

Abstract
We measured physiological responses of elderly recreational skiers of different fitness and skiing abilities. Six subjects (mean age: 61.2 ± 4.6 yrs; Wt: 76.8 ± 15.6 kg; Ht: 1.69 ± 0.10 m; BMI: 26.9 ± 5.0) were tested in a laboratory and during 30 and 75 min of recreational downhill skiing. Oxygen uptake (VO2), heart rate (HR), blood lactate (LA) concentration, and diastolic (DBP) and systolic (SBP) blood pressure were used to estimate energy demands while skiing. During maximal testing in a laboratory, subjects achieved a mean maximal VO2max of 28.2 ± 7.5 ml.kg-1.min-1 and a mean HRpeak of 165 ± 4 bpm (98 ± 1% of HRmax). Mean maximal workload measured on a cycle ergometer was 2.2 ± 0.7 W.kg-1 with a mean LApeak of 7.4 ± 1 mmol.l-1. During field testing, mean VO2 during skiing was 12 ± 2 ml.kg-1.min-1 (45 ± 16% of VO2max). Skiing VO2peak was 19 ± 5 ml. kg-1.min-1 (72 ± 23% of VO2max) was lower than VO2max in the lab (p = 0.04). Mean HR during skiing was 126 ± 2 bpm (77 ± 1% of HRmax from lab tests). Skiing HRpeak was 162 ± 2 bpm. This was not different from HRmax in the lab (p = 0.68). Mean LA after 30 and 75 min of skiing was not different (2.2 ± 0.8 mmol.l-1 and 2.0 ± 0.8, respectively, p = 0.71). Both LA samples during skiing were lower than lab tests (p < 0.0001). There was no difference for DBP between field and laboratory tests; however, SBP increased after 30 min of skiing to 171 ± 20 (p < 0.009) and 165 ± 17 (p < 0.003) after 75 min. These remained below the mean peak SBP determined in lab tests (218+31). Mean oxygen demand during 30 and 75 min of recreational skiing is only 45% of VO2max while mean HR is 77% of HRmax. This departure from linearity not often seen in typical aerobic activities suggests that alpine skiing requires a combination of aerobic and anaerobic activity. Blood LA remained low during skiing suggesting that elderly skiers may govern their intensity via signals closer to VO2 and LA compared to HR or BP.
Key points.
Recreational Alpine skiing for elderly population does not pose health risks
Blood pressure and heart rate during recreational Alpine skiing is retain within normal limits
Blood lactate levels remain relatively low and do not contribute to fatigue
Oxygen uptake and blood lactate are better markers of intensity in elderly Alpine skier compared to heart rate and blood pressure.
Key words: Elderly, physiological responses, blood lactate, blood pressure
Introduction
Numerous media outlets publicize alpine skiing as a predominantly fun and adventurous sport (Bässler, 1996). Skiing has been recommended as an appropriate activity for physically fit and healthy populations. It has also been labeled a risky, injury prone activity, especially for the elderly and physically unfit individuals (Brügmann, 1974; Hollmann and Hettinger, 2000; Phlippen et al., 1970; Prokop and Bachl, 1984). However, the alpine skiing public is not only limited to young, healthy, fit generations; it often includes less fit individuals and a growing number of elderly recreational alpine skiers (Bässler, 1996; Hansen, 2002; Lamprecht und Stamm, 2001).
Much of the research in alpine skiing has focused on ski racing and the associated changes in physiological demands or energy expenditure for successful ski racing and/or was designed to assess performance, training status, capacities and abilities of individuals or groups of alpine ski racers (Andersen and Montgomery, 1988; Bacharach and von Duvillard, 1995; Cortili at al. 1984; Tesch et al., 1978; Tesch, 1995; Veicsteinas et al. 1984; von Duvillard et al., 2009). Based on general conclusions from studies with elderly populations (Burtscher et al., 2000; 2005; Burtscher, 2004; 2007; Brügmann, 1974, Faulhaber et al., 2007, Hollmann and Hettinger, 2000; Kahn and Jouanin, 1996, Phlippen et al., 1970; Prokop and Bachl, 1984) changes in cardiovascular responses to physical exertion may warrant medical attention prior to engaging in such activities. Acute changes possible during alpine skiing include increased blood pressure (BP), greater oxygen uptake (VO2) and higher percentage of peak heart rate (HRpeak) at submaximal levels.
