

Abstract
The objectives of this study were to design a field test based on the Conconi protocol to determine the ventilatory threshold of rowers and to test its reliability and validity. A group of sixteen oarsmen completed a modified Conconi test for on-water rowing. The reliability of the detection of the heart rate threshold was evaluated using heart rate breaking point in the Conconi test and retest. Heart rate threshold was detected in 88.8% of cases in the test-retest. The validity of the modified Conconi test was evaluated by comparing the heart rate threshold data acquired with that obtained in a ventilatory threshold test (VT2). No significant differences were found for the values of different intensity parameters i.e. heart rate (HR), oxygen consumption (VO2), stroke rate (SR) and speed (S) between the heart rate threshold and the ventilatory threshold, (170.9 ± 6.8 vs. 169.3 ± 6.4 beats·min-1; 42.0 ± 8.6 vs. 43.5 ± 8.3 ml·kg-1·min-1; 25.8 ± 3.3 vs. 27.0 ± 3.2 strokes·min-1 and 14.4 ± 0.8 vs. 14.6 ± 0.8 km·h-1). The differences in averages obtained in the Conconi test-retest were small with a low standard error of the mean. The reliability data between the Conconi test-retest showed low coefficients of variations (CV) and high intraclass correlation coefficients (ICC). The total errors for the Conconi test-retest are low for the measured variables (1.31 HR, 0.87 VO2, 0.65 SR, and 0.1 S). The Bland- Altman’s method for analysis validity showed a strong concordance according to the analyzed variables. We conclude that the modified Conconi test for on-water rowing is a valid and reliable method for the determination of the second ventilatory threshold (VT2).
Key points.
The Modified Conconi test for on-water rowing is a simple and non-invasive method for the determination of anaerobic threshold for on-water rowing.
The modified Conconi protocol for rowing was also shown to be a valid protocol for the calculation of the second ventilatory threshold using the ventilatory method.
The Bland-Altman analysis suggests an adequate concordance for the modified Conconi test with the ventilatory method for the measurement of the ventilatory threshold.
Key words: Field test, anaerobic threshold heart rate, ventilatory threshold
Introduction
Rowing is considered an endurance sport, where the energy required to cover the 2000m of a regatta is divided approximately into 70% aerobic and 30% anaerobic metabolism (Secher, 1993). It has been demonstrated that in the first 500m of a competition primarily anaerobic metabolism is used. Then up to 1800m, the aerobic metabolism predominates, but in the final 200m anaerobic metabolism again predominates (Nilsen et al., 1993). Anaerobic threshold is a decisive parameter in the performance of a rower.
From Wasserman first definition of anaerobic threshold to the present day, a large amount of research has been carried out on this topic. Currently, it is considered best practice to refer to the anaerobic threshold as aerobic-anaerobic transition, as there is no exact point where the change between aerobic-anaerobic metabolisms occurs. In this way the aerobic threshold corresponds to the first increase of blood lactate, and the anaerobic threshold to the maximal lactate steady state (MLSS) in the blood (Meyer et al., 2005).
However, the latest research shows that the lack of oxygen does not cause a lactate release in the blood. During incremental exercise, it has been proven that there are other factors which may cause increases of lactic acid in the blood such as the activation of the B-adrenergic system.
Various methods exist for the determination of the anaerobic threshold - lactate concentration, gas exchange, and heart rate are variables used to detect the threshold by various methods, with greater or lesser accuracy of the determination. In 1982, Conconi et al., 1982 proposed a method to determine the anaerobic threshold in runners by analysing the relationship between heart rate, running, and velocity. During continuous, incremental exercise, heart rate increases at a linear rate up to a specific point (the point of deflection). At which heart rate deviates from linearity, the so-called point of deflection which was shown to be related to the lactate anaerobic threshold (Conconi et al., 1982). This method has been used in running, cycling, canoeing, rowing, and swimming (Droghetti et al., 1985; Droghetti, 1986; Hofmann et al., 2007). We are not aware of its having been studied in depth with rowers in field conditions and we suggest it is a valid and reliable method for the detection of the anaerobic threshold in on-water rowing.
Doubts have been raised about the Conconi method as a result of either low reproducibility in the detection of the point of deflection of heart rate, or lack of corroboration of the results obtained using other methods, (Francis et al., 1989; Jones and Doust, 1995; 1997; Kara et al., 1996; Kiupers et al., 1988; Nicolaizik et al., 1998; Schmid et al., 1998; Thorland et al., 1994; Vachon et al., 1999). As a result, Conconi et al., 1996 published a follow up of their original contribution (Conconi at al., 1982). Other authors, such as Ballarin et al., 1996, Hofmann et al. (1994; 1997; 2007) and Petit et al., 1997, Ribiero et al. (1985), have demonstrated the validity and reliability of this method for the evaluation of anaerobic threshold. The method has great advantages in that it is non-invasive.
