

Abstract
The centre of pressure (COP) movement during stance maintenance on a stable surface is commonly used to describe and evaluate static balance. The aim of our study was to test sensitivity of individual COP parameters to different stance positions which were used to address size specific changes in the support surface. Twenty-nine subjects participated in the study. They carried out three 60-second repetitions of each of the five balance tasks (parallel stance, semi-tandem stance, tandem stance, contra-tandem stance, single leg stance). Using the force plate, the monitored parameters included the total COP distance, the distance covered in antero-posterior and medio-lateral directions, the maximum oscillation amplitude in antero-posterior and medio-lateral directions, the total frequency of oscillation, as well as the frequency of oscillation in antero-posterior and medio-lateral directions. The parameters which describe the total COP distance were the most sensitive to changes in the balance task, whereas the frequency of oscillation proved to be sensitive to a slightly lesser extent. Reductions in the support surface size in each of the directions resulted in proportional changes of antero-posterior and medio- lateral directions. The frequency of oscillation did not increase evenly with the increase in the level of difficulty of the balance task, but reached a certain value, above which it did not increase. Our study revealed the monitored parameters of the COP to be sensitive to the support surface size manipulations. The results of the study provide an important source for clinical and research use of the body sway measurements.
Key points.
Testing static balance with body sway related center of pressure (COP) parameters;
Testing sensitivity of COP sub-components to manipulations of the stance position;
Analytical approach to the study of COP parameters that enable the insight to the frequency/amplitude and direction-dependency relationships;
Adding to the basic knowledge of static balance which can be applied to testing and training routines.
Key words: Balance, body sway, center of pressure, feet positioning, sensitivity
Introduction
For the purpose of describing the ability to maintain a balanced body posture, various body sway (BS) parameters are used in clinical, sports and research practices (Chiari et al., 2002; Rocchi et al., 2004). The selection of suitable BS parameters depends on the methods to be used, as well as on the stationary or dynamic nature of the balancing task (Gillette and Abbas, 2003; Sarabon et al., 2010b; Winter, 1995). BS related quantitative data are useful for an in-depth evaluation of balance mechanisms in the elderly, people with injuries or anomalies of the locomotor system, and athletes (Baczkowicz et al. , 2008; Nardone et al., 2009; Nault et al., 2002; Popa et al., 2007; Winter, 1995; Yim-Chiplis and Talbot, 2000).
BS is reflected in the movement of the common center of body mass (COM). However, for the methodological reasons the movement of the common center of foot pressure (COP) is most often used in research and clinical practice (Chiari, et al., 2002; Lamoth et al., 2009; Rocchi et al., 2004; Winter et al., 2003). It was shown by Winter, 1995 that COP in quiet stance almost synchronously reflects movement of COM. Various balance strategies, such as ankle and hip strategies, are used by the body to control BS in medio-lateral (m-l) as well as in anterio-posterior (a-p) directions (Benvenuti, 2001; Gage et al., 2004; Winter, 1995; Winter et al., 2003)
Manipulating those biomechanical factors that affect BS, creates an opportunity for a more analytical insight into clinical balance testing and goal directed training (Benvenuti, 2001; Winter et al., 2003). The support surface size (SSS), mathematically defined as the convex hull of the contact surface, is most commonly modified. SSS influences passive and active body stability and stiffness (Benvenuti, 2001). It can be manipulated separately in an a-p or in m-l direction using direction specific foot placement. The stability of the body in both directions is dependent on the width of the foot placement, while stability in the sagittal plane is additionally influenced by the length of the feet (Benvenuti, 2001; Gillette and Abbas, 2003; Tarantola et al., 1997; Winter et al., 1998; 2003).
In order that the BS testing methods could be useful for clinical and research practice, their repeatability (intra- and inter-visit) as well as the sensitivity (to acute-chronic conditioning-deconditioning effects as well as to pathology and task specifics) are of primary importance. Superior sensitivity is gained by using two separate force plates, enabling a more in- depth evaluation of BS and the control mechanisms involved (Benvenuti, 2001). In practice, clinicians usually only have a single force plate at their disposal, which is sufficient in the great majority of cases to provide the relevant data (Winter et al., 2003). It is of importance for users of single force plate methods to check for basic metric characteristics and to adhere to the measurement protocols accordingly. Our previous publication (Sarabon et al., 2010b) reported that good intra-visit repeatability could be obtained with single force plate balance tests. The aim of the current study was to build on the previous one and to evaluate the sensitivity of those COP parameters which proved to have the highest repeatability. For this purpose a systematic modification of the SSS by changing foot positions was used. As an outcome, based on the acquired results, some indications for practical use are proposed in the discussion.