Therefore, the purpose of this study was to measure physiological responses in a group of elderly individuals having different skiing abilities and different fitness levels, first in a laboratory setting and then during recreational alpine skiing in hopes of demonstrating recreational alpine skiing is not only an activity for a healthy, physically fit, younger population.
Methods
This study was approved by the local ethics committee and a written informed consent was obtained from all participants prior to all testing.
Subjects
Six (3 male and 3 female) subjects (mean age: 61.2 ± 4.6 yrs; weight: 76.8 ± 15.6 kg; height: 1.69 ± 0.10 m; BMI: 26.9 ± 5.0) completed a single maximal laboratory test on an electronically braked cycle ergometer and on a separate day a 75 min recreational alpine skiing field test.
Subjects varied in skiing ability ranging from low to high intermediate level and were classified according to the Austrian Ski Teaching Concept 2007 (Wörndle, 2007). Participants documented a wide range of skiing days per year but not less than seven days per year and started to ski on an average age of 9 yrs, thus, subjects were skiing a total of 49 ± 10 years.
Laboratory test
Subjects completed a single incremental cycle test on an electronically braked cycle ergometer to volitional fatigue (Ergoline, Ergoselect, Reiner, Austria). The cycle ergometer test started with a workload of 50 W followed by a 25 W increase every 3 min until exhaustion. Heart rate (HR) beats per minute (bpm) was measured and recorded continuously via 12-lead ECG (Cardio Soft, Marquette, Hellige, Germany). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured via ascultatory method (MPÖ Konstante II, FB, Bosch Medizintechnik, Germany) at the end of each increment. Respiratory gas exchange measures were assessed via an open-air spirometry system (Masterscreen CPX, Jäger, Germany) for determination of selected respiratory gas exchange measures of maximal oxygen uptake (VO2max), carbon dioxide production (VCO2), and pulmonary ventilation (VE). All subjects reached the criteria for VO2max (plateau in VO2 at volitional exhaustion and an increase in VCO2 associated with hypercapnic activity). Additionally, blood lactate concentration (LA) was measured at rest, at the end of every increment and at the end of the maximal effort via fully enzymatic amperometric analysis instrument (EBIO Plus, Eppendorf, Germany).
Throughout this manuscript, maximal laboratory values are compared to peak field test data and reported at percentages of max and peak data to associate physiological demand of our elderly subjects during recreational alpine skiing to their maximal efforts performed in the lab.
Field test
Subjects participated in a total of ~ 75 min of alpine skiing on slopes of the Maiskogel in Kaprun, Salzburg, Austria at an altitude of 1128-1730 m. Subjects resided at various altitudes ranging from 300-800 m and did not appear to be limited in their ability to ski at these latitudes.
The ski slopes consisting of < 25 % to < 40 % grade were used for testing and were serviced by a chair lift that required approximately 12 min for a subject to arrive at the top of the testing area. The weather conditions were sunny and temperature throughout testing days was consistent ranging between -2°C in the mornings to +10°C in the afternoons.
Participants were requested to ski at their normal speed using their preferred technique, stopping to rest and thus skiing at their own self selected pace.
To familiarize the subjects with the portable metabolic measurement system (Cosmed, K4b2, Rome, Italy), each subject was asked to ski one preliminary run with the respiratory gas exchange measuring equipment while wearing the respiratory gas exchange mask. This familiarization run also served as a warm-up and to obtain knowledge of slopes, snow conditions, and environmental conditions that were present for subsequent testing.
Each subject’s HR and respiratory gas exchange data were monitored continuously during 75 min of alpine skiing. Raw data for VO2 were filtered using a moving average of 15 breaths to eliminate non physiological spikes. Both HR and VO2 responses during skiing were quantified with average and peak values during downhill-runs. Due to various logistical reasons, the use of different metabolic measurement systems between laboratory tests (Masterscreen CPX, Jäger, Germany) and field tests (Cosmed, K4b2, Rome, Italy) were used. Reported validity and reliability measures of 3-5% for each system are well within the expected variance of these data.