The most frequently used variables to determine the anaerobic threshold in athletes are lactate concentration and gas exchange analysis. Both are proven methods which are usually used to demonstrate the validity of other, newer, methods. The V-slope method developed by Beaver et al., 1986 is based on the relationship between oxygen consumption (VO2) and the production of carbon dioxide (CO2) during continuous and incremental physical activity (respiration quotient). VT1 is defined as the first increase in VE accompanied by an increase in the respiratory equivalent for O2 (VE/VO2). VT2 is defined as an abrupt increase in VE accompanied by an increase in both respiratory equivalents for O2 (VE/VO2) and CO2 (VE/VCO2).
A significant relationship between the VT2 and the maximal lactate steady state (MLSS) has been found by several researchers (Hofmann et al., 1994; Lucia et al., 1999; Wonisch et al., 2003). Hofmann et al., 1994 reported the possibility of determining the intensity of exercise at MLSS by means of the heart rate deflection point.
The aim of the study was to evaluate the validity of the Conconi method modified for on-water rowing in order to determine the anaerobic threshold and to compare it to the second ventilatory threshold (VT2). In addition, reliability of the Heart Rate Threshold was determined by means of a re-test in identical conditions.
Methods
Subjects
Sixteen male lightweight category oarsmen voluntarily participated in the study. They had all been rowing for at least four years and trained 6 days a week for 2 hours per training session. They all competed at national and international levels. The age range was from 19 to 26 years with a mean age of 22.1 ± 2.3. The mean weight, percentage of body fat and height were respectively, 75.8 ±7 .3 kg, 8.8 ± 1.5%, and 1.78 ± 0.04 m.
Data were treated in line with national data protection protocols relating to personal details.
Experimental approach to the problem
This study tried to evaluate the validity and reliability of the modified Conconi test for rowing (dependent variable), compared with the ventilatory method (independent variable). The protocol designed is valid to determinate the anaerobic threshold heart rate (ATHR) and ventilatory thresholds (VT1 and VT2). Although blood lactate is considered the gold standard to determine the anaerobic threshold (AT), this variable cannot be applied in on water rowing without substantial breaks between load steps which will influence the outcome substantially. There are significant changes in the final results due to multiple stops and starts to be performed by the rowers, along with the excessive time required to collect samples of lactic acid. Furthermore, the evaluation of performance in athletes must be as specific as possible.
Procedure
Protocol
The athletes were informed of the nature of the tests and were familiarised with all of the different apparatus to be used. Subjects were required to abstain from any exhausting physical activity in the 48 hours prior to the test or consume any type of stimulant (coffee, tea, colas, nicotine, etc) either the day before or on the day of the test as this could affect the results. The study was performed in accordance with ethical principles for medical research involving human subjects and in accordance with ethical standards (Harris and Atkinson, 2009).
Body mass was obtained using mechanical scales (Shoenle model) with a range of 0 to 150 kg, and an accuracy of 50g for body weight. Height was measured with a Seca anthropometer accurate to 1mm. In addition, Holtain callipers, with an accuracy of 0.5mm were used to measure skin folds to calculate the body fat percentage.
Body fat was determined according to the equation by Whiters et al. (1987). Six skin folds were measured (triceps, subscapular, iliac crest, abdominal, anterior thigh and medial calf).
The procedure we designed to determine the anaerobic threshold heart rate (ATHR) and ventilatory threshold (VT2) was maximal, continuous, incremental and progressive and the test was carried out in a single scull. The test needs to be done on a large body of water of around 4 or 5 km, given that it is a continuous test where the oarsman rows in a straight line for 12 to 15 minutes without interruptions and does not turn the boat. The workload of each stage was determined by stroke frequency and average speed at each stage. Starting stroke rate was set at 18 strokes per minute, and was increased by 2 strokes in each subsequent minute. Average starting speed was established at 12 km·h-1, and increased by 0.5 km·h-1 every minute. Boat speed was calculated as the average speed within a stroke cycle. The boat speed per stroke rate for every load step was calculated in previous unpublished studies. The intensity increase at each stage was adjusted in such a way that the increase in the heart rate of the athletes between consecutive stages was less than 8 beats per minute according to Conconi et al., 1996. The test was stopped when subjects were not able to sustain the imposed rhythm or showed clear signs of exhaustion. The design of the procedure incorporated the latest guidelines proposed by Conconi et al., 1996.
Before the tests all subjects completed a 20 min standardised warm up following the recommendations of Conconi et al., 1996. All tests were conducted at an air temperature of 15-20 ºC, humidity 75-90%, non-windy and on calm water.
In order to assess the reliability of the results, a second test (retest) was conducted with all subjects under the same conditions. The elapsed time between the test and retest was 72 hours in order to ensure complete recovery. Prior to testing each subject, all measuring apparatus was checked.
