

Abstract
Accurately assessing the energy expenditure (EE) of different types of physical activity is important for exercise prescription in obese individuals. The aim of this study was to examine the accuracy of the Polar S810i Heart Rate Monitor and SenseWear Pro Armband (SWA) for estimating energy expenditure (EE) during indoor rowing versus indirect calorimetry (IC). 43 overweight and obese adults (16 men, 27 women, BMI = 31.2 ± 3.7) participated in the study. Within a week after a maximal incremental test on a rowing ergometer, EE was assessed with Polar S810i, SWA and IC during two different intensities of rowing exercises (at 50% VO2max and 70% VO2max) on a Concept II ergometer. Data were analyzed with Pearson’s product moment correlations and repeated measures ANOVA. Post hoc multiple comparisons were performed using the Bonferroni test. Bland-Altman plots were created to assess the agreement between the EE estimates and IC measurements. At 50% VO2max, Polar S810i and SWA significantly overestimated EE by 0.5 ± 0.50 kcal·min-1 (p < 0.001) and by 0.9 ± 0.92 kcal·min-1 (p < 0.001), respectively. At 70% VO2max, no significant differences were found between the SWA and IC, and between Polar S810i and IC measurements. Bland-Altman plots showed good agreements between the measured EE and estimates by Polar S810i and SWA at 70% VO2max. At 50% VO2max, there was a poor agreement between SWA and IC measurements. There were high correlations among three methods at both intensities (r = 0.82 to r = 0.95). In conclusion, Polar S810i and SWA showed reasonable concordance with IC for measuring EE of the moderate intensity exercise but not the lower intensity exercise on indoor rowing in the participants of this study. Polar S810i and SWA might be useful to assess EE during indoor rowing for overweight and obese individuals who try to manage their body weight, but it is necessary to develop exercise and population specific algorithms to enhance the accuracy of SWA to estimate energy expenditure during various intensities of physical exercises.
Key points.
Polar S810i and SWA when compared to the indirect calorimetry, provide reasonable estimates of energy expenditure on rowing ergometer at the moderate exercise intensity, but not at the low exercise intensity.
The monitor of the Concept II Model D rowing ergometer significantly overestimated the energy expenditure during low and moderate intensity exercises. However there was a moderate correlation between EE estimates of this device and indirect calorimetry measurements.
Key words: Indirect calorimetry, armband, heart rate monitor, energy expenditure, indoor rowing
Introduction
In the past two decades, the world has experienced an increased prevalence of obesity, resulting in a global obesity epidemic. Nearly half a billion of the world’s population now considered to be overweight or obese (Chopra et al., 2002). A number of pathologic conditions and health risks are associated with being overweight or obese affecting both men and women among all racial and ethnic groups (Calle et al., 1999). Interrelations between low physical activity and the epidemiology of obesity and its effects on health are now clear (DiPietro, 1995). Regular physical activity has been shown to improve weight loss when combined with modifications in eating behaviors and is one of the best predictors of long-term weight loss maintenance (Jakicic et al., 2002). At present an energy deficit of 500-1000 kcal/day is recommended to induce proper weight loss (Jakicic et al., 2001). Thus, understanding and accurately assessing the energy expenditure of different types of physical activity is important for exercise prescription.
Indirect calorimetry technique is regarded as the gold standard measure of EE for a structured bout of physical activity (Westerterp, 1999), but it cannot easily assess free-living subjects. Furthermore, the expense of the equipment and supplies, time needed in the laboratory and for subsequent analysis, burden for subjects, and significant amount of technical expertise required limit the use of this technique (Campbell et al. , 2002).
Consequently, to provide simpler estimates, less expensive, smaller, more manageable objective EE assessment tools like motion sensors (accelerometers, pedometers) and heart rate monitors (HRM) have been developed. Motion sensors have been shown to be ineffective at predicting the energy cost of activities such as cycling, upper-body exercise, swimming, rowing, or walking/running up an incline (Fehling et al., 1999; Jakicic et al., 1999; King et al., 2004). Heart rate (HR) is a physiological parameter that can be used to detect changes in exercise intensity even when the movement patterns differ greatly. Thus, the HR monitor is able to estimate EE in activities such as rowing and cycling, which do not elicit vertical displacement of the trunk, where pedometers and accelerometers are less accurate (Jakicic et al., 1999; Campbell et al., 2002). Heart rate monitors also have limitations since they respond to a person’s emotions (such as anxiety) and increased body temperature. They also tend to lag momentarily behind changes in movement and remain elevated after the termination of the movement (Trost, 2007). Crouter et al., 2004 showed that in spite of its inherent limitations, HR monitoring (a Polar S410 HRM) can yield reasonable estimates of EE for exercise modes (treadmill, cycle, rowing ergometer exercises) where motion sensors (i.e., pedometers and accelerometers) often fail. Because Crouter et al., 2004 conducted the study in young, active, normal weight adults; accuracy of the HRM in overweight and obese adults is still questionable.