Measures for BP (Omron, RX Classic, Mannheim, Germany) and LA (EKF, Biosen 5040, Magdeburg, Germany) were measured twice after downhill-runs. Recordings for BP were conducted immediately after downhill-runs at 30 min of skiing and the again after 75 min of skiing. Blood LA was measured approximately 1 min after downhill-runs at 30 and 75 min of skiing, respectively.
Statistical analyses
Statistical significance was set at p < 0.05. All statistical calculations (means ± standard deviations), t-tests for maximal values obtained in the laboratory and peak values measured during on snow skiing. An analysis of variance (ANOVA) was performed using data from the laboratory, 30 min and 75 min of testing. Each time interval chosen was used to compare energy demands of early to late recreational skiing. Statistical analysis was conducted with SigmaStat version 3.5 software (Systat, Richmond, California, USA).
Results
Laboratory test
Table 1 shows individual data and group means (±SD) for maximal HR (HRmax), maximal VO2 (VO2max), workload and maximal blood LA (LAmax) measured during the ergometry test. Resting mean SBP/DBP was 126/79 mmHg and at exhaustion, it increased to 217/86 mmHg.
Table 1.
Physiological characteristics of subjects during cycle ergometry in laboratory tests.
| Subject | HRmax (bpm) |
VO2max (ml.kg-1.min-1) |
Peak LA (mmol.l-1) |
Workload max (W.kg-1) |
|---|---|---|---|---|
| 1 | 162 | 33.5 | 8 | 2.6 |
| 2 | 158 | 22.1 | 9 | 1.8 |
| 3 | 167 | 27.6 | 6.2 | 1.9 |
| 4 | 165 | 39.6 | 7.3 | 2.9 |
| 5 | 167 | 27.3 | 6.6 | 2.7 |
| 6 | 169 | 19.1 | 7.5 | 1.2 |
| Mean (±SD) | 165 (4) | 28.2 (7.5) | 7.4 (1) | 2.2 (0.7) |
Field test
Mean and peak absolute and relative HR data are shown in Table 2. Participants reached a mean HR during downhill skiing of 126 ± 15 bpm or 77 ± 9% (range 64-91%) of HRmax. Peak HR was 162 ± 15 bpm that corresponded to 98 ± 8% (range 87-113%) of HRmax and a comparison between lab and field values were not different (p = 0.68).
Table 2.
Mean and peak absolute and relative HR data (±SD) during downhill skiing.
| Subject | Mean HR absolute (bpm) |
Mean HR relative (% of HRmax) |
Peak HR absolute (bpm) |
Peak HR relative (% of HRmax) |
|---|---|---|---|---|
| 1 | 120 (4) | 74 (2) | 164 (7) | 101 (5) |
| 2 | 118 (6) | 75 (4) | 156 (9) | 99 (6) |
| 3 | 108 (3) | 64 (2) | 148 (12) | 89 (7) |
| 4 | 126 (4) | 80 (3) | 155 (6) | 94 (4) |
| 5 | 128 (4) | 76 (3) | 158 (9) | 95 (6) |
| 6 | 153 (1) | 90 (1) | 191 (8) | 113 (5) |
| Mean (±SD) | 126 (15) | 77 (9) | 162 (15) | 99 (8) |
The mean VO2peak for subjects during skiing was 19 ± 5 ml.kg-1.min-1 (72 ± 23% of VO2max) and this was significantly lower than VO2max measured in the lab (p = 0.04). Mean VO2 during skiing was 12 ± 2 ml.kg-1.min-1 (45 ± 16% of VO2max) (Table 3) ranging between 30-66% of VO2max for the entire group.
Table 3.
Mean and peak relative VO2 and %VO2max data (±SD) during downhill skiing.