The VT2 was established as the second linearity break point of VE accompanied by an increase in respiratory equivalents for O2 and CO2 (Figure 1).
Figure 1.
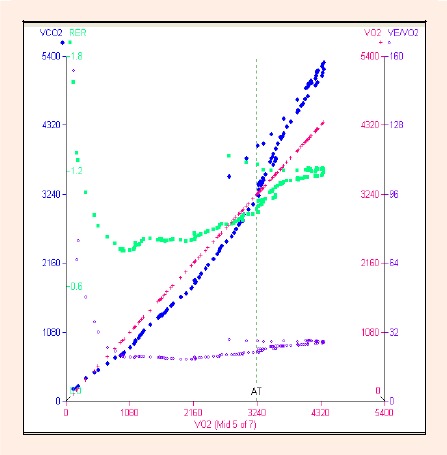
Determination of second ventilatory threshold (VT2) during the on-water rowing test.
The heart rate deflection point was established by means of simple linear regression between heart rate, stroke rate, and average boat speed. Average boat speed (S) and stroke rate (SR) served as progression criteria of the test and indicators of the same (Figure 2).
Figure 2.
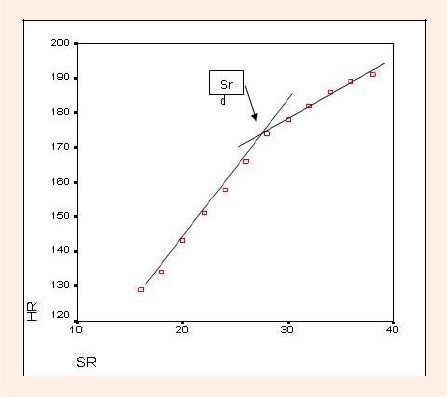
Determination of anaerobic threshold heart rate (ATHR) during the on-water rowing test.
Gas exchange was measured with a VO 2000 Portable Metabolic System gas analyzer (Medical Graphics, St. Paul, MN). This analyzer can be carried in a backpack by the athlete during the test. This equipment measures micro-samples of expired gases using the respiratory cycle method (Breath by breath). Among the parameters, which this apparatus can determine, are: oxygen consumption (VO2), carbon dioxide production (VCO2), minute ventilation (VE), heart rate (HR), respiratory exchange ratio (RER), ventilatory equivalent for oxygen production (VE/VO2), ventilatory equivalent for CO2 production (VE/VCO2) and metabolic equivalents (METS). The portable analyzer was prepared and calibrated with gases of known concentration according to the manufacturer’s instructions.
A Polar S-810 Sport Tester heart rate monitor (Polar Electro, Kempele, Finland) was also used and encoded for use with the gas analyzer which enabled heart rate to be shown directly on the computer screen and integrated with the other respiratory parameters.
The speed of the boat required in each stage of the test was determined using an eTrex Summit GPS system (Garmin International Inc). This instrument has a receptor with 12 channels in parallel, and a positioning accuracy lower than 15 m, and a speed accuracy of 0.05 m·sec-1. (see detail at http://www8.garmin.com/specs/ eTrex_spec_sheet_0105.pdf)
Statistical analysis
All data are described as means and Standard Deviation (SD). Dispersion diagrams were used to analyse the degree and type of dependency between the different variables. If linear relationships were observed between variables, correlation coefficients were calculated to determine the degree of intensity.
Linear regressions using the variables SR-HR and S-HR for each athlete were carried out to determine heart rate deflection point in the Conconi test on water.
The Kolmogorov-Smirnov test was used in order to check the normal distribution of the studied variables. The equality between the means, pair test-retest (to analyze the possible systematic bias), was compared by using the usual paired T-test. In addition, coefficient of variation (CV) was used in order to assess within-subject variation. The retest correlation is calculated by the intraclass correlation coefficients (ICC). Bland-Altman plots are carried out in order to check the reliability of the test. Finally, validity was determined by the application of a Bland-Altman analysis (Bland and Altman, 1986) and a Passing-Bablok regression (Passing and Bablok, 1983).
Test-retest relationship was evaluated following the issues indicated in Atkinson and Nevill (Atkinson and Nevill, 1998). Statistical analysis was conducted using the free software R.2.10 (www.r-project.org).
Results
All variables were normally distributed. The Pearson’s correlation coefficient obtained between the variables HR-SR and HR-S in the on-water Conconi test were 0.96 and 0.97 respectively, indicating a strong direct linear correlation between heart rate and stroke rate, as well as heart rate and boat speed.
The results of two oarsmen were excluded from the second part of the study as the point of deflection was not seen for either athlete.
No significant differences were observed between the variables HR, VO2, %VO2 max, SR and S when comparing data from the VT2 and ATHR. ATHR was found at 92% of HRmax and 73.7% of VO2 max (Table 1). The mean differences between VO2, SR and S at the ATHR and the VT2 were only 2.5%, 3% and 2% respectively.
