be expected to display the highest exchange and removal lactate abilities.
Despite the difference in training mode we found a similarity between t-[La]peak and [La]peak in the two trained groups. This might be related to the fact, as mentioned in the methods sections, that blood sampling was not continuous, and therefore we could not determine the exact time or the accurate concentration of the peak lactate level in any of our subjects. Yet, measuring lactate continuously is not easy to implement and the previous studies used such an intermittent sampling method used in the present study.
Conclusion
In conclusion, we investigated the differences in lactate exchange and removal abilities following intermittent and continuous physical training by applying a biexponential model. The main findings of the present study suggest that intermittent training was more effective in elevating MAS and raising the lactate exchange (γ1) and removal (γ2) abilities. However, both continuous and intermittent training were equally effective in t-[La]peak and [La]peak.
Biographies
Adnene Gharbi
Employment
Associate, High Institute of Sport and Physical Education, South Univ., Gafsa, Tunisia.
Degree
PhD
Research interests
Exercise and training induced metabolic changes.
E-mail: adnenegharbi@yahoo.fr
Karim Chamari
Employment
National Center of Medicine and Sciences in Sports (CNMSS), El Menzah, Tunisia.
Degree
PhD
Research interests
Exercise and sports performance training and testing.
E-mail: karimchamari@gmx.net
Amjad Kallel
Employment
Associate Professor, ISSTEG University Gabes-Tunisia.
Degree
PhD
Research interests
Environnement interest.
E-mail: kalamj@hotmail.com
Saîd Ahmaidi
Employment
Professor, Faculty of Sports Sciences, Picardie University, Amiens, France.
Degree
PhD
Research interests
Exercise training, recovery, adaptations and rehabilitations.
E-mail: said.ahmaidi@u-picardie.fr
Zouhair Tabka
Employment
Professor, Faculty of Medicine Ibn El Jazzar, Sousse, Tunisia.
Degree
PhD
Research interests
Exercise induced cardio-circulatory, respiratory, metabolic and hormonal changes.
E-mail: zouhair.tabka@rns.tn
Zbidi Abdelkarim
Employment
Director of the Faculty of Medicine Ibn El Jazzar, Sousse, Tunisia.
Degree
PhD
Research interests
Exercise induced cardio-circulatory, respiratory, metabolic and hormonal changes.
REFERENCES
- Bassett D.R., Merrill P.W., Nagle F.J., Sampedro R. (1991) Rate of decline in blood lactate after cycling exercise in endurance-trained and untrained subjects. Journal of Physiology 70, 1816-1820 [DOI] [PubMed] [Google Scholar]
- Billat V., Sirvent P., Lepretre P.M., Koralsztein J.P. (2004) Training effect on performance, substrate balance and blood lactate concentration at maximal lactate steady state in master endurance-runners. European Journal of Physiology 447, 875-883 [DOI] [PubMed] [Google Scholar]
- Billat V., Slawinski J., Bocquet V., Demarle A., Lafitte L., Chassaing P., Koralsztein JP. (2000) Intermittent runs at the velocity associated with maximal oxygen uptake enables subjects to remain at maximal oxygen uptake for a longer time than intense but submaximal runs. European Journal of Applied Physiology 81, 188-196 [DOI] [PubMed] [Google Scholar]
- Bonen A. (2000) Lactate transporters (MCT proteins) in heart and skeletal muscles. Medicine Science Sports and Exercise 32, 778-789 [DOI] [PubMed] [Google Scholar]
- Bret C., Messonnier L., Nouck J M., Freund H., Dufour AB., Lacour J R. (2003) Differences in lactate exchange and removal abilities in athletes specialised in different track running events (100 to 1500 m). International Journal of Sports Medicine 24, 108-113 [DOI] [PubMed] [Google Scholar]
- Chtara M., Chamari K., Chaouachi M., Chaouachi A., Koubaa D., Feki Y., Millet G.P., Amri M. (2005) Effects of intra-session concurrent endurance and strength training sequence on aerobic performance and capacity. British Journal of Sports Medicine 39, 555-560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donovan C.M., Pagliassotti M.J. (2000) Quantitative assessment of pathways for lactate disposal in skeletal muscle fiber types. Medicine Science Sports and Exercise 32, 772-777 [DOI] [PubMed] [Google Scholar]
- Dudley G.A., Abraham W.M., Terjung R.J. (1982) Influence of exercise intensity and duration on biochemical adaptations in skeletal muscle. Journal of Applied Physiology 53, 844-850 [DOI] [PubMed] [Google Scholar]
- Edge J., Bishop D., Dawson B., Goodman C. (2006) The effects of training intensity on muscle buffer capacity in females. European Journal of Applied Physiology 96, 97-105 [DOI] [PubMed] [Google Scholar]
- Edge J., Bishop D., Goodman C., Dawson B. (2005) Effects of High- and Moderate-Intensity Training on Metabolism and Repeated Sprints. Medicine Science Sports and Exercise 37, 1975-1982 [DOI] [PubMed] [Google Scholar]