| Subject | VO2 mean (ml.kg-1.min-1) |
VO2 mean (% of VO2max) |
VO2 peak (ml.kg-1.min-1) |
VO2 peak (% of VO2max) |
|---|---|---|---|---|
| 1 | 10 (1) | 30 (4) | 16 (2) | 47 (4) |
| 2 | 12 (2) | 55 (9) | 20 (1) | 88 (5) |
| 3 | 9 (1) | 31 (4) | 16 (2) | 56 (6) |
| 4 | 13 (1) | 34 (3) | 20 (1) | 51 (3) |
| 5 | 15 (1) | 56 (4) | 28 (2) | 100 (7) |
| 6 | 13 (1) | 67 (3) | 17 (0) | 88 (1) |
| Mean (±SD) | 12.0 (2.2) | 45.5 (15.8) | 19.5 (4.5) | 71.8 (23.1) |
Blood LA measured one min after 30 and 75 min of downhill skiing ranged between 1.0-3.0 mmol.l-1 (Table 4). No differences were noted between LA at 30 min (2.2 ± 0.8 mmol.l-1) and 75 min (2.0 ± 0.8 mmol.l-1) of skiing (p = 0.74); however, both of these values were significantly lower than peak LA values from the lab tests (p < 0.0001) (Figure 1).
Table 4.
Blood lactate (LA) and systolic blood pressure (SBP) values at 30 min and 75 min of skiing.
| Subject | LA at 30 min (mmol.l-1) |
LA at 75 min (mmol.l-1) |
SBP at 30 min (mm Hg) |
SBP at 75 min (mm Hg) |
|---|---|---|---|---|
| 1 | 1.47 | 1.06 | 179 | 176 |
| 2 | 2.13 | 2.03 | 180 | 173 |
| 3 | 1.15 | 1.01 | 180 | 173 |
| 4 | 2.65 | 2.42 | 155 | 140 |
| 5 | 3.04 | 2.98 | 193 | 179 |
| 6 | 2.72 | 2.65 | 138 | 146 |
| Mean (±SD) | 2.2 (.8) | 2.0 (.8) | 167.3 (21.8) | 161.3 (17.6) |
Figure 1.
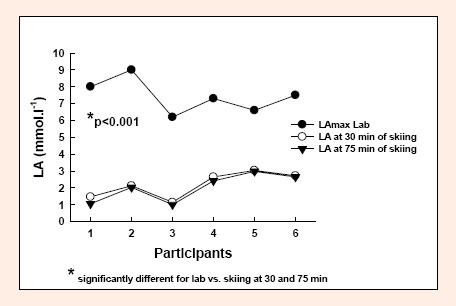
Peak blood lactate values between laboratory test and 30 and 75 min of skiing. Laboratory test values were significantly higher than blood lactate measured during skiing (p<0.001).
Table 4 also shows BP values recorded twice while skiing. Average BP values measured immediately after downhill skiing for the group were similar at 30 and 75 min of skiing (p > 0.05). Compared to lab test data, SBP at 30 min of alpine skiing was lower than peak SBP in the lab test (p = 0.009) while DBP was not different (p > 0.05). Similar results were recorded at 75 min of alpine skiing where SBP was also lower than peak SBP in the lab tests (p = 0.003), while DBP was not different (p > 0.05).
Discussion
Laboratory tests
With a workload range between 1.2-2.9 W.kg-1 at exhaustion, a wide range of fitness level was evident in this group of elderly skiers. Similar results were also observed for VO2max values, which ranged between 19-40 ml.kg-1.min-1. Thus, it is important to note the heterogeneity of this group of elderly alpine skiers.
Field tests
In general, alpine skiing may be classified as an intermittent activity (Scheiber et al., 2009, Zintl and Eisenhut, 2001) that requires both aerobic and anaerobic demands. This is supported by data for single downhill skiing runs. Time to complete one run ranged from 2.8 min for better skiers to ~20 min for less skilled skiers. This adds additional support to the notion that these subjects represent a wide range of skiing abilities and levels of fitness often seen in the alpine skiing public.
Mean HR during downhill runs ranged between 64-91% of HRmax. Kahn et al., 1993 reported values between 70-78% of HRmax. Similar data for mean HR during recreational alpine skiing in elderly were reported by Krautgasser et al., 2009 and Scheiber et al., 2009.
Peak HR during alpine skiing ranged between 87-113% of HRmax for the elderly subjects in this study. Peak HR values for young alpine ski racers have been reported during competition to have a similar range (Anderson and Montgomery, 1988; Tesch, 1995). For some subjects peak HR values during downhill skiing exceeded maximal values recorded at exhaustion in the laboratory test. These high peak HR values may be the result of an increase in static loading of the lower extremities as a result of isometric contraction during ski turns in comparison to the dynamic movement exhibited during the cycle ergometer test (Cortili et al., 1984; Hollmann and Hettinger, 2000).