Table 1.
Means (±SD) for heart rate (HR) oxygen consumption (VO2), percentage of maximal oxygen consumption (%VO2 max), stroke rate (SR), boat speed (S) at ventilatory threshold (VT), anaerobic threshold heart rate (ATHR) and maximal (Max) data during on-water Conconi testing.
| N = 16 | HR (beats/min) | VO2 (ml/kg/min) | % VO2max | SR | S (Km/h) |
|---|---|---|---|---|---|
| ATHR | 170.9 (6.8) | 42.0 (8.6) | 73.7 (9.4) | 25.8 (3.3) (77%) | 14.4 (.8) (89%) |
| VT2 | 169.3 (6.4) | 43.5 (8.3) | 76.2 (8.6) | 27.0 (3.2) (80%) | 14.6 (.8) (91%) |
| Max | 186.6 (7.5) | 57.2 (10.4) | 100 | 33.5 (3.0) (100%) | 16.1 (.8) (100%) |
Table 2 shows some statistics related to the reliability of the modified Conconi test for on-water rowing. As argued in the reliability analysis, the data can be assumed as homoscedastic (four absolute correlations lower than 0.2).
Table 2.
Data (n = 16) for Passing-Bablok regression.
| Test | Retest | Paired T-test | CV | ICC* (Single rating) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean (±SD) | (±SE) | Mean (±SD) | (±SE) | Differences (±SD) | p-value | (%) | ||
| HRCT | 170.9 (6.9) | 1.72 | 172.3 (6.7) | 1.68 | -1.37 (5.23) | .310 | 2.19 | .704 (.34 - .88) |
| VO2CT | 42.1 (8.6) | 2.15 | 45.0 (8.0) | 1.99 | -2.93 (3.49) | .004 | 6.25 | .862 (.43 -. 95) |
| SRCT | 25.9 (3.3) | .83 | 26.4 (2.8) | .69 | -.50 (2.58) | .450 | 7.37 | .645 (.24 - .86) |
| SCT | 14.4 (.8) | .20 | 14.7 (.8) | .20 | -.24 (.41) | .034 | 2.03 | .847 (.56 - .94) |
HRCT = Heart Rate in the Conconi Test, VO2CT = Oxygen Comsuption in the Conconi Test, SRCT = Stroke Rate in the Conconi Test, SCT = Speed in the Conconi Test, CV = Variation coeficient, ICC = Intraclass Correlation Coefficient.
* 95% CI
From the correlations between the individual average of the test-retest values and the absolute value of their differences, it can be concluded that random errors are not related to the measured values (the four absolute values for the correlations are lower than 0.2) and the data can be assumed to be homoscedastic.
Figure 3 depicts the Bland-Altman plots for the reliability analysis. To analyze the validity of the modified Conconi test for on -water rowing, the Bland-Altman method was used (Bland and Altman, 1986) and regressions were carried out according to Passing and Bablok (1983) (Figure 4, Table 3).
Figure 3.
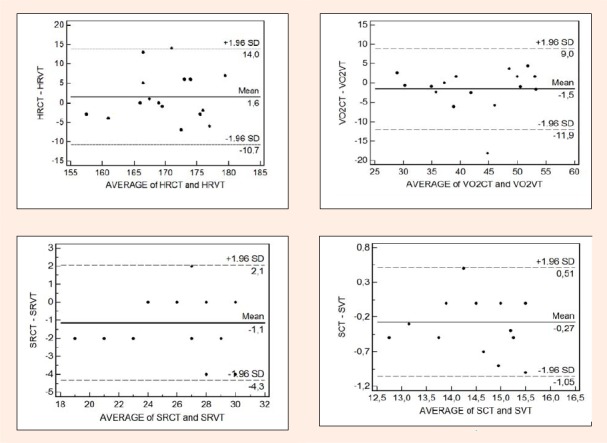
Bland-Altman plots for analysis of reliability.
Figure 4.
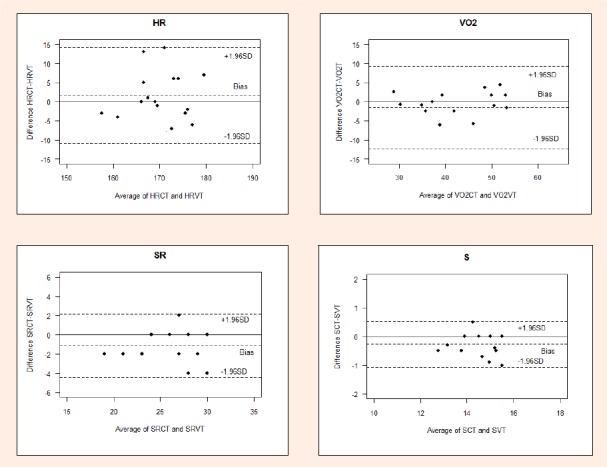
Bland-Altman method for analysis of validity.