During recent years, activity monitors that combine various physiological and movement parameters such as accelerometry and physiological parameters have been developed to increase the accuracy in assessing physical activity. One of these is the SenseWear Pro Armband (SWA) (BodyMedia Inc., Pittsburgh, PA, USA), which is worn on the right upper arm over the triceps muscle and combines data from a variety of parameters including heat flux, accelerometer, galvanic skin response, skin temperature, near-body temperature, and demographic characteristics including gender, age, height, and weight. Data registered by the SWA is converted into energy expenditure using the proprietary computer software, which uses activity-specific algorithms. SWA also provides estimates of intensity (MET-level), frequency and duration of physical activity. An advantage with SWA is its design, which allows individuals to wear the device without preventing them from participating in everyday activities and sport activities (Papazoglou et al., 2006). Previous studies in relatively young, normal-weight adults have reported that the SWA in combination with different software versions has shown to be highly reliable at estimating the energy expenditure of rest, but has provided less accurate estimates of energy expenditure when compared with IC during various exercise protocols (Fruin and Rankin, 2004; Jakicic et al., 2004; Papazoglou et al., 2006; Welk et al., 2004). In a previous study, SWA (with software version 4.0), has been validated in obese individuals, showing that accuracy of SWA was poor in three different exercise modes including cycle ergometry, stair stepping, and treadmill walking (Papazoglou et al., 2006). However, in many of the studies that found the SWA to have limited accuracy during several activities, it was also pointed that when applying enhanced software algorithms the SWA may have the potential to provide a feasible assessment of EE (Fruin and Rankin, 2004; Jakicic et al., 2004; Papazoglou et al., 2006; Welk et al., 2004). The new computer software “SenseWear Professional 6.1” therefore remains to be investigated.
Rowing is a different exercise mode which has both a strength and an endurance component (Fagard, 2003) and could be an effective alternative activity (Hagerman et al., 1988) in exercise prescription for obese subjects, especially when the severe obesity impairs the ability to properly walk (Poirier and Despres, 2001). However, to our knowledge, there has been only one study, examining the validity of SWA during indoor rowing (Cole at al., 2004). The authors concluded in that study that when using software developed for the general population, the EE information should be interpreted cautiously during rowing exercise. Because the subjects of that study were normal weight adults (i.e. old, cardiac rehabilitation patients), it is unclear whether similar conclusion would be reached in relatively young and healthy, overweight and obese individuals. Therefore, the aim of the present study was to assess the ability of the Polar S810i HRM and SenseWear Pro Armband to accurately estimate the energy cost of various workloads of indoor rowing in overweight and obese individuals in a laboratory setting measured by simultaneous indirect calorimetry.
Methods
Subjects
From a large group of obese patients participating in an ongoing weight-loss program at Suleyman Demirel University Hospital, forty-three overweight and obese subjects (16 men, 27 women, 24 overweight, 19 obese) who volunteered to participate in rowing ergometer exercise protocols were selected for this study. None of the patients had rowing experience before. Subjects with a medical condition that could prevent safe participation in maximal exercise testing or with a medical condition that would require medical clearance before participation were excluded from this study. Diabetics and patients on medication that might have affected the SWA or the thermoregulatory process (e.g., sibutramine, anti-cholinergics, psychotrops) were not included in this study to minimize the number of confounding factors. The aim and design of the study were approved by the Suleyman Demirel University Ethics Committee, and informed consent was obtained from all participants.
Body composition
Upon arrival at the laboratory on the first test session, anthropometric measurements were taken on each subject. Weight and height were measured in light clothing without shoes. Height was measured to the nearest 0.5 cm using a calibrated stadiometer, weight was measured to the nearest 0.1 kg using an electronic platform scale (Tanita Corp, Tokyo, Japan), and percentage of body fat was measured by Bio-Electric Impedance Analysis using a Tanita body fat monitor/scale (Model TBF-350, 4-contact electrodes with two on each foot, Tanita Corp, Tokyo, Japan). Early in the morning after an overnight fast, subjects stood still on the metal sole plates of the machine wearing only light clothes.
Maximal oxygen uptake test
After giving instructions on how to use the rowing ergometer, subjects performed a discontinuous incremental intensity protocol on a rowing ergometer (Concept II model D, Morrisville, VT, USA). The initial intensity on the rowing ergometry was at 50 W and it was increased by 25 W and 20 W every second minute for men and women, respectively. Subjects stopped rowing for 20 s between each stage so that a blood sample could be drawn. Exercise was terminated when the subjects were no longer able to maintain the required intensity. The test was deemed to be a valid maximal test on the basis of achievement of at least three of the following criteria during the last completed stage: (1) a plateau in VO2 despite increasing exercise intensity; (2) a respiratory exchange ratio exceeding 1.15; (3) a blood lactate concentration exceeding 8-9 mmol.l-1; (4) achievement of age-predicted HRmax; and (5) a rating of perceived exertion of 19 or 20. Gas exchange during the tests was measured breath by breath with a portable gas analyzing system (K4b2, Cosmed, Rome, Italy) (McLaughlin et al., 2001). The HR was recorded every 5 seconds using a telemetric heart rate monitor (Polar S810i, Polar Electro, Kempele, Finland). Blood samples were taken in heparinized glass capillaries from the ear-lobe immediately after each stage and at termination of exercise. Blood lactate concentration was analyzed by an enzymatic membrane method using a YSI 1500 Analyzer (Yellow Springs, OH, USA).