- Evertsen F., Medbo J.I., Bonen A. (2001) Effect of training intensity on muscle lactate transporters and lactate threshold of cross- country skiers. Acta Physiologica Scandinavica 173, 195-205 [DOI] [PubMed] [Google Scholar]
- Fell J.W., Rayfield J.M., Gulbin J.P., Gaffney P.T. (1998) Evaluation of the Accusport Lactate Analyzer. International Journal of Sports Medicine 19, 199-204 [DOI] [PubMed] [Google Scholar]
- Freund H., Gendry P. (1978) Lactate kinetics after short strenuous exercise in man. European Journal of Applied Physiology 39, 123-135 [DOI] [PubMed] [Google Scholar]
- Freund H., Lonsdorfer J., Oyono-Enguelle S., Lonsdorfer A., Bogui P. (1992) Lactate exchange and removal abilities in sickle cell patients and in untrained and trained healthy humans. Journal of Applied Physiology 73, 2580-2587 [DOI] [PubMed] [Google Scholar]
- Gmada N., Bouhlel E., Mrizek I., Debabi H., Ben Jabrallah M., Tabka Z., Feki Y., Amri M. (2005) Effect of combine active recovery from supramaximal exercise on blood lactate disappearance in trained and untrained man. International Journal of Sports Medicine 26, 1-6 [DOI] [PubMed] [Google Scholar]
- Gorostiaga E.M., Walter C.B., Foster C., Hickson R.C. (1991) Uniqueness of interval and continuous training at the same maintained exercise intensity. European Journal of Applied Physiology 63, 101-107 [DOI] [PubMed] [Google Scholar]
- Juel C., Klarskov C., Neilsen J.J., Krustrup P., Mohr M., Bangsbo J. (2004) Effect of high-intensity intermittent training on lactate and H+ release from human skeletal muscle. American Journal of Physiology 286, E245-251 [DOI] [PubMed] [Google Scholar]
- Laffite L.P., Mille H.K., Billat V.L. (2003) The effects of interval training on oxygen pulse and performance in supra-threshold runs. Archives of Physiology & Biochemistry 111, 202-210 [DOI] [PubMed] [Google Scholar]
- Mayes R., Hardman A.E., William C. (1987) The influence of training on endurance and blood lactate concentration during submaximal exercise. British Journal of Sports Medicine 21, 119-124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLellan T.F., Skinner J.C. (1982) Blood lactate removal during recovery related to the aerobic threshold. International Journal of Sports Medicine 3, 224-229 [Google Scholar]
- Messonnier L., Freund H., Denis C., Féasson L., Lacour JR. (2006) Effects of training on lactate kinetics parameters and their influence on short high-intensity exercise performance. International Journal of Sports Medicine 27, 60-66 [DOI] [PubMed] [Google Scholar]
- Messonnier L., Freund H., Féasson L., Prieur F., Castells J., Denis C., Linossier MT., Geyssant A., Lacour JR. (2001) Blood lactate exchange and removal abilities after relative high-intensity exercise: effects of training in normoxia and hypoxia. European Journal of Applied Physiology 84, 403-412 [DOI] [PubMed] [Google Scholar]
- Oosthuyse T., Carter RN. (1999) Plasma lactate decline during passive recovery from high intensity exercise. Medicine Science Sports and Exercise 31, 670-674 [DOI] [PubMed] [Google Scholar]
- Oyono-Enguelle S., Freund H., Lampert E., Lonsdorfer A., Lonsdorfer J. (1993) Modeling lactate kinetics during recovery from muscular exercise in human. 1. Inluence of some physiological factors. Science & Sports 8, 181-187 [Google Scholar]
- Pilegaard H., Domino K., Noland T., Juel C., Hellsten Y., Halestrap AP., Bangsbo J. (1999) Effect of high-intensity exercise training on lactate/H+ transport capacity in human skeletal muscle. American Journal of Physiology 276, E255-E261 [DOI] [PubMed] [Google Scholar]
- Poole D.C., Gaesser G.A. (1985) Response of ventilatory and lactate thresholds to continuous and interval training. Journal of Applied Physiology 58, 1115-1121 [DOI] [PubMed] [Google Scholar]
- Slawinski J., Demarle A., Koralsztein J.P., Billat V. (2001) Effect of supra-lactate threshold training on the relationship between mechanical stride descriptors aerobic energy cost in trained runners. Archives of Physiology & Biochemistry 109, 110-116 [DOI] [PubMed] [Google Scholar]
- Tabata I., Irisawa K., Kouzaki M., Nishimura K., Ogita F., Miyachi M. (1997) Metabolic profile of high-intensity intermittent exercises. Medicine Science Sports and Exercise 29, 390-395 [DOI] [PubMed] [Google Scholar]
- Thomas C., Perrey L., Hugon K.G., Mornet D., Mercier J. (2005) Monocarboxylate transporters, blood lactate removal after supramaximal exercise, and fatigue indexes in humans. Journal of Applied Physiology 98, 804-809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weltman A., Seip R., Snead D., Weltman J.Y., Haskvitz E.M., Evans W.S., Ve.ldhuis JD., Rogol A.D. (1992) Exercise training at and above the lactate threshold in previously untrained women. International Journal of Sports Medicine 13, 257-263 [DOI] [PubMed] [Google Scholar]