Table 3.
Data for Conconi test-retest. Means, standard error of the mean (SEM). Paired T-test between Conconi test-retest with P-values. Coefficients of variation (CV) and intraclass correlation coefficients (ICC).
| HRCT-HRVT | VO2CT-VO2VT | SRCT-SRVT | SCT-SVT | |
|---|---|---|---|---|
| Constant* | 0.00 (-198.6-76.5) | 2.18 (-13.75-11.91) | -1.00 (-7.25-13.00) | 0.15 (-11.55-2.54) |
| Slope | 1.00 (0.54-2.17) | 0.96 (0.72-1.37) | 1.00 (0.50-1.25) | 1.00 (0.83-1.80) |
| Test for linearity | P>0.10 | P>0.10 | P>0.10 | P>0.10 |
* 95% CI
Discussion
Since Conconi et al., 1982 published his method for the first time; the method has been applied to various sports, frequently with varying results. Much of the criticism has been related to poor reliability in the detection of the Anaerobic Threshold Heart Rate (Francis et al., 1989; Jones and Doust, 1995; 1997; Kara et al., 1996; Kiupers et al., 1988; Nicolaizik et al., 1998; Schmid et al., 1998; Thorland et al., 1994; Vachon et al., 1999).
A test is considered to be reliable when the differences between test and retest are insignificant, the within-individual variations are low, and the retest correlations are high. In this study, in order to test the reliability of the modified Conconi test on water for rowers, the field test was repeated in similar conditions. Pearson’s correlation coefficients for the variables HR-SR and HR-S between the test and retest were calculated to be 0.96 and 0.97 respectively. The point of deflection of the heart rate was detected in 88.8% of cases. Two athletes did not clearly exhibit the point of deflection in either the test or retest and, as a result, their data were not included in the second part of the study.
The percentage error in the detection of ATHR (11.2%) is low, given that this was a field study where results can be affected by environmental factors such as the wind, currents or waves. Although care was given to the selection of the day and the location of the tests, tests conducted in the field are always subject to a greater number of variables which may influence the reliability of results more than a laboratory test. Despite this, the results obtained from such tests are excellent predictors of an oarsman’s performance capacity in race conditions. Various authors have found differing percentage errors in the detection of ATHR varying from the 3.2% found by Celik et al., 2005, to the 20% encountered by Bauder et al., 1994. On the other hand, Hofmann et al., 2007 on a rowing ergometer exercise determined the ATHR in all subjects. We suggest that the percentage of error in the present study can be attributed to technical deficiencies of one or more of the athletes, or certain oarsmen’s lack of experience with this type of test. We have found that a necessary condition for the successful detection of ATHR is that the subjects have rehearsed for the test, or have completed a similar test previously. Hofmann et al., 1997 showed in incremental cycle ergometer exercise that only 85.9 % of subjects presented a “regular” deflection of the heart rate performance curve. This may be consistent with our observations.
It can be seen from the analysis of the reliability data of the Conconi test for rowing on-water designed by us that all indices are within the adequate range. A small systematic bias was observed, probably caused by some learning effects. Table 3 demonstrates that no significant differences exist between the means for the variables HR and S. The especially small variability in the test-retest differences for VO2 and S, proves that the small observed bias (both lower than 10%) will be significant. Homoscedasticity makes the errors more relevant in the lowest measures, however, from the Bland- Altman plots (Figure 3) and the intraclass correlation coefficient (ICC) (Table 2), it can be concluded that the Conconi test allows a good approximation from the considered variables (taking into account its variability in the studied population). A learning effect has been detected (re-test mean values are slightly higher than test ones), and a familiarisation process could improve the final results. On the other hand, the recovery time between test-retest was sufficient for this type of test. The observed random test-retest errors can be considered low. We want to highlight that they are from field tests. The highest observed differences are related to the HR variable (10.24 beats·min-1) and the smallest one is for SCT (0.80 km·h-1). It is necessary to point out that ideal conditions for field tests carried out on rowers (without any wind, waves and currents) are extremely difficult to achieve. Therefore, we can conclude that the total errors for Conconi test- retest are suitable for this kind of problems and for the measured variables (1.31 HR, 0.87 VO2, 0.65 SR, and 0.1 S). Furthermore, the differences for oxygen consumption and speed could be attributable to two rowers who had a lower level of fitness than the others as a result of physical difficulties experienced during the season.