Exercise protocols
All participants were scheduled to return to the laboratory within 1 week (second test session) of maximal oxygen uptake test to perform a single validity test at two different submaximal intensities on a Concept II model D rowing ergometer while simultaneously wearing the SWA and Polar S810i HRM. Subjects were instructed to refrain from consuming any food or performing any exercise for the 3 h before testing. Before the test, each device was initialized with test and participant information (height, weight, age, gender) using a single desktop computer. The use of a single computer allowed each activity monitor device to be aligned to a single clock so that all monitor data could be synchronized to within 1 s. The Polar watch was programmed also with the participant’s actual VO2max and HRmax.
As recommended by the manufacturer, the SenseWearPro Armband was worn on the right arm over the triceps muscle at the midpoint between the acromion and olecranon processes. Upon entering the laboratory, the armband was placed on the subject’s arm and worn while in a seated position for a period of 15 min before data collection to allow for acclimation to skin temperature. Energy expenditure during exercise was computed at 1-min intervals using a generalized proprietary algorithm (SenseWear Professional 6.1) developed by the manufacturer.
The submaximal exercise test consisted of a brief warm-up period followed by two 10-minute stages of rowing at fixed workloads which represented 50% (low intensity) and 70% (moderate intensity) of each subject’s predetermined VO2max, with a 20-min rest between each stage. During the rest interval, participants were allowed to breathe without the facemask and drink water but were not allowed to eat food or drink any calorie-containing beverages. During the exercise protocol, energy expenditure was measured simultaneously using the open-circuit calorimetry, the Polar S810i and the SWA. Due to the time it takes for an individual to reach a physiological steady-state condition and for the indirect calorimetry measurement to reflect actual energy expenditure, the first 3 min of each 10-min measurement were not used in analysis.
The criterion method of assessing energy expenditure during the exercise protocol was open-circuit calorimetry. A K4b2 (Cosmed, Italy) portable gas analyzer was used to measure breath by breath oxygen uptake and the respiratory exchange ratio (RER). The system was worn on the chest and a flexible rubber facemask was placed over the participants’ mouth and nose using a net head cap. Immediately before every test the system was calibrated. Calibration involved 10 pumps of a 3 L syringe into the Cosmed turbine for volume of expired air during ventilation, a room air calibration (20.93% O2 and 0.03% CO2) and a calibration with a standard gas mixture of O2 (16%) and CO2 (5%). Energy expenditure (kcal·min-1) was computed by multiplying the oxygen uptake (l·min-1) by the caloric equivalent based on the RER as described by McArdle et al. (1981).
Concept II Model D rowing ergometers include a performance monitor named PM3. PM3 has a feature which allows calculation of EE using the acceleration and deceleration of the flywheel on every stroke. During the submaximal exercise test EE estimates of PM3 (CII) were also recorded to compare with IC.
Shortly after the completion of the submaximal exercise test each patient was asked to describe his/her subjective perception of effort (RPE) utilizing the 20 points Borg scale (Borg, 1982). All subjects were familiar with RPE scale which comprises fifteen numerical ratings (between 6 and 20) associated with verbal cues, from“7=very very light” to“19=very very hard.”
Statistical analysis
All statistical analyses were performed using SPSS version 15.0 (SPSS INC., Chicago, IL, USA) and the significance level was set at p<0.05. Data are presented as means ± SD. VO2max and HR, blood lactate concentration, RER, and RPE at the termination of the maximal exercise test were compared between men and women and between overweight and obese participants using independent t-tests. Indirect calorimetry (IC) values were established as the criterion EE measure and all EE values are reported as kilocalories per minute. Bivariate Pearson’s product moment correlations were calculated for comparison between the measurement devices and indirect calorimetry. Two-way repeated measures ANOVA (workload x measurement method) was performed to assess differences in the EE measurements (kcal·min-1) for CII, HRM, SWA and IC at two intensity levels. Both measurement method and workload were considered as within-subject variables in the repeated measures. Significant interactions were further analyzed using paired t-tests to determine differences between the mean values obtained with the IC and the other methods, with the critical alpha level adjusted using the Bonferroni procedure. Bland-Altman plots were created to assess the agreement between the IC measurements and estimations of energy expenditure and to graphically show the variability in individual estimated EE values (kcal·min-1) around zero. Limits of agreement involved the percentage mean difference between the two measurement device ± 2 standard deviation of the percentage mean difference. Devices that are accurate will display a tight prediction interval around zero. Data points below zero signify an overestimation, whereas points above zero signify an underestimation.
Results
The characteristics of the participants are shown in Table 1. Maximal incremental exercise responses are shown in Table 2. All participants achieved VO2max based on the criteria used for the present study. While VO2max and RPE at the end of the maximal test were not significantly different among genders, maximum RER and blood lactate concentrations were higher in men than in women, and maximal HR was significantly higher in women.
Table 1.
Descriptive characteristics of the participants (n = 43). Data are means (±SD).
| Overweight Men (BMI < 30 kg·m-2, n=4) |
Obese Men (BMI ≥ 30 kg·m-2, n=12) |
Overweight Women (BMI < 30 kg·m-2, n=15) |
Obese Women (BMI ≥ 30 kg·m-2, n=12) |
All (n=43) |
|
|---|---|---|---|---|---|
| Age (yr) † | 39.5 (3.1) | 37.4 (6.0) | 32.1 (4.7) | 34.5 (4.6) | 34.9 (5.5) |
| Height (cm) † | 1.75 (.03) | 1.74 (.08) | 1.61 (.06) | 1.61 (.08) | 1.66 (.09) |
| Weight (kg) *† | 86.8 (4.8) | 104.5 (12.4) | 72.7 (6.5) | 85.0 (7.0) | 86.3 (15.2) |
| BMI (kg·m-2) *† | 28.4 (1.7) | 34.6 (3.3) | 28.0 (1.3) | 32.9 (2.3) | 31.2 (3.7) |
| %BF† | 29.2 (2.6) | 34.7 (3.2) | 39.4 (3.4) | 43.6 (4.0) | 38.3 (5.6) |
* p < 0.05 for overweight versus obese,
† p < 0.05 for men versus women.