Methods
Subjects
Twenty-nine subjects participated in the study (13 males and 16 females). Their average age was 26.3 ± 4.7 years, and their average height was 1.78 ± 0.4 m. Prior to the start of the experiment, interviews were held with all the subjects, during which they were informed about the course of the study and possible risks. Subjects with neurological disorders, disorders of the locomotor system, or disorders of the vestibular or visual systems were excluded from the study. Prior to their participation, all subjects signed a statement of informed consent to participate in measurements.
Measurement protocol
The experiment consisted of measurements of maintaining balance during quiet stance on a force plate. The subjects' task was to maintain a balanced position in each of five foot placements. All these balance tasks required the subjects to maintain a balanced position of the trunk with their hands placed on their hips while their gaze was directed at a certain point in front of the body. Throughout the measurement, the knees had to be fully extended, however, they had to be active and not in the position of locking the joint. The following foot placements were used (Figure 1); (i) feet placed parallel in hip width (parallel stance at hip width apart - PS), (ii) feet placed parallel at hip width apart, with the dominant leg placed in front of the non-dominant leg by a half of the foot length (semi-tandem stance - SET), (iii) feet placed together, medial edges of feet touching, and the dominant leg placed in front of the toes of the other leg by a half of the foot length (tandem stance - TAN), (iv) feet placed in the same position as is in TAN, however with the non-dominant leg in the front (contralateral tandem stance - CTA), and (v) a single leg stance with the other leg lifted from the floor with the knee bent at a 90° angle, with the thighs parallel (single leg stance - SL). The support leg was defined as the take-off leg i.e. the leg opposite to the kicking leg.
Figure 1.
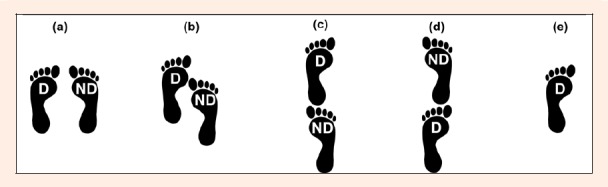
The five different foot positions used: (a) PS, (b) SET, (c) TAN, (d) CTA, and (e) SL. The leg dominance is marked by D (dominant leg) and ND (non-dominant leg). Note that the m-l dimension in PS (a) equals that of the hip-width.
The subject performed each individual task with three trials, each lasting 60 seconds. The sequence of performing the balance tasks was randomized. Between each trial, the subject had a two-minute break and a five-minute break each time the foot placement was changed. Altogether, each subject performed fifteen trials.
Data collection and processing
Balance was measured by means of the AMTI balance board (Watertown, USA). The measurement data was acquired with a personal computer (sampling frequency 1000 Hz). Raw data processing was conducted using Wise-Coach software (Wise Technologies, Ljubljana, Slovenia). The software contains algorithms for calculating the total distance performed by the center of pressure (SΣ), the COP distance covered in the m-l direction (Sm-l), the COP distance covered in the a-p direction (Sa-p), the maximum amplitude described by the COP in the m-l direction during the measurement (Am-l), the maximum amplitude in the a-p direction (Aa-p), the total frequency of oscillation in the m-l and a-p directions (FΣ), the frequency of oscillation in the m-l direction (Fm-l), and the frequency of oscillation in the a-p direction (Fa-p) (Sarabon et al., 2010a). The FΣ, Fm-l, Fa-p and parameters represent the average within a 60-second trial, while SΣ, Sm-l, and Sa-p are cumulative values for an individual trial (in mm). For further statistical processing SPSS 13 software (SPSS Inc., Chicago, USA) was used.
Statistical analyses
For each subject the average of each individual parameter during three consecutive repetitions of the same balance task was taken for further statistical analysis. Basic descriptive statistics were conducted. Deviations from the normal distribution were observed through the coefficients of kurtosis and skewness. Intra-class correlation coefficients (ICC) and their confidence limit intervals were calculated to check for repeatability.
Differences among various foot placements in individual parameters were examined by means of two-way repeated measures analysis of variance (RANOVA). Paired T-tests with Bonfferoni corrections for multiple comparisons were applied post hoc.
The correlations between SΣ, Sm-l, and Sa-p were examined using the Pearson correlation coefficient (r).
Results
All eight measured COP parameters proved to be responsive to the changes in SSS. The biggest changes and differences among individual balance tasks were observed in parameters SΣ, Sm-l and Sa-p (Figure 2). Most clearly noticeable was the change in Sm-l in SL. Parameters Am-l, Aa-p, FΣ, Fm-l, and Fa-p were responsive to a slightly lower degree, but all of them reflected a change according to the PS. Differences among other stances in Am-l, Aa-p, FΣ, Fm-l, and Fa-p were minor and not statistically significant (p ≥ 0.05). On the other hand, statistically significant differences (p < 0.05) were observed in SΣ, Sm-l, and Sa-p pair-wise comparisons with the exception of TAN:CTA and TAN:SL.
Figure 2.