The Conconi protocol modified for rowing on water was also shown to be a valid protocol for the calculation of VT using the V-slope method as it is a continuous, progressive, staged maximal test. In all subjects a clear point corresponding to the VT2 was obtained. In order to check the validity of the Conconi method adapted to on-water rowing, the data obtained in the anaerobic threshold heart rate (ATHR) were contrasted with those obtained in the second ventilatory threshold (VT2). The random errors do not depend on the magnitude of the measurement (homoscedascity) and the Bland-Altman analysis (Figure 4) concluded that the limits of agreement (with the reference ventilatory measures) are not significantly different to those obtained from our own Conconi test variation (test-retest analysis). The Bland-Altman analysis suggests an acceptable reliability for the Conconi test (although more trails must be carried out in order to avoid a training effect) and an adequate concordance with the ventilatory method for the measurement of the anaerobic threshold field tests among rowers. Carrying out a Passing-Bablok regression (Passing and Bablok, 1983) demonstrated that all data were within the accepted limits (confidence level of 1 for the slopes, and 0 for the constants). As such this confirms our belief that the modified Conconi test for rowers on water, as designed for this study, could be used as a valid test for the determination of anaerobic threshold in rowers. Grazzi et al., 2008, found a strong concordance for oxygen uptake at the ATHR and VT applying a Bland-Altman analysis in cyclists. However, Carey, 2002, in a study of the validity of the Conconi test, concludes that in such studies the measurement error of HR is unacceptably high, possibly due to the characteristics of the samples studied.
Analyzing the data obtained in the modified Conconi test for rowers on-water it can be observed that the mean values are very homogenous, with very little variation between them (see Table 1). Other studies (Bourgois and Vrijens, 1998; Jones and Doust, 1995; 1997; Kara et al., 1996; Kuipers et al., 1988; Thorland et al., 1994; Vachon et al., 1999; Hofmann et al., 2007) have found higher heart rate at ATHR, similar in fact to that found at the threshold at 4 mmol of lactate or coincide with VT2. The age of subjects is an important factor to take into account when heart rate is studied. In the present study, the ATHR was determined in 88.8 % of cases (age: 22 yr). This result is in agreement with data presented by Hofmann who showed percentages of 86% and 88.8% respectively (Hofmann et al., 1997; 2007). In contrast, Lucia, in subjects aged 62 years old, the percentage in the ATHR was only 31% of cases (Lucia et al., 2000). This suggests that in older athletes the curvilinear performance is rather unlikely. On the other hand, our %HRmax in the ATHR, 91.5%, was similar to that found by Hofmann, 90% and 88.4% respectively (Hofmann et al., 1997; 2007). In contrast, Bourgois et al. (1998) determined the %HR max in the ATHR in 95%. This higher data is possibly due to the age of subjects (17 yr). Hofmann et al., 2007 carried out a study with rowers determining the heart rate turn point (HRTP) in an incremental rowing ergometer exercise test and applied it in a prolonged exercise test. Our data is in agreement with data presented by Hofmann et al., 2007 showing similar values at ATHR and VT2.
Conclusion
Our data suggest that the ATHR matches with the VT2 and it is a valid tool for the determination of anaerobic threshold in field tests among rowers. The limitation of this study may be the width of the limits for the HRCT and VO2CT; variables and make further research necessary with the aim of generalizing these results.
Practical applications
The modified Conconi test for on- water rowing has many advantages. No expensive equipment is necessary, it is a non-invasive test, and it is carried out in the same conditions as the rowers’ training. However, it is a field test, it is very important to reduce the percentage of errors. Rowers must be thoroughly familiarised with the test protocols and two pre-tests of familiarization are necessary to reduce systematic bias. The use of a gas analyzer during the tests can be an obstacle in the normal respiratory cycle stress in oarsmen not familiarised thoroughly with its use. Besides, some specific weather conditions (such as an absence of wind, currents, and waves) are essential in order to reduce random error.
According to Conconi et al., 1996, a key factor in the correct detection of ATHR is that the increments in intensity between stages are minimal in order to ensure maximum progression through the test. The greater the experience of the oarsman, the better his/her ability to know at any given moment at what speed or stroke rate he/she should make. We may assume that ATHR may be suitable for its application in training regulation with rowers.
Biographies
Jorge Villamil Cabo
Employment
Professor at Secondary School. Navia, Spain.
Degree
PhD.
Research interests
Aerobic and anaerobic metabolism, overweight and obesity in adolescents
E-mail: jorgevc@educastur.princast.es

Pablo Martinez-Camblor
Employment
Biosanitary Research Office of Asturias, Statistics Department, University of Oviedo, Spain.
Degree
PhD
Research interests
Applied statistics, specially, for clinical research. Nonparametric curve comparison.
E-mail: pablomc@ficyt.es

Miguel del Valle
Employment
Morphology and Functional Biology Department.Head of Sport Medicine School. University of Oviedo, Spain.