Table 2.
Maximal exercise responses to the incremental rowing test in overweight and obese men and women (n = 43). Data are means (±SD).
| Overweight Men (BMI < 30 kg·m-2, n = 4) |
Obese Men (BMI ≥ 30 kg·m-2, n =12) |
Overweight Women (BMI < 30 kg·m-2, n = 15) |
Obese Women (BMI ≥ 30 kg·m-2, n = 12) |
All (n = 43) |
|
|---|---|---|---|---|---|
| VO2max (ml·min·kg-1)* | 35.4 (4.8) | 27.2 (3.9) | 31.6 (6.0) | 23.4 (2.5) | 28.4 (6.0) |
| VO2max (ml·min·kg-1 FFM)* | 49.9 (5.1) | 41.7 (5.4) | 52.4 (10.5) | 41.4 (3.4) | 46.1 (8.7) |
| HRmax† | 180 (.8) | 181 (6) | 185 (4) | 183 (3) | 183 (4) |
| HR as %APMHR † | 99.7 (1.7) | 99.1 (1.5) | 98.5 (1.7) | 98.3 (2.1) | 98.7 (1.8) |
| Max RER† | 1.30 (.04) | 1.29 (.13) | 1.25 (.09) | 1.26 (.10) | 1.27 (.10) |
| Lactate (mmol·l-1) *† | 12.5 (2.1) | 11.7 (2.7) | 10.1 (2.4) | 8.6 (2.0) | 10.2 (3.2) |
| RPE | 18.7 (.3) | 18.5 (.9) | 18.5 (1.2) | 18.6 (1.1) | 18.5 (1.1) |
* p < 0.05 for overweight versus obese,
† p < 0.05 for men versus women, FFM, fat-free mass, APMHR, age-predicted maximum HR (220 - age), RPE, ratings of perceived exertion (Borg scale).
Compared with overweight participants, the obese had lower VO2max and blood lactate concentration (Table 2). Average energy expenditure values for indirect calorimetry, Concept IITM, Polar S810iTM and the SenseWear Pro ArmbandTM are presented in Figure 1A for the workload set at 50% VO2max and Figure 1B for the workload set at 70% VO2max. RPE was 10.3 ± 1.1 and 14.8 ± 1.1 for low and moderate intensity exercises, respectively. A significant workload by measurement method interaction occurred for the repeated measures ANOVA (p < 0.001). Post hoc analyses were performed to compare the energy expenditure during each 10-min workload between indirect calorimetry and other methods with the critical P value adjusted based on the number of comparisons using the Bonferroni procedure. Results showed that CII significantly overestimated EE during both at 50% VO2max and 70 % VO2max workloads by 2.3 ± 1.0 kcal·min-1 and 2.9 ± 1.3 kcal·min-1 , respectively (p < 0.001). Polar S810i significantly overestimated EE during low intensity exercise by 0.5 ± 0.50 kcal·min-1 (p < 0.001). There was no significant difference in EE between Polar S810i and IC during moderate intensity exercise (p = 0.027, adjusted critical p-value was 0.05/6=0.008). The mean error (IC - S810i) was - 0.2 ± 0.57 kcal·min-1 (-0.38 to -0.02 kcal·min-1, 95% CI). The SenseWear Pro ArmbandTM significantly overestimated EE during low intensity exercise by 0.9 ± 0.92 kcal·min-1 (P < 0.001). There was no significant difference in EE between SWA and IC during moderate intensity exercise (p = 0.149, adjusted critical p-value was 0.05/6=0.008). The mean error (IC - SWA) was 0.1 ± 0.55 kcal·min-1 (−0.05 to 0.29 kcal·min-1, 95% CI).
Figure 1.
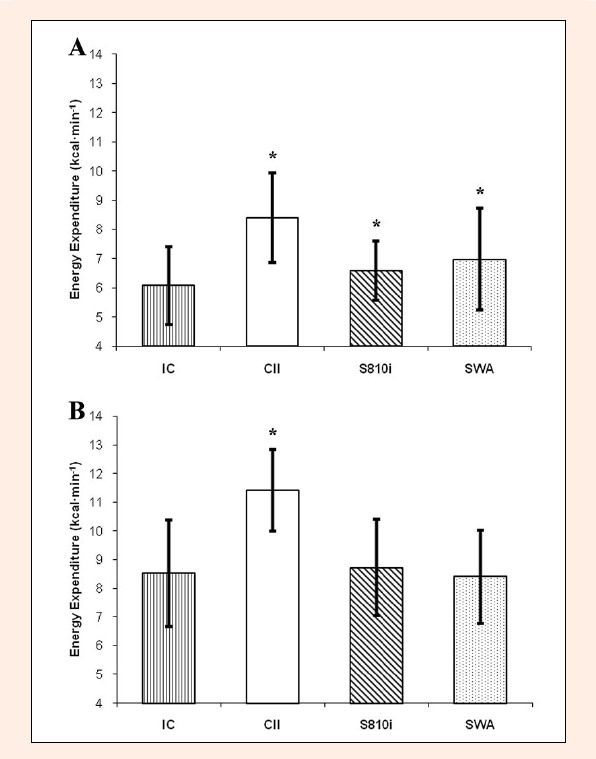
Energy expenditure values at 50% VO2max for Concept II PM3 monitor, the Polar S810i heart rate monitor, SenseWear Pro armband, and indirect calorimetry (IC) on rowing ergometer. B) Energy expenditure values at 70% VO2max for Concept II PM3 monitor, the Polar S810i heart rate monitor, SenseWear Pro armband, and indirect calorimetry (IC) on rowing ergometer (mean ± standard error). * significantly different from IC (p < 0.001).