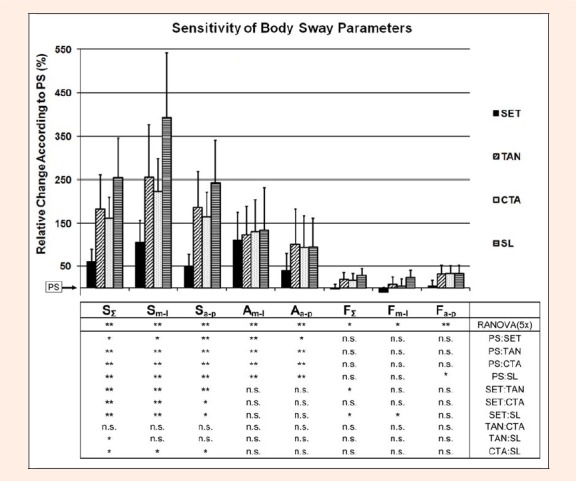
Relative changes in individual COP parameters as a result of SSS manipulation. Vertical bars (average ± standard deviations) represent values of COP parameters relative to the PS values. Statistical significance is indicated (* for p < 0.05, ** for p < 0.01 and n.s. for p ≥ 0.05) in the table below for RANOVA (first row) and T-tests (the lower rows from the second on).
Correlations among SΣ:Sm-l, SΣ:Sa-p and Sm-l:Sa-p for all balance tasks were high (over 0.9 for SΣ:Sm-l, SΣ:Sa-p, p < 0.05 and over 0.76 for Sm-l:Sa-p, p < 0.05) (Figure 3 and Figure 4).
Figure 3.
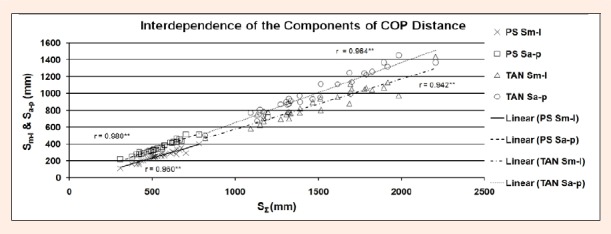
Relationship between SΣ and Sm-l or SΣ and Sa-p for SL and TAN. Pearson correlation coefficients (r) and levels of statistical significance are indicated (** for p < 0.01).
Figure 4.
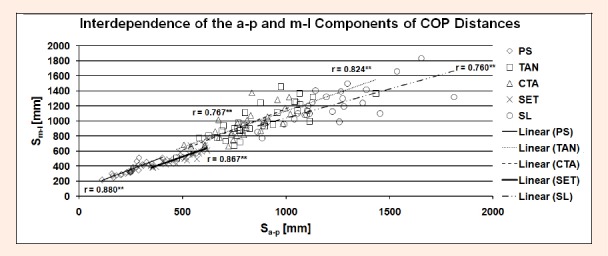
Relationship between Sa-p and Sm-l for PS, TAN, CTA, SET and SL. Pearson correlation coefficients (r) and levels of statistical significance are indicated (** for p < 0.01).
Table 1 illustrates the descriptive statistics of the results. A comparison of the averages of the parameters for individual conditions points to a linear growth of all parameters related to the COP distance. No considerable changes or increases were observed in parameter Am-l during SET, TAN, CTA and SL. The lowest Am-l was in PS. To a smaller extent Am-l increased from PS through SET to TAN. The TAN, CTA and SL balance tasks did not exhibit differences in Am-l, however, a slightly smaller increase of Aa-p was observed.
Table 1.
Basic descriptive statistics and measures of repeatability (ICC with confidence limits) for all the COP parameters in all the stance conditions.