Degree
PhD
Research interests
Biomechanics, Physiology of Sport
E-mail: miva@uniovi.es
References
- Atkinson G., Nevill A.M. (1998) Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Medicine 26(4), 217-238 [DOI] [PubMed] [Google Scholar]
- Ballarin E., Duhues U., Borsetta C., Casoni I., Grazzi G., Guglielmini C., Manfredini F., Mazzoni G., Conconi F. (1996) Reproducibility of the Conconi Test: Test repeatability and observer variations. International Journal of Sports Medicine 17(7), 520-524 [DOI] [PubMed] [Google Scholar]
- Bauder K., Kalus V., Schneekluth U., Weie M., Bärtsch P. (1994) Training Control in rowing ergometer by determination of Conconi deflection point. Deutsche Zeitschrift fur Sportmedizin 45, 308-316 [Google Scholar]
- Beaver W.L., Wasserman K., Whipp B. (1986) A new method for detecting anaerobic by gas exchange. Journal of Applied Physiology 60, 2020-2027 [DOI] [PubMed] [Google Scholar]
- Beneke R., Leithauser M., Hutler M. (2001) Dependence of the maximal lactate steady state on the motor pattern of exercise. British Journal of Sport Medicine 35, 192-196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bland J.M., Altman D.G. (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1, 307-310 [PubMed] [Google Scholar]
- Bourgois J., Vrijens J. (1998) The Conconi test: A controversial concept for the determination of the anaerobic threshold in young rowers. International Journal of Sports Medicine 19, 553-559 [DOI] [PubMed] [Google Scholar]
- Carey D. (2002) Assessment of the accuracy of the Conconi test in determining gas analysis anaerobic threshold. Journal of Strength and Conditioning Research 16, 641-644 [PubMed] [Google Scholar]
- Celik O., Kosar S.N., Korkusuz F., Bozkurt M. (2005) Reliability and validity of the modified Conconi test on Concept II rowing ergometers. Journal of Strength and Condition Research 19, 871-877 [DOI] [PubMed] [Google Scholar]
- Conconi F., Ferrari M., Ziglio P.G., Droghetti P., Codeca L. (1982) Determination of the anaerobic threshold by a noninvasive field test in runners. Journal of Applied Physiology 52, 869-873 [DOI] [PubMed] [Google Scholar]
- Conconi F., Grazzi G., Casoni I., Guglielummi G., Borsetto G., Ballarin E., Mazzoni G., Patracchini M., Manfredini F. (1996) The Conconi test: Methodology after 12 years of application. International Journal of Sports Medicine 17, 509-519 [DOI] [PubMed] [Google Scholar]
- Droghetti P., Borsetto C., Casoni L., Cellini M., Ferrari M., Paolini A.R, Ziglio P.G., Conconi F. (1985) Noninvasive determination of the anaerobic threshold in canoeing, cross-country, skiing, cycling, roller and ice skating, rowing and walking. European Journal of Applied Physiology 53, 299-303 [DOI] [PubMed] [Google Scholar]
- Droghetti P. (1986) Determination of the anaerobic threshold on a rowing ergometer by the relationship between work output and heart rate. Scandinavian Journal of Sports Science 8, 59-62 [Google Scholar]
- Francis K.T., McClatchey P.R., Sumsion J.R., Hansen D.E. (1989) The relationship between anaerobic threshold and heart rate linearity during cycle ergometry. European Journal of Applied Physiology 59, 273-277 [DOI] [PubMed] [Google Scholar]
- Grazzi G., Mazzoni G., Casoni I., Iliari S., Collini G., Heide L., Conconi F. (2008) Identification of a VO2 deflection point coinciding with the heart rate deflection point and ventilatory threshold in cycling. Journal of Strength and Conditioning Research 22(4), 1116-1123 [DOI] [PubMed] [Google Scholar]
- Harris D.J., Atkinson G. (2009) International Journal of Sports Medicine - ethical standards in sport and exercise science research. IInternational Journal of Sports Medicine 30, 701-702 [DOI] [PubMed] [Google Scholar]
- Hofmann P., Bunc P.V., Leitner H., Pokan R., Gaisl G. (1994) Heart rate threshold related to lactate turn point and steady state exercise on a cycle ergometer. European Journal of Applied Physiology 69, 132-139 [DOI] [PubMed] [Google Scholar]
- Hofmann P., Pokan R., Von Duvillard S.P., Seibert F.J., Zweiker R., Schmid P. (1997) Heart rate performance curve during incremental cycle ergometer exercise in healthy young male subjects. Medicine and Science in Sports and Exercise 29, 762-768 [DOI] [PubMed] [Google Scholar]
- Hofmann P., Jürimäe T., Jürimäe J., Purge P., Maestu J., Wonisch M., Pokan R., Von Duvillard S.P. (2007) HRTP, Prolonged Ergometer Exercise, and Single Sculling. International Journal of Sports Medicine 28, 964-969 [DOI] [PubMed] [Google Scholar]