The mean EE measurements for each subject provided by the Polar S810i and IC were highly correlated at low and moderate intensity exercises (r = 0.86; P < 0.001 and r = 0.95; P < 0.001, respectively). The Bland-Altman plots (Figure 2A and Figure 3A) display the good agreement between the two measures for both intensities. The SWA estimate significantly correlated with the IC energy expenditure at low and moderate intensity exercise (r = 0.82; p < 0.001 and r = 0.87; p < 0.001, respectively). The Bland-Altman plots (Figure 2B) shows a poor agreement and a strong tendency for a fanning effect with a wider spread of biases at higher EE measurements (larger prediction errors for the individuals with the highest energy expenditures) for low intensity exercise. At the moderate intensity exercise the plot reveals a very good agreement between SWA and IC and no bias toward over- or underestimation (Figure 3B). The fanning effect was weakened but still evident at moderate intensity exercise (Figure 3B).
Figure 2.
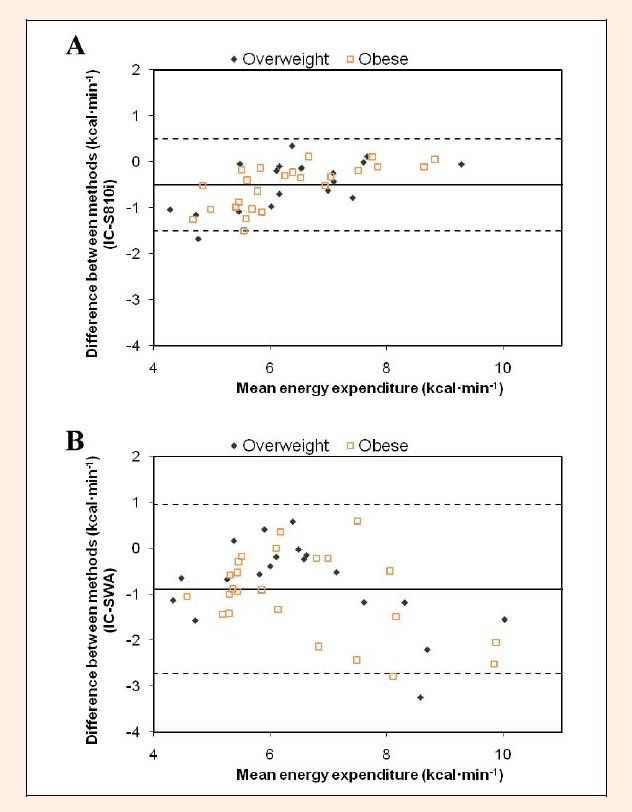
Bland-Altman bias plot between Polar S810i estimate and IC measurement for rowing energy expenditure at 50% VO2max. 95% Limits of Agreement = -1.50 to 0.49; 95% CI = -0.73 to −0.28 B) Bland-Altman bias plot between SWA estimate and IC measurement for rowing energy expenditure at 50% VO2max. 95% Limits of Agreement = -2.73 to 0.94; 95% CI = -1.30 to -0.49. The middle solid line represents the mean difference between the methods, and the dashed lines represent the 95% limits of agreement.
Figure 3.
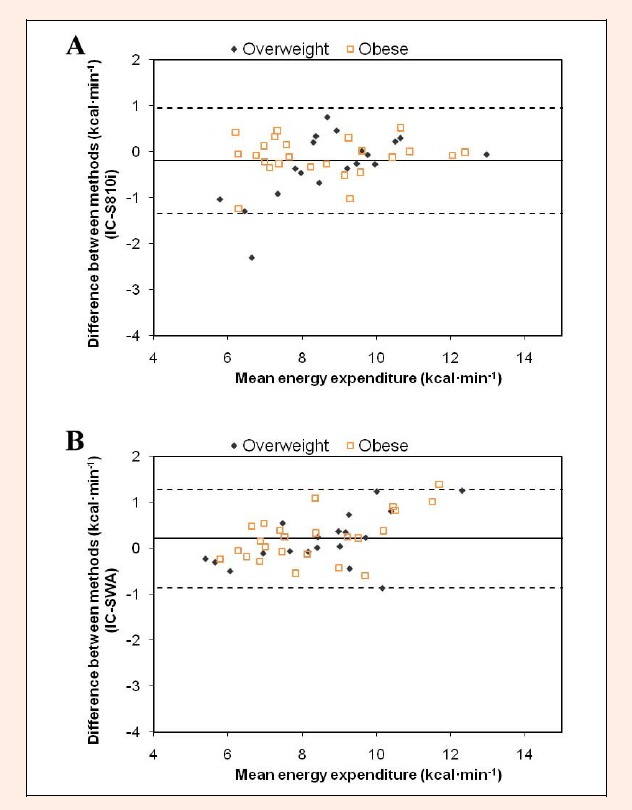
Bland-Altman bias plot between Polar S810i estimate and IC measurement for rowing energy expenditure at 70% VO2max. 95% Limits of Agreement = -1.35 to 0.95; 95% CI = -0.45 to 0.05 B) Bland-Altman bias plot between SWA estimate and IC measurement for rowing energy expenditure at 70% VO2max. 95% Limits of Agreement = -0.87 to 1.28; 95% CI = -0.03 to 0.44. The middle solid line represents the mean difference between the methods, and the dashed lines represent the 95% limits of agreement..