| N | MIN | MAX | AVG | SD | VAR | SKEW | KURT | ICC | ICC-low | ICC-upper | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PS | SΣ (mm) | 29 | 307.4 | 781.7 | 537.6 | 107.8 | 11616 | .12 | -.16 | .83 | .69 | .91 |
| Sm-l (mm) | 29 | 111.5 | 403.0 | 254.0 | 63.3 | 4002 | -.03 | .37 | .84 | .71 | .92 | |
| Sa-p (mm) | 29 | 219.0 | 512.7 | 357.7 | 75.2 | 5658 | .42 | -.41 | .78 | .59 | .89 | |
| Am-l (mm) | 29 | 6.2 | 20.1 | 13.1 | 3.9 | 15.4 | .07 | -.99 | .54 | .15 | .77 | |
| Aa-p (mm) | 29 | 13.0 | 43.2 | 21.3 | 8.4 | 70.8 | 1.52 | 1.77 | .67 | .40 | .83 | |
| FΣ (Hz) | 29 | 2.21 | 3.9 | 2.92 | .40 | .16 | .26 | .14 | .85 | .73 | .93 | |
| Fm-l (Hz) | 29 | 1.16 | 2.0 | 1.53 | .21 | .04 | .21 | -.51 | .78 | .58 | .89 | |
| Fa-p (Hz) | 29 | 1.01 | 1.9 | 1.40 | .20 | .04 | .25 | .71 | .84 | .71 | .92 | |
| STS | SΣ (mm) | 29 | 627.2 | 1146.4 | 846.8 | 132.4 | 17527 | .14 | -.54 | .79 | .62 | .90 |
| Sm-l (mm) | 29 | 349.2 | 618.8 | 499.2 | 85.4 | 7296 | -.32 | -1.09 | .80 | .63 | .90 | |
| Sa-p (mm) | 29 | 379.6 | 777.2 | 524.2 | 96.7 | 9344 | .58 | .18 | .78 | .60 | .89 | |
| Am-l (mm) | 29 | 17.1 | 41.9 | 25.9 | 5.6 | 31.8 | .88 | 1.16 | .73 | .50 | .86 | |
| Aa-p (mm) | 29 | 17.1 | 38.2 | 27.4 | 5.3 | 27.6 | .26 | -.62 | .46 | .00 | .73 | |
| FΣ (Hz) | 29 | 2.11 | 3.78 | 2.80 | .35 | .13 | .93 | 1.40 | .93 | .86 | .96 | |
| Fm-l (Hz) | 29 | 0.98 | 1.89 | 1.36 | .18 | .03 | .92 | 1.95 | .88 | .77 | .94 | |
| Fa-p (Hz) | 29 | 1.12 | 1.89 | 1.44 | .18 | .03 | .94 | .68 | .92 | .84 | .96 | |
| TAN | SΣ (mm) | 29 | 817.3 | 2206.0 | 1480.9 | 321.1 | 103124 | .28 | -.36 | .72 | .49 | .86 |
| Sm-l (mm) | 29 | 471.6 | 1434.5 | 863.3 | 203.1 | 41266 | .62 | .82 | .85 | .73 | .93 | |
| Sa-p (mm) | 29 | 505.0 | 1454.2 | 997.3 | 237.8 | 56552 | .17 | -.66 | .65 | .34 | .82 | |
| Am-l (mm) | 29 | 17.8 | 40.7 | 27.0 | 5.2 | 26.8 | .39 | .66 | .61 | .29 | .80 | |
| Aa-p (mm) | 29 | 18.8 | 122.6 | 39.7 | 18.8 | 351.6 | 3.23 | 13.82 | .21 | -.43 | .60 | |
| FΣ (Hz) | 29 | 2.75 | 4.34 | 3.46 | .36 | .13 | .21 | .14 | .89 | .81 | .95 | |
| Fm-l (Hz) | 29 | 1.24 | 2.11 | 1.62 | .18 | .03 | .40 | .74 | .90 | .81 | .95 | |
| Fa-p (Hz) | 29 | 1.48 | 2.23 | 1.83 | .20 | .04 | -.09 | -.59 | .87 | .75 | .93 | |
| CTA | SΣ (mm) | 29 | 983.9 | 1859.5 | 1379.3 | 240.1 | 57657 | .24 | -.54 | .76 | .56 | .88 |
| Sm-l (mm) | 29 | 506.8 | 1020.3 | 788.4 | 135.9 | 18462 | -.09 | -.37 | .78 | .60 | .89 | |
| Sa-p (mm) | 29 | 664.1 | 1372.5 | 928.4 | 193.9 | 37593 | .62 | -.05 | .75 | .54 | .88 | |
| Am-l (mm) | 29 | 20.3 | 56.2 | 28.2 | 6.8 | 45.9 | 2.68 | 10.07 | .52 | .13 | .75 | |
| Aa-p (mm) | 29 | 22.0 | 77.63 | 37.6 | 10.7 | 115.0 | 1.83 | 5.93 | .27 | -.39 | .64 | |
| FΣ (Hz) | 29 | 2.96 | 4.11 | 3.41 | .30 | .09 | .50 | -.42 | .85 | .72 | .92 | |
| Fm-l (Hz) | 29 | 1.29 | 2.02 | 1.57 | .17 | .03 | .59 | .10 | .84 | .71 | .92 | |
| Fa-p (Hz) | 29 | 1.58 | 2.10 | 1.85 | .15 | .02 | .09 | -.79 | .77 | .57 | .88 | |
| SL | SΣ (mm) | 29 | 1350.6 | 2657.2 | 1849.3 | 323.5 | 104658 | .63 | .36 | .86 | .74 | .93 |
| Sm-l (mm) | 29 | 862.8 | 1811.5 | 1187.3 | 230.6 | 53163 | .86 | .81 | .87 | .76 | .93 | |
| Sa-p (mm) | 29 | 772.6 | 1835.6 | 1185.8 | 234.6 | 55020 | .84 | 1.04 | .86 | .73 | .93 | |
| Am-l (mm) | 29 | 19.3 | 39.03 | 27.4 | 4.3 | 18.8 | .62 | .67 | .60 | .27 | .80 | |
| Aa-p (mm) | 29 | 25.3 | 49.60 | 37.5 | 6.2 | 38.7 | -.09 | -.77 | .29 | -.32 | .65 | |
| FΣ (Hz) | 29 | 3.19 | 4.17 | 3.71 | .24 | .06 | -.25 | -.11 | .69 | .43 | .85 | |
| Fm-l (Hz) | 29 | 1.59 | 2.16 | 1.87 | .14 | .02 | -.02 | -.31 | .67 | .39 | .84 | |
| Fa-p (Hz) | 29 | 1.54 | 2.05 | 1.84 | .13 | .02 | -.44 | -.38 | .71 | .47 | .85 |
The smallest effect of the SSS was recorded on the COP frequency parameters (FΣ, Fm-l, and Fa-p) with an increasing trend of the oscillations towards SL.