Individual VO2 values during downhill skiing ranged from 30-66% of VO2max and were similar to the VO2 range reported by Scheiber et al., 2009 in a guided group of elderly recreational skiers. The VO2peak values in our group of elderly skiers ranged from 47-100% of VO2max. Different percentages of VO2max measured during the lab tests were observed during skiing. Subjects with the lowest VO2max value showed the highest meanVO2 response during skiing. It is difficult to determine the relationship of low physical fitness with elevated skiing demands due to the influence of various internal and external factors on skiing performance (Krautgasser et al., 2009); however, it may be reasonable to assume that all subjects require a similar level of aerobic capacity to successfully perform the skiing task of this study. Those subjects with a low aerobic capacity required a greater percentage of that capacity to ski for 75 min, hence a higher mean VO2 for subjects with a lower VO2max.
Blood LA have been recorded under many different conditions for alpine skiing. von Duvillard et al., 2009 reported mean blood LA concentrations measured at peak exercise in laboratory tests of 13.7 mmol.l-1 and 3 min after GS on-snow training run of only 5.6 mmol.l-1. Anderson and Montgomery (1988) reported blood LA values of 9.0-13.0 mmol.l-1 in a group of young elite ski racers after slalom and giant slalom competition. Tesch et al., 1978 analyzed muscle fiber lactate accumulation and reported LA values of 12.0 mmol.l-1 and higher after a giant slalom ski race. This suggests that alpine skiing and ski racing appears to be an intermittent activity of moderately high intensity and thus, energy production depends greatly on both aerobic and anaerobic energy sources that result in substantial blood LA production.
For the elderly subjects in this study, all blood LA values remained between 1.0-3.0 mmol.l-1 at 30 and 75 min of recreational alpine skiing. Scheiber et al., 2009 who studied nine skilled and experienced older alpine skiers found LA value ranging from 0.7 and 6.0 mmol.l-1 during guided skiing. Subjects in the study of Scheiber et al., 2009 were very well skilled and had to perform defined skiing patterns that could have easily resulted in higher LA values compared to LA values of skiers in this study. With a wide range of intermediate skiing abilities and a self determined pace and intensity, it would not be too unexpected to record LA values in the range seen here.
The current group of recreational skiers who skied for 75 min are not comparable to young alpine racers or to older more advanced ability skiers such as the ones used by Scheiber et al., 2009. These current data do however reflect an intermittent character of activity during downhill skiing in spite of having relatively low blood LA values. Whether this low LA is a result of technical abilities of our elderly recreational skiers or a product of the skiing protocol allowing subjects to self regulate their skiing pace, cannot be determined.
Blood pressure was recorded immediately after downhill skiing for 30 and 75 min. Mean SBP measured right after skiing remained below maximal levels for all subjects. These results are in agreement with Scheiber et al., 2009 who also reported submaximal BP levels in a guided group of elderly skiers after downhill runs.
Conclusion
It is quite evident that alpine skiing requires both aerobic and anaerobic capacities. It also appears that during 75 min of recreational skiing by older intermediate level skiers, the oxygen demand ranged from 40-50% of VO2max while at the same time HRs range from 70-80% of peak HR. When compared to typical aerobic activity of elderly, such as walking or cycling, there seems to be a greater demand on HR versus VO2; yet, given blood LA remained low during skiing, elderly skiers may govern their intensity via signals more closely in tune to VO2 and blood LA rather than HR or BP. Limitations of this study included a small number of subjects and each subject was allowed to control his/her own skiing intensity and duration. The intermittent character of alpine skiing allowed individuals to tailor their skiing with regard to personal health and physical capacity. The chosen skiing slopes and their characteristics, the frequency and length of downhill runs, the elected speed and resulting technique all needed to be synchronized to individual skiing skill level. This, in concert with their physical capacity, was chosen to achieve an optimal skiing intensity while also providing an enjoyable experience for the subjects. This however could have limited the potential for finding differences in physiological demands of the skiers.
Biographies

Sabine Krautgasser
Employment
Christian Doppler Laboratory, Biomechanics in Skiing, Department of Sport Science and Kinesiology, University of Salzburg, Salzburg, Austria
Degree
MS
Research interests
Alpine skiing, biomechanics.