There were moderate significant correlations (r = 0.65; p < 0.001 and r = 0.57; p < 0.01, for low and moderate intensity, respectively) but very poor agreement between the CII and IC EE measurements (plots not shown). Limits of agreement for low and moderate intensities were -4.38 to -0.23 kcal·min-1 and -5.51 to -0.27 kcal·min-1, respectively. When separated by gender (men - women) and by weight status (overweight - obese) the results of the analyses did not differ (results not shown).
Discussion
This study investigated the validity of three simple devices (CII, S810i, and SWA) during indoor rowing across two submaximal exercise intensities in overweight and obese adults by comparing EE estimates for each device to actual EE determined with simultaneous IC. All devices significantly overestimated EE at low intensity of rowing. As illustrated in Figure 1B, during moderate exercise intensity, S810i and SWA provide EE estimates that are not significantly different from EE measured using indirect calorimetry. Although there were moderate to high correlations between EE estimates of all three devices and IC measures for both exercise intensities, the Bland-Altman plots show that there was a considerable individual variation in the estimates of EE using CII. During both low and moderate intensity, high correlation and very good agreement were found between S810i estimates and the measured values by IC. Similar high correlations were provided by SWA, but there were large limits of agreement. The magnitude of the difference in EE between SWA and IC appeared to increase for the individuals with the highest energy expenditures. Our results are in accordance with the previously reported results for the Polar S810i in healthy adults (Crouter et al., 2004) and SWA in cardiac patients (Cole et al., 2004). To our knowledge, this study is the first to examine the validity of the Polar S810i and the SWA for estimating EE during indoor rowing in overweight and obese individuals.
The findings of this study suggest that Polar HRM may provide accurate exercise EE estimates in overweight and obese adults during indoor rowing based upon the fact that there were no significant differences at moderate intensity exercise, the measurements were highly correlated, and had good agreement at low and moderate intensities. However, to provide reasonable estimates, the Polar HRM needs to be programmed using individuals’ measured VO2max and HRmax. Particular types of Polar heart rate monitors, including S810i, have the “OwnIndex” software which uses nonexercise prediction equations for VO2max and HRmax. As a limitation of this study, HRmax and VO2max values which were predicted by OwnIndex were not used. However, Crouter et al., 2004 showed that without using actual values, the Polar HRM provided only a rough estimate of EE. As evidenced by the present results, age-predicted maximum HR (220 - age) can yield reasonable predictions (Table 2). Thus, reported differences in accuracy seem to be caused by the inconsistency between actual and predicted VO2max values. However, it is most of the time impractical to measure VO2max for being used in large intervention trials and for exercise prescription (Poirier and Després, 2001).
The SWA, on the other hand, does not have this disadvantage. The SWA device was user-friendly for the subjects in terms of easy attachment/detachment, minimal discomfort, and little or no interference in activity. In a previous study including obese adults, Papazoglou et al., 2006 showed that SWA substantially overestimated the EE during exercise and had clinically significant limits of agreement when compared with the IC. These results were partly in contradiction with the present study. When compared with that study, the SWA appears to provide a better estimate of moderate intensity exercise energy expenditure and a similar estimate of lower intensity energy expenditure. However, in the study by Papazoglou et al., 2006 the exercise modes (cycle ergometry, stair stepping, and treadmill walking) were different than indoor rowing. Discrepancies between the present results and previous studies may also be due to the software used in combination with SWA. Papazoglou et al., 2006 used an older version of software (Version 4.0). For example, using Version 1.0, Fruin and Rankin, 2004 reported no significant differences in EE measurements on cycle ergometer between the SWA and IC. However, there was a poor correlation (r = 0.03 to 0.12) and wide range of agreement (−3.8 to 3.5 kcal·min-1) in Bland-Altman analyses. Better agreement obtained at moderate intensity in the present study might suggest improvement of the generalized algorithm within the latest version of the software (version 6.1). The algorithms are proprietary to the manufacturer; therefore it has not been possible to compare the versions transparently. Additionally, the discrepant findings in the study by Fruin and Rankin, 2004 could be partially attributed to a difference in the mechanical efficiency of healthy and obese subjects (Lafortuna et al., 2008). In overweight and obese individuals, reduced mechanical efficiency might lead greater body motion during rowing, and consequently, overestimation of EE by accelerometry based monitor. The weights of the other physiological parameters in the algorithm may have increased at the higher exercise intensities. More research is needed to determine whether the changing the weights of sensor data may provide more accurate estimation than commercially available software algorithm. All subjects of the present study were participating in an ongoing weight-loss program and were used to train at lower exercise intensities. This program may have altered the metabolic response to exercise. This could have influenced the results and may explain less accurate estimations attained during lower intensity exercise. Despite the significant differences and large limits of agreements, there was a strong correlation (r = 0.82; p < 0.001) between SWA estimates and IC measurements at the lower exercise intensity. It seems that it is necessary to improve the algorithm to enhance the accuracy of SWA to estimate energy expenditure during lower intensity exercises on rowing ergometer.