The largest positive skewness was observed for parameter Aa-p in TAN. This parameter also had a distinct conical distribution. This kind of trend was present also in CTA. Am-l was right asymmetrically distributed with an increased conical distribution.
The weakest intra-session repeatability (ICC) in all conditions was observed for Aa-p (Table 1). Am-l also proved to have poor repeatability (ICC ), while all other parameters exhibited good repeatability (majority of ICC values above 0.80), in particular for SΣ, Sm-l and Sa-p.
Discussion
In practice, BS parameters have to be sensitive to small manipulations of balance task difficulty or ever changing states of the locomotor system. The effects of changing SSS are routinely assessed in clinical practice to identify possible balance deficits (Emery, 2003). Differences due to changed SSS must be considered by physicians before the specific effects of pathology or exercise are interpreted. As seen in our study, maximal amplitudes and distance parameters of the COP, when using a single force plate, proved to be highly sensitive to small changes in SSS. This suggests that SSS has a major effect on BS parameters tested on healthy subjects.
Previous research showed that the use of a standardized measurement protocol can substantially improve the repeatability of the BS measurements (Brouwer et al., 1998; Emery, 2003; Elliott and Murray, 1998; Helbostad et al., 2004; Kamen et al., 1998; Korpelainen et al., 2005; Mattacola et al., 1995; Pincivero et al., 1995; Rogind et al., 2003), which might influence the sensitivity of the parameters used in our study. The duration of the individual trials was sufficient to achieve high repeatability (Sarabon et al., 2010a), indicating that an appropriate measurement protocol was used that avoided a significant contribution by inconsistencies.
In order for COP to be able to maintain a suitable COM position, it is necessary for the oscillation amplitude of COP to be larger than the oscillation amplitude of COM. As the COP oscillation amplitude might depend on the SSS (Winter, 1995; Winter et al., 2003) we would expect that a reduction in SSS would result in a decreased maximum of the COP oscillation amplitudes. In our study, however, if we look at the absolute values of the maximal COP amplitudes, we can see that COP oscillation remains markedly inside the SSS for all the foot positions. Therefore the assumption that when narrowing SSS limits would be divisive for COP amplitudes is probably not right. The conclusion can be drawn that the balance safety factor (the relationship between maximal COP amplitudes and the dimensions of the support surface) obviously decreases with a reduction of SSS. However, as demonstrated by the SL condition, reaches values which enable the subject to complete the balance task.
Our results showed that when the support surface is reduced, the SΣ, Sm-l, and Sa-p increase. We can speculate that this happens because of the need for a longer lever arm, in order to ensure the proper counter torque for the COM corrections, when the SSS is small. If the developed counter torque is not optimal, COM will oscillate over the natural vertical line, which will evoke a new demand for correction. As a result of this, COP amplitude and cumulative distance parameters will increase, possibly accompanied by a larger frequency of oscillation. Comparisons of the relative changes in COP average frequencies and cumulative distance parameters reveal very different trends. The increased cumulative distance parameters in our study therefore most probably reflect primarily the change in average oscillation amplitudes. This interpretation can be additionally supported by the kurtosis and skewness values which reveal conical and right asymmetrical distribution for amplitude and cumulative distance parameters, while frequency parameters showed more central profile of distribution. The distribution characteristics described present theoretically a bigger potential of the amplitude and amplitude-related parameters to respond in a positive direction.
Considering direction specifics, the most distinct change was observed in Sm-l, followed by Sa-p. In positions where the support surface has only been changed in the m-l direction, we would have expected that only Sm-l would change, but not Sa-p. However, interdependence between Sm-l and Sa-p has obviously arisen, a conclusion that is also supported by the high Pearson correlation coefficients between these two parameters in each individual stance (r > 0.9). Direction specific changes in foot positioning were not mirrored by direction specific COP distance changes. The same also applied to those balance tasks in which SSS had been changed in the a-p direction. When the SSS was increased in the a-p direction, both, the Sa-p and Sm-l were amplified. This was also the case for the opposite m-l reductions in SSS.