Peter Scheiber
Employment
Christian Doppler Laboratory, Biomechanics in Skiing, Department of Sport Science and Kinesiology, University of Salzburg, Salzburg, Austria
Degree
PhD
Research interests
Alpine sking and biomechanics.

Serge P. von Duvillard
Employment
Visiting Professor
Degree
PhD
Research interests
Exercise physiology, exercise biochemistry, training studies, cardiac rehabilitation.
E-mail: serge.duvillard@sbg.ac.at

Erich Müller
Employment
The University of Salzburg, Vice President for Education
Degree
PhD
Research interests
Biomechanics, training sciences
References
- Andersen R.E., Montgomery D.L. (1988) Physiology of alpine skiing. Sports Medicine 6(4), 210-221 [DOI] [PubMed] [Google Scholar]
- Bacharach D.W., von Duvillard S.P. (1995) Intermediate and long-term anaerobic performance of elite alpine skiers. Medicine and Science in Sports and Exercise 27(3), 305-309, 1995 [PubMed] [Google Scholar]
- Bässler R. (1996) Projekt: Bewegung am Berg. Skifahren Alpin. Bericht über die Sekundäranalyse und sonstige Befunde. Studie im Auftrag des Fachverbandes für Seilbahnen Österreichs, Wien; (In German). [Google Scholar]
- Burtscher M., Pachinger O., Mittleman M.A., Ulmer H. (2000) Prior myocardial infarction is the major risk factor associated with sudden cardiac death during downhill skiing. International Journal of Sports Medicine 21(8), 613-615 [DOI] [PubMed] [Google Scholar]
- Burtscher M. (2004) Endurance performance of the elderly mountaineer: requirements, limitations, testing, and training. Wiener Medizinische Wochenschrift 116(21-22), 703-714 (In German: English abstract). [DOI] [PubMed] [Google Scholar]
- Burtscher M., Faulhaber M., Kornexl E., Nachbauer W. (2005) Cardirespiratory and metabolic responses during mountain hiking and downhill skiing. Wiener Medizinische Wochenschrift, 155(7-8), 129-135 (In German: English abstract) [DOI] [PubMed] [Google Scholar]
- Burtscher M. (2007) Risk of cardiovascular events during mountain activities. Advances in Experimental Medicine and Biology 618, 1-11 [DOI] [PubMed] [Google Scholar]
- Buskies W. (1997) Zur Wahl der richtigen Belastungsintensität im gesundheitssportlich orientierten Ausdauertraining. In: Sport im Lebenslauf. Schmidbleicher D., Bös K., Müller A. (Hrsg.) Hamburg: 279-280 (In German). [Google Scholar]
- Brügmann E. (1974) Sport für ältere Menschen. Goldmann Publishers, München, Das wissenschaftliche Taschenbuch.Abteilung; Medizin: 40 (In German). [Google Scholar]
- Cortili G., Gavazzi P., Magistri P., Saibene F. (1984) Energy Sources in Alpine Skiing. In: Current Topics in Sports Medicine- Proceedings of the World Congress of Sports Medicine, Vienna 1982, Wien. Eds: Bachl N., Prokop L., Suckert R. Urban und Schwarzenberg; 506-510 [Google Scholar]
- Faulhaber M., Flatz M., Gatterer H., Schobersberger W., Burtscher M. (2007) Prevalence of cardiovascular diseases among alpine skiers and hikers in the Austrian Alps. High Altitude Medicine and Biology 8(3), 245-252 [DOI] [PubMed] [Google Scholar]
- Hansen J. (2002) Gesellschaftliche und demoskopische Rahmenbedingungen. In: Deutscher Sportbund, Referat. Grundsatzfragen, Wissenschaft und Gesellschaft(Hrsg.), Einheit in der Vielfalt. Dokumentation der Workshopreihe zum "Leitbild des deutschen Sports" Frankfurt/Main, Deutscher Sportbund; 175-201 (In German). [Google Scholar]
- Hollmann W., Hettinger T. (2000) Sportmedizin Grundlagen für Arbeit, Training und Präventivmedizin. Stuttgart, New York: Schattauer; (In German [Google Scholar]