An interesting finding of this study was the significant correlation between EE estimates of CII and IC measurements. Concept II ergometers are commonly used by elite rowers for training and competition purposes (Mäestu et al., 2005). Rowing is a learned skill and none of the participants in this study had rowing experience. Generalized equation for the calculation of EE may account for the significant overestimation of CII observed in this study. Creating different equations incorporating more data from obese and sedentary individuals by the manufacturer might lead to an enhancement in the accuracy of CII to estimate EE.
The most recent recommendations suggest that to promote weight-loss and reduce fat mass, obese patients need combined caloric restriction and endurance training at moderate intensities (55-65% VO2max) (Hansen et al., 2007). These recommendations further suggest that resistance training should form an integrative part of any exercise intervention to improve muscle mass and function. (Hansen et al., 2007). Rowing, which involves dynamic and static exercise with large muscle groups (Fagard, 2003) provides a convenient mode of exercise training to meet these needs simultaneously. Therefore, the need for practical tools to estimate EE during low to moderate intensity exercise on rowing ergometer, as well as different modes of activities, is evident. The present study revealed that in overweight and obese individuals, the SWA, using in combination with SenseWear Professional 6.1 software, provided accurate estimation of energy expenditure during the moderate intensity rowing exercise but not during the lower intensity exercise. These small, unobtrusive devices seem to have a capacity to be placed in exercise prescriptions for obese individuals in future. However, an enhancement of the accuracy of the generalized algorithm is needed. Additionally, despite the promising findings demonstrated in this study, it is necessary to test the reliability of the SWA in estimating the energy expenditure of various activities in various populations before conclusions can be made about the overall reliability of this device, although it was beyond the scope of this study.
Conclusion
This study was novel in that it assessed the accuracy of SWA and Polar heart rate monitor to estimate EE (versus indirect calorimetry) in an overweight and obese population using a rowing ergometer. In conclusion, the results of the present study showed that when compared with IC, both Polar S810i and SWA can provide reasonable EE estimates during the moderate intensity indoor rowing in overweight and obese individuals. Despite the strong correlation between SWA and IC, the accuracy of the SWA was poor during the lower exercise intensity. For the moderate exercise intensity, EE estimates of Polar S810i which was programmed with the actual measured values for VO2max and HRmax were not significantly more accurate than those of SWA. SWA looks promising but it is necessary to develop exercise and population specific algorithms to enhance the accuracy to estimate energy expenditure during various intensities of physical exercises.
Acknowledgements
Authors would like to thank Research Assistant Dr. Mustafa Yolcu for his technical assistance in conducting the exercise tests.
Biographies
Ali Erdogan
Employment
Assistant Professor, Suleyman Demirel University, Faculty of Medicine.
Degree
PT, PhD.
Research interests
Exercise and sports performance training and testing, sports medicine
E-mail: aerdogan@med.sdu.edu.tr
Cem Cetin
Employment
Associate Professor of Sports Medicine, Suleyman Demirel University, Isparta, Turkey.
Degree
MD.
Research interests
Exercise testing, rehabilitation in sports medicine
E-mail: cem@med.sdu.edu.tr
Hilmi Karatosun
Employment
Associate Professor of Sports Medicine, Suleyman Demirel University, Isparta, Turkey.
Degree
PhD.
Research interest
Sports physiology
E-mail: hilmi@med.sdu.edu.tr
Metin Lütfi Baydar
Employment
Professor of Orthopedics and Traumatology, Suleyman Demirel University, Isparta, Turkey.
Degree
MD.