To a certain extent, these findings contradict those who reported on the mutually independent a-p and m-l COP movements, which could point to the independence among ankle-, hip- or load/unload balance strategies (Winter, 1995; Winter et al., 2003). In our study, we were unable to confirm independent changes in m-l and a-p BS. Several reasons might contribute to this observed discrepancy. First, plantar flexors considered responsible for a-p balance control (Benvenuti, 2001; Winter, 1995) function also as foot invertors and evertors. Their increased activity as stabilizers in the m-l direction may also cause additional Sa-p oscillation. Secondly, differences between the COP measurement methods used might also contribute. In our study, a single force plate was used while in the study performed by Winter et al., 2003 two force plates were used. Their measurement setup enabled them to monitor the COP of each leg individually and to show that this moved primarily in the a-p direction due to the activity of plantar and dorsiflexors. They monitored a common COP as well as the changes in weight bearing of individual legs. However, in explaining the m-l oscillation of the COP, they used predominantly a load/unload mechanism (Benvenuti, 2001; Winter et al., 2003). A comparison of their data indicates that mechanisms which maintain balance in the a-p and m-l directions are not correlated. In our study we used the common COP movement. Since the aforementioned study did not report on Sm-l and Sa-p parameters, direct comparisons about the direction specificity cannot be drawn. We assume that the total COP sway is influenced by a combination of ankle and load/unload mechanisms; which results in a simultaneous increase of oscillation in a-p as well as m-l directions.
The maximum oscillation amplitude, both in m-l and a-p directions, increased in accordance with the reduction in SSS. However, Am-l and Aa-p became more stable and no longer reached the highest values when SSS was reduced beyond SET and TAN respectively. The body had most likely reached its optimum oscillation amplitude, for which it is able to provide adequate torque for maintaining balance. The maximum oscillation amplitude is influenced by the m-l and a-p size of the support surface, but as it seems these are not the most significant factors. If the m-l and a-p SSS would have exerted a bigger influence, we would have expected the Am-l to be at its smallest in SL and TAN, however this does not happen. The body probably requires certain oscillation amplitude, in order to be capable of producing an adequate counter torque, regardless of the SSS. In stances with a wide foot placement the maximum oscillation amplitude was lower. Based on our results it can be concluded that in stances with a wide leg placement, the body is more stable or stiffer, and thus controls the BS in a better manner. On the other hand, the body becomes less stable with decreased stiffness when the feet are put closer together which is consistent with reports from other authors.(Benvenuti, 2001; Winter, 1995; Winter et al., 2003).
The oscillation frequency is a parameter which is percentage-wise least sensitive to increased levels of difficulty of the balance task. Factors which might increase the total frequency have been partly mentioned before in the analysis of the increase in oscillation amplitude. An upward trend in FΣ in accordance with the decreasing SSS was observed. However, in the same way as with all the COP distance parameters, the frequency likewise increases in both the m-l, as well as the a-p directions. Since neuro-muscular control of balance was shown to be related to increase in COP frequencies (Saffer et al., 2008; Winter et al., 1998), we can speculate that manipulating SSS in quiet stance balance tasks affects over this mechanism.
Conclusion
We can conclude that the selected BS parameters are sensitive to changes in SSS. Furthermore, the highest sensitivity proved to be in those COP parameters which describe amplitudes and cumulative distances of the COP. Additionally, our study suggests a clear interdependency between direction specific COP parameters for all the foot positions observed. In order to further the understanding of the ground reaction force based BS parameters, future studies should focus on investigating the interplay between the COP and load/unload parameters by testing the same subjects using a single force plate and by using a double force plate. Our data suggest that there are close relationships of the normalized COP parameters between different foot positions. However, since the group of subjects in our study was very homogeneous, further research should gather reference data for other relevant groups of subjects for whom balance is important. We believe namely that such an additional effort can result in an evidence based possibility to extrapolate the results among different SSS conditions in clinical practice.
If we wrap-up the results of the current study and those of our previous one, we can conclude the following: (i) the selected amplitude, frequency, and cumulative distance parameters of the COP movement in the quiet stance tasks are repeatable measures of balance, (ii) the method is sufficiently sensitive for detecting inter-individual differences, (iii) from these parameters, amplitudes of oscillation, resulting also in cumulative distance parameters, are the most sensitive to SSS manipulations, and (iv) direction specific changes in the SSS cause direction unspecific changes in COP movement. All these metric characteristics of the BS related parameters strongly depend nevertheless on the measurement protocol. Clinical and sport professionals, who use COP measurements for the evaluation of body balance, should realize that intra- and inter-session repeatability drops if durations shorter than 30s and/or fewer repetitions are used in testing (Pinsault and Vuillerme, 2009; Sarabon et al., 2010a; Salavati et al., 2009). Users should be aware that such an drop in reliability also endangers the sensitivity of the measurement method. We propose that an average of three 30 to 60-second repetitions should be used in order to gain a high enough repeatability that will be needed to study sensitivity. The same advice should be taken by the users in clinical practice who would like to test the effect of an intervention or of an injury on static balance.