- Jones A.M., Doust J.H. (1995) Lack of reliability in Conconi’s heart rate deflection point. International Journal of Sports Medicine 16, 541-544 [DOI] [PubMed] [Google Scholar]
- Jones A.M., Doust J.H. (1997) The Conconi test is not valid for the estimation of the lactate turnpoint in runners. Journal of Sports Sciences 15, 385-394 [DOI] [PubMed] [Google Scholar]
- Kara M., Kokbel H., Bediz C., Rgne N., Ucok K., Uysal H. (1996) Determination of the heart rate deflection point by the D max method. The Journal of Sports Medicine and Physical Fitness 36(1), 31-34 [PubMed] [Google Scholar]
- Kuipers H., Keiser T., Devries P., Van Rijhoven P., Mijts M. (1988) Comparison of heart rate as a non invasive determinant of anaerobic threshold with the lactate threshold when cycling. European Journal of Applied Physiology 58, 303-306 [DOI] [PubMed] [Google Scholar]
- Lormes W., Buckwitz R., Rebbein H., Steinacker M.J. (1993) Performance and blood lactate on Gjesing and Concept II rowing ergometers. International Journal of Sports Medicine 14, 29-32 [DOI] [PubMed] [Google Scholar]
- Lucia A., Carvajal A., Perez M., Boraita A. (2000) Heart rate response during incremental exercise in master runners. The Japanese Journal of Physiology 50(1),155-158 [DOI] [PubMed] [Google Scholar]
- Lucia A., Sanchez O., Carvajal A., Chicharro JL. (1999) Analysis of the aerobic-anaerobic transition in elite cyclists during incremental exercise with the use of electromyography. British Journal of Sports Medicine 33, 178-185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer T., Lucía A., Earnest C.P., Kindermann W. (2005) A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters-theory and application. International Journal of Sports Medicine (Suppl. 1), S38-48 [DOI] [PubMed] [Google Scholar]
- Nicolaizik W.H., Knopfi E., Leister E., De Boer P., Sievers B., Schoni M.. (1998) The anaerobic threshold in cystic fibrosis: Comparison of the V-slope method, lactate turnpoints, and Conconi test. Pediatric Pulmonology 25, 147-153 [DOI] [PubMed] [Google Scholar]
- Nilsen T., Daigneault T., Smith M. (1993) FISA Coaching Development Programme Course 13-18 [Google Scholar]
- Passing H., Bablok W., (1983) A new biometrical procedure for testing the equality of measurements from two different analytical methods. Application of linear regression procedures for method comparison studies in Clinical Chemistry. Part I. Journa lof Clinical. Chemistry and Clinical Biochemistry 21, 709-720 [DOI] [PubMed] [Google Scholar]
- Petit M.A., Nelson C.M., Rhodes E.C. (1997) Comparison of a mathematical model to predict 10-km performance from the Conconi test and ventilatory threshold measurements. Canadian Journal of Applied Physiology 22, 562-572 [DOI] [PubMed] [Google Scholar]
- Ribiero J.P, Fielding R.A, Hughes V, Black A, Bochese M.A., Knuttgen H.G. (1985) Heart rate break point may coincide with anaerobic and not the aerobic threshold. International Journal of Sports Medicine 6, 220-224 [DOI] [PubMed] [Google Scholar]
- Schmid A., Hounker M., Aramendi J.F., Kluppel E., Barturen J.M., Grathwohl D., Schmidt, Truchsass A., Berg A., Kbul J. (1998) Heart rate deflection compared to 4 mmol lactate threshold during incremental exercise and to lactate during steady state exercise on an arm -cranking ergometer in paraplegic athletes. European Journal of Applied Physiology 78, 177-182 [DOI] [PubMed] [Google Scholar]
- Secher N.H. (1993) The physiology of rowing. Sports Medicine 15, 23-53 [Google Scholar]
- Thorland W., Podolin D.A., Mazzeo R.S. (1994) Coincidence of lactate threshold and HR-power output threshold under various nutritional states. International Journal of Sports Medicine 15, 301-304 [DOI] [PubMed] [Google Scholar]
- Vachon J.A., Basset D.R., Clarke S. (1999) Validity of the heart rate deflection point as a predictor of lactate threshold during running. Journal of Applied Physiology 87, 452-459 [DOI] [PubMed] [Google Scholar]
- Withers R.T., Craig N.P., Bourdon P.C., Norton K.I. (1987) Relative body fat and anthropometric prediction of body density of male athletes. European Journal of Applied Physiology 56, 191-200 [DOI] [PubMed] [Google Scholar]
- Wonisch M., Hofmann P., Schwaberger G.., Von Duvillar S.P., Klein W. (2003) Validation of a field test for non-invasive determination of badminton specific aerobic performance. British Journal of Sports Medicine 37, 115-118 [DOI] [PMC free article] [PubMed] [Google Scholar]