Research interests
Exercise and sports traumatology, sports medicine
E-mail: mlbaydar@sdu.edu.tr
References
- Borg G.(1982) Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise 14, 377-381 [PubMed] [Google Scholar]
- Calle E.E., Thun M.J., Petrelli J.M., Rodriguez C., Heath C.W.(1999) Body-mass index and mortality in a prospective cohort of U.S. adults. The New England Journal of Medicine 341, 1097-1105 [DOI] [PubMed] [Google Scholar]
- Campbell K.L., Crocker P.R., Mc Kenzie D.C.(2002) Field evaluation of energy expenditure in women using Tritrac accelerometers. Medicine and Science in Sports and Exercise 34, 1667-1674 [DOI] [PubMed] [Google Scholar]
- Chopra M., Galbraith S., Darnton-Hill I.(2002) A global response to a global problem: the epidemic of overnutrition. Bulletin of the World Health Organization 80(12), 952-958 [PMC free article] [PubMed] [Google Scholar]
- Cole P.J., LeMura L.M., Klinger T.A., Strohecker K., Mc Connell T.R.(2004)Measuring energy expenditure in cardiac patients using the Body Media Armband versus indirect calorimetry. A validation study Journal of Sports Medicine and Physical Fitness. 44(3), 262-271 [PubMed] [Google Scholar]
- Crouter S.E., Albright C., Bassett D.R., Jr. (2004) Accuracy of Polar S410 Heart Rate Monitor to Estimate Energy Cost of Exercise. Medicine and Science in Sports and Exercise 36(8), 1433-1439 [DOI] [PubMed] [Google Scholar]
- Di Pietro L.(1995) Physical activity, body weight and adiposity: an epidemiologic perspective. Exercise and Sport Sciences Reviews 23, 275-303 [PubMed] [Google Scholar]
- Fagard R.H.(2003) Athlete’s heart. Heart 89, 1455-1461 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fehling P.C., Smith D.L., Warner S.E., Dalsky G.P.(1999) Comparison of accelerometers with oxygen consumption in older adults during exercise. Medicine and Science in Sports and Exercise 31, 171-175 [DOI] [PubMed] [Google Scholar]
- Fruin M.L., Rankin J.W.(2004) Validity of a multi-sensor armband in estimating rest and exercise energy expenditure. Medicine and Science in Sports and Exercise 36, 1063-1069 [DOI] [PubMed] [Google Scholar]
- Hagerman F.C., Lawrence R.A., Mansfield M.C.(1988) A comparison of energy expenditure during rowing and cycling ergometry. Medicine and Science in Sports and Exercise 20(5), 479-488 [PubMed] [Google Scholar]
- Hansen D., Dendale P., Berger J., van Loon L.J., Meeusen R.(2007) The effects of exercise training on fat-mass loss in obese patients during energy intake restriction. Sports Medicine 37(1), 31-46 [DOI] [PubMed] [Google Scholar]
- Jakicic J.M., Winters C., Lagally K., Ho J., Robertson R.J., Wing R.R.(1999) The accuracy of the Tritrrac-R3D accelerometer to estimate energy expenditure. Medicine and Science in Sports and Exercise 31, 747-754 [DOI] [PubMed] [Google Scholar]
- Jakicic J.M., Clark K., Coleman E., Donnelly J.E., Foreyt J., Melanson E., Volek J., Volpe S.L.(2001) Appropriate intervention strategies for weight loss and prevention of weight regain for adults: position stand of The American College of Sports Medicine. Medicine and Science in Sports and Exercise 33(12), 2145-2156 [DOI] [PubMed] [Google Scholar]
- Jakicic J.M., Wing R.R., Winters-Hart C.(2002) Relationship of physical activity to eating behaviors and weight loss in women. Medicine and Science in Sports and Exercise 34, 1653-1659 [DOI] [PubMed] [Google Scholar]
- Jakicic J.M., Marcus M., Gallagher K.I., Randall C., Thomas E., Goss F.L., Robertson R.J.(2004) Evaluation of the SenseWear Pro Armband to assess energy expenditure during exercise. Medicine and Science in Sports and Exercise 36, 897-904 [DOI] [PubMed] [Google Scholar]
- King G.A., Torres N., Potter C., Brooks T.J., Coleman K.J.(2004) Comparison of Activity Monitors to Estimate Energy Cost of Treadmill Exercise. Medicine and Science in Sports and Exercise 36(7), 1244-1251 [DOI] [PubMed] [Google Scholar]
- Lafortuna C.L., Agosti F., Galli R., Busti C., Lazzer S., Sartorio A.(2008) The energetic and cardiovascular response to treadmill walking and cycle ergometer exercise in obese women. European Journal of Applied Physiology 103(6), 707-717 [DOI] [PubMed] [Google Scholar]
- Mäestu, F., Jürimäe J., Jürimäe T. (2005) Monitoring of performance and training in rowing. Sports Medicine 35, 597-617 [DOI] [PubMed] [Google Scholar]
- Mc Ardle W.D., Katch F.I., Katch V.L.(1981) Exercise physiology: energy, nutrition, and human performance Philadelphia: Lea and Febiger, 508 [Google Scholar]
- Mc Laughlin J.E., King G.A., Howley E.T., Bassett D.R., Jr., Ainsworth B.E.(2001) Validation of the COSMED K4b2 Portable Metabolic System. International Journal of Sports Medicine 22, 280-284 [DOI] [PubMed] [Google Scholar]
- Papazoglou D., Augello G., Tagliaferri M., Savia G., Marzullo P., Maltezos E., Liuzzi A.(2006) Evaluation of a Multisensor Armband in estimating energy expenditure in obese individuals. Obesity 14, 2217-2223 [DOI] [PubMed] [Google Scholar]
- Poirier P., Després J.P. (2001) Exercise in weight management of obesity. Cardiology Clinics 19(3), 459-470 [DOI] [PubMed] [Google Scholar]
- Trost S.G.(2007) State of the art reviews: measurement of physical activity in children and adolescents. American Journal of Lifestyle Medicine 4, 299-314 [Google Scholar]
- Welk G.J., Schaben J.A., Morrow J.R.(2004) Reliability of accelerometry-based activity monitors: a generalizability study. Medicine and Science in Sports and Exercise 36, 1637-1645 [PubMed] [Google Scholar]
- Westerterp K.R.(1999) Assessment of physical activity level in relation to obesity: current evidence and research issues. Medicine and Science in Sports and Exercise 331, S522-S522 [DOI] [PubMed] [Google Scholar]