Finally, future studies should focus on the sensitivity of these parameters to detect potential differences among subjects of different ages and gender, as well as the effects caused, for example, by the manipulation of vision and other sensory sub-systems, by COM redistribution, as well as the effects of training-, trauma- and other interventions.
Acknowledgements
The authors would like to acknowledge the support of the EU Interreg-IV A- Programme Österreich - Slowakei, Project No. SK-AT_080612_N0008 “Mobilität im Alter ”and Austrian national co-financing of the BM BWK.F.
Biographies

Sarabon Nejc
Employment
University of Primorska, Science and Research Center, Institute for Kinesiological Research , Slovenia.
Degree
PhD, PET-AT, BPT.
Research interests
Motor control and behavior, injury prevention using primarily electrophysiological and biomechanical diagnostic tools.
E-mail: Nejc.sarabon@zrs.upr.si

Rosker Jernej
Employment
Prevention and rehabilitation sports centre, Terme Krka, Terme Smarješke Toplice, Sloven.
Degree
PET.
Research interests
Sports injuries rehabilitation, coaching and biomechanical diagnostics in sports and rehabilitation.
E-mail: jernej.rosker@terme-krka.si

Stefan Loefler
Employment
Ludwig Boltzmann Institute for electrical stimulation and rehabilitation, Wien.
Degree
PhD.
Research interests
Sensorimotor and functional performance, rehabilitation, age and muscle weakness.
E-mail: stefan.loefler@wienkav.at

Helmut Kern
Employment
Institute for physical medicine and rehabilitation, Wilhelminenspital; Ludwig Boltzmann Institute for electrical stimulation and rehabilitation, Wien.
Degree
PhD.
Research interests
SPain therapy, physical rehabilitation, electrical stimulation on paraplegics and rehabilitation and training development in elderly.
E-mail: wil.pys.kern-forschung@wienkav.at
References
- Baczkowicz D., Szczegielnik J., Proszkowiec M.(2008) Relation between postural stability, gait and falls in elderly persons- preliminary report. Ortop Traumatol Rehabil 10(5), 478-485 [PubMed] [Google Scholar]
- Benvenuti F.(2001) Physiology of human balance. Advances in Neurology 87, 41-51 [PubMed] [Google Scholar]
- Brouwer B., Culham E.G., Liston R.A., Grant T.(1998) Normal variability of postural measures: implications for the reliability of relative balance performance outcomes. Scandinavian Journal of Rehabilitation Medicine 30, 131-137 [DOI] [PubMed] [Google Scholar]
- Chiari L., Rocchi L., Cappello A.(2002) Stabilometric parameters are affected by anthropometry and foot placement. Clinical Biomechanics 17, 666-677 [DOI] [PubMed] [Google Scholar]
- Danna-Dos-Santos A., Degani A.M., Latash M.L.(2008) Flexible muscle modes and synergies in challenging whole-body tasks. Experimental Brain Research 189, 171-187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott C., Murray A.(1998) Repeatability of body sway measurements; day-to-day variation measured by sway magnetometry. Physiological Measurement 19, 159-164 [DOI] [PubMed] [Google Scholar]
- Emery C.A.(2003) Is there a clinical standing balance measurement appropriate for use in sports medicine? A review of the literature. Journal of Science and Medicine in Sport 6, 492-504 [DOI] [PubMed] [Google Scholar]
- Gage W.H., Winter D.A., Frank J.S., Adkin A.L.(2004) Kinematic and kinetic validity of the inverted pendulum model in quiet standing. Gait & Posture 19, 124-132 [DOI] [PubMed] [Google Scholar]
- Gillette J.C., Abbas J.J.(2003) Foot placement alters the mechanisms of postural control while standing and reaching. IEEE Transactions on Neural Systems and Rehabilitation Engineering 11, 377-385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Helbostad J.L., Askim T., Moe-Nilssen R.(2004) Short-term repeatability of body sway during quiet standing in people with hemiparesis and in frail older adults. Archives of Physical Medicine and Rehabilitation 85, 993-999 [DOI] [PubMed] [Google Scholar]
- Kamen G., Patten C., Du C.D., Sison S.(1998) An accelerometry-based system for the assessment of balance and postural sway. Gerontology 44, 40-45 [DOI] [PubMed] [Google Scholar]