- Kahn J.F., Jouanin J.C., Espirito-Santo J., Monod H. (1993) Cardiovascular response to leisure alpine skiing in habitually sedentary middle-aged men. Journal of Sport Sciences 11(1), 31-36 [DOI] [PubMed] [Google Scholar]
- Kahn J.F., Jouanin J.C. (1996) Physiological effects of downhill skiing at moderate altitude in untrained middle-aged men. Wilderness and Environmental Medicine 7(3), 199-207 [DOI] [PubMed] [Google Scholar]
- Krautgasser S., Scheiber P., Kröll J., Ring-Dimitriou S., Müller E. (2009) Influence of physical fitness on individual strain during recreational skiing in the elderly. : Science in Skiing IV. Eds: Müller E., Lindinger S., Stoeggl T. Meyer & Meyer Sport, Maidenhead UK: 310-319 [Google Scholar]
- Lamprecht M., Stamm H. (2001) Sport in der Stadt Zürich. Analysen zum Sportverhalten und zu den Sportwünschen der Stadtzürcher Bevölkerung. Zürich: Sportamt der Stadt Zürich, 2001; (In German). [Google Scholar]
- Phlippen R., Heck H., Grünewald B. (1970). EKG-Langzeituntersuchungen zur Frage der Herzbelastungen beim Ski-Abfahrtslauf im Alter. Medizinische Welt 21/46, 1985 (In German). [PubMed] [Google Scholar]
- Prokop L., Bachl N. (1984) Alterssportmedizin. Springerverlag, Wien: (In German). [Google Scholar]
- Samitz G., Mensink G. (2002) Körperliche Aktivität in Prävention und Therapie. Marseille Verlag, München: (In German). [Google Scholar]
- Scheiber P., Krautgasser S., Kröll J., Müller E. (2009) Guided Alpine Skiing-Physiological demands on elderly recreational skiers. : Science in Skiing IV. Eds: Müller E., Lindinger S., Stoeggl T. Meyer & Meyer Sport, Maidenhead UK: 445-453 [Google Scholar]
- Scheiber P., Krautgasser S., von Duvillard S.P., Müller E. (2009) Physiologic responses of older recreational alpine skiers to different skiing modes. European Journal of Applied Physiology 105(4), 551-558 [DOI] [PubMed] [Google Scholar]
- Shephard R.J. (2004) Aging. : Clinical exercise physiology- application and physiological principles. Eds: LeMura L.M., von Duvillard S.P. Lippincott Wiliams and Wilkins, Philadelphia, Pennsylvania: 549-565 [Google Scholar]
- Tesch P., Larsson L., Eriksson A., Karlsson J. (1978) Muscle glycogen depletion and lactate concentration during downhill skiing. Medicine and Science in Sports and Exercise 10(2), 85-90 [PubMed] [Google Scholar]
- Tesch P.A. (1995) Aspects on muscle properties and use in competitive alpine skiing. Medicine and Science in Sports and Exercise 27(3), 310-314 [PubMed] [Google Scholar]
- Veicsteinas A., Ferretti G., Margonato V., Rosa G., Tagliabue D. (1984) Energy cost of and energy sources for alpine skiing in top athletes. European Journal of Applied Physiology 56(5), 1187-1190 [DOI] [PubMed] [Google Scholar]
- Vater H.H., Nowacki P.E., Röder Y., Vater K.U., Härtel S., Neumann R., Buhl B., Bös K. (2005) Kardiorespiratorische und metabolische Parameter beim Alpinen Skilauf und beim Tourenskilauf einer kombinierten Labor und Feldstudie. Deutsche Zeitschrift für Sportmedizin 56(7/8), 248 (In German). [Google Scholar]
- von Duvillard S.P., Bacharach D.W., Stanek F. (2009) Respiratory and metabolic demands of field versus laboratory test in young competitive alpine ski racers. : Science in Skiing IV. Eds: Müller E., Lindinger S., Stoeggl T. Meyer & Meyer Sport, Maidenhead UK: 543-555 [Google Scholar]
- Wörndle W. (2007) Alpiner Skilauf. : Snowsport Austria - Die österreichische Skischule. Hollinek, Purkersdorf, Austria: 23-88 (In German). [Google Scholar]
- Zintl F., Eisenhut A. (2001) Ausdauertraining. BLV Verlagsgesellschaft, München: (In German). [Google Scholar]