- Kirby R.L., Price N.A., Mac Leod D.A.(1987)The influence of foot position on standing balance. Journal of Biomechanics 20(4), 423-427 [DOI] [PubMed] [Google Scholar]
- Korpelainen R., Kaikkonen H., Kampman V., Korpelainen J.T.(2005) Reliability of an inclinometric method for assessment of body sway. Technology and Health Care 13, 115-124 [PubMed] [Google Scholar]
- Lamoth C.J., van Lummel R.C., Beek P.J.(2009) Athletic skill level is reflected in body sway: a test case for accelometry in combination with stochastic dynamics. Gait & Posture 29(4), 546-551 [DOI] [PubMed] [Google Scholar]
- Mattacola C.G., Lebsack D.A., Perrin D.H.(1995) Intertester Reliability of Assessing Postural Sway Using the Chattecx Balance System. Journal of Athletic Training 30, 237-242 [PMC free article] [PubMed] [Google Scholar]
- Nardone A., Godi M., Grasso M., Guglielmetti S., Schieppati M.(2009) Stabilometry is a predictor of gait performance in chronic hemiparetic stroke patients. Gait & Posture 30(1), 5-10 [DOI] [PubMed] [Google Scholar]
- Nault M.L., Allard P., Hinse S., Le Blanc R., Caron O., Labelle H., Sadeghi H.(2002) Relation between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine 27(17), 1977-1917 [DOI] [PubMed] [Google Scholar]
- Pincivero D., Lephart S., Henry T.(1995)Learning effects and reliability of the Biodex Stability System. Journal of Athlet-ics and Training 30, S35 [Google Scholar]
- Pinsault N., Vuillerme N.(2009) Test retest reliability of centre of foot pressure measures to assess postural control during unperturbed stance. Medical Engineering & Physics, 31, 276-286 [DOI] [PubMed] [Google Scholar]
- Popa T., Bonifazi M., Della Volpe R., Rossi A., Mezzocchio R.(2007) Adaptive changes in postural strategy selection in chronic low back pain. Experimental Brain Research, 177(3), 411-418 [DOI] [PubMed] [Google Scholar]
- Rogind H., Simonsen H., Era P., Bliddal H.(2003) Comparison of Kistler 9861A force platform and Chattecx Balance System for measurement of postural sway: correlation and test-retest reliability. Scandinavian Journal of Medicine & Science in Sports 13, 106-114 [DOI] [PubMed] [Google Scholar]
- Rocchi L., Chiari L., Cappello A.(2004) Feature selection of stabilometric parameters based on principal component analysis. Medical & Biological Engineering & Computing 42, 71-79 [DOI] [PubMed] [Google Scholar]
- Sarabon N., Kern H., Loefler S., Rosker J.(2010a) Selection of body sway parameters according to their sensitivity and repeatability. Basic and Applied. Myology 20, 5-13 [Google Scholar]
- Sarabon N., Mlaker B., Markovic G.(2010b) A novel tool for the assessment of dynamic balance in healthy individuals. Gait & Posture 31(2), 261-264 [DOI] [PubMed] [Google Scholar]
- Saffer M., Kiemel T., Jeka J.(2008) Coherence analysis of muscle activity during quiet stance. Experimental Brain Research 185(2), 215-226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salavati M., Hadian M.R., Mazaheri M., Negahban H., Ebrahimi I., Talebian S., Jafari A.H., Sanjari M.A., Sohani S.M., Parnianpour M.(2009) Test retest reliability of center of pressure measures of postural stability during quiet standing in a group with musculoskeletal disorders consisting of low back pain, anterior cruciate ligament injury and functional ankle instability. Gait & Posture 29, 460-464 [DOI] [PubMed] [Google Scholar]
- Tarantola J., Nardone A., Tacchini E., Schieppati M.(1997) Human stance stability improves with the repetition of the task: effect of foot position and visual condition. Neuroscience Letters 228, 75-78 [DOI] [PubMed] [Google Scholar]
- Winter D.A.(1995) Human balance and posture control during standing and walking. Gait & Posture 3, 192-214 [Google Scholar]
- Winter D.A., Patla A.E., Ishac M., Gage W.H.(2003) Motor mechanisms of balance during quiet standing. Journal of Electromyography and Kinesiology 13, 49-56 [DOI] [PubMed] [Google Scholar]
- Winter D.A., Patla A.E., Prince F., Ishac M., Gielo-Perczak K.(1998) Stiffness control of balance in quiet standing. Journal of Neurophysiology 80, 1211-1221 [DOI] [PubMed] [Google Scholar]
- Yim-Chiplis P.K., Talbot L.A.(2000) Defining and measuring balance in adults. Biological Research for Nursing 1, 321-331 [DOI] [PubMed] [Google Scholar]