

Abstract
The purpose was to determine if cold whirlpool treatment decreases functional performance equally regardless of gender. A secondary aim was to determine if there is a gradual increase in functional performance across time. Twenty-one college-aged subjects volunteered to participate in this study and were required to perform four measures of functional performance including: counter movement vertical jump, T-test, 36.58-meter dash (40-yard), and active range of motion of the ankle. Participants were treated with a 20 minute, 10 degree Celsius cold whirlpool following the pre-test of a given functional performance measure. Participants demonstrated significant decreases in counter movement vertical jump, T-test, and 40-yard dash performance immediately following treatment. Vertical jump performance remained impaired for at least 32 minutes. While both the T-test and 40-yard dash were affected for 7 and 22 minutes post- treatment, respectively. Participants also demonstrated significant decreases in peak power and average power immediately after and for 32 minutes post-treatment. Dorsiflexion was significantly decreased 7 and 12 minutes following treatment. There were no differences for plantar flexion, inversion, or eversion. These data suggest functional performance was affected immediately following and for up to 32 minutes after cold whirlpool treatment. It was also evident that there is a gradual performance increase for each measure of functional performance across time. Therefore, the consequences should be carefully considered before returning athletes to activity following cold whirlpool treatment.
Key points.
Cryotherapy is a common and highly effective modality in treating acute and chronic athletic injuries.
The results indicated that cold whirlpool does have an immediate and subsequent effect on functional performance.
Understanding how cold whirlpool adversely affects functional performance allows clinicians to continue using this modality before vigorous athletic activity.
Key words: Functional performance, cryotherapy, therapeutic modalities
Introduction
In the sports medicine setting, the use of cryotherapy is a widely accepted therapeutic modality. While the benefits of cryotherapy are agreed upon by many, there may be certain physiological changes which hinder performance. Several studies have aimed to establish if the use of cryotherapy adversely affects various measures which play a role in functional performance. These include proprioception (Ingersoll et al., 1992; LaRiviere and Osternig, 1994), power (Ferretti et al., 1992), strength (Mattacola and Perrin, 1993), speed (Bergh and Ekblom, 1979; Richendollar et al., 2006), and agility (Cross et al., 1996; Evans et al., 1995). Cryotherapy, has been shown to have no effect on joint position sense or sensory perception and therefore, proprioception appears to be unaffected by the use of cold in the treatment of athletic injuries (Ingersoll et al., 1992; LaRiviere and Osternig, 1994). Power and isokinetic strength, both appear to be decreased immediately following the application of various cryotherapeutic modalities (Ferretti et al., 1992; Hatzel and Kaminski, 2000; Mattacola and Perrin, 1993; Ruiz et al., 1993). However, most research pertaining to strength changes and cryotherapy has primarily been limited to isometric contractions (Johnson and Bahamonde, 1996; Mattacola and Perrin, 1993). The results of these studies, unfortunately, are equivocal and strength has been shown to increase (Mattacola and Perrin, 1993) and decrease (Johnson and Bahamonde, 1996). Speed and agility, both which are essential to athletic participation have not been studied in great detail (Bergh and Ekblom, 1979; Cross et al., 1996; Evans et al., 1995; Richendollar et al., 2006). Limited studies, however, have demonstrated that following a cold treatment in which muscle was directly cooled, functional performance may be impaired (Cross et al., 1996). Conversely, a cold treatment that only cools a joint may not adversely alter agility (Evans et al., 1995).
Previous literature examining functional performance and cryotherapy has primarily been limited to the effects of functional performance immediately, within minutes following cold application (Cross et al., 1996; Evans et al., 1995). While this is important, past research fails to take into account the effects of tissue re-warming and the subsequent effect on functional performance. Assuming tissue re-warming occurs, the immediate affects of the cold treatment should subside and a gradual increase in performance may occur. Often cryotherapy is used to offset the pain, swelling, and dysfunction associated with minor athletic trauma with athletes returning to activity shortly after treatment. Since many forms of cryotherapy are used by sports medicine clinicians before or during athletic participation, a more knowledgeable understanding of the immediate and delayed effects of cryotherapy on functional performance is necessary. Specifically, the cold whirlpool has become an increasingly popular modality due to its ability to treat larger areas, its analgesic massaging effect, the integration of therapeutic exercises, as well as all the benefits of cold. Therefore, our purpose was to investigate the effects of a cold whirlpool treatment on various measures of functional performance at subsequent time intervals following cold whirlpool treatment.
Methods
This research experiment used a repeated measures pretest-posttest design. Twenty-one, apparently healthy, participants who were recruited by word of mouth volunteered for this study (Table 1). Those who suffered a lower extremity injury in the past six months were excluded from this study. Furthermore, participants that indicated a contraindication to the use of cryotherapy (e.g. cold allergy, Raynaud’s phenomenon) or physical activity were excluded from this study. Informed consent and health history questionnaire forms were completed prior to participation and approval from the university’s institutional review board was also granted.
Table 1.
Sample descriptive statistics. Data are means (±SD).
| Gender | n | Age (yrs) |
Height (m) |
Weight (kg) |
Body Mass Index |
|---|---|---|---|---|---|
| Male | 7 | 19.4 (1.4) | 1.83 (.09) | 77.1 (10.9) | 23.0 (2.1) |
| Female | 13 | 20.0 (1.1) | 1.69 (.08) | 67.2 (11.3) | 23.4 (3.6) |
| Total | 20 | 19.8 (1.2) | 1.74 (.10) | 70.7 (11.9) | 23.3 (3.1) |
Procedures
Each participant reported to the athletic training facility on four separate occasions at least 48 hours apart to perform a given functional performance test. The four measures of functional performance were balanced across participants using a Latin Square design. All participants were first introduced and instructed on the performance test which they would be completing during a given testing session. Prior to a pre- test, each subject performed four to six practice trials of the test they would be performing (i.e. CMJ, T-test, or 40-yard dash) at a submaximal level, approximately 50%. The number of trial runs was based on a learning curve observed during a pilot study performed prior to data collection as well as past research (Evans et al., 1995). Subjects did not perform any practice trials of ankle AROM. After the practice trials, a rest period of 60s was given. Following the rest period, subjects preformed one pre-test. All subjects were instructed to give an all-out maximal effort. Immediately following the pre-test, subjects were escorted down a flight of stairs into the hydrotherapy room. Subjects were then instructed to sit comfortably on the tank top seat and maintain a bilateral immersion of their lower legs in the cold whirlpool for 20 minutes. The fibular head was denoted with an “x ”and subjects were required to keep this mark at the water level. Following the cold whirlpool treatment, subjects were given a towel to dry off and instructed to put their shoes and socks on as quickly as possible. As soon as each subject removed their lower legs from the cold whirlpool treatment, a hand-help stopwatch was started and used to monitor elapsed time following treatment. During a two minute period subjects were escorted up one flight of stairs to a field house where all measures of functional performance were tested. The first post-test began promptly at the two minute mark, while subsequent post-tests were completed every five minutes at the 7, 12, 17, 22, 27, and 32 minute marks following the cold whirlpool immersion. Between post test trials, subjects were not allowed to stretch in any manor. Subjects were allowed only minimal activity or relaxation in between test trials. Following the conclusion of a testing session, subjects were instructed when to return for further testing.
Each participant was required to perform four tests measuring functional performance: counter movement vertical jump test, 36.58-meter dash (40-yard), T- test, and active range of motion (AROM). The aim of these functional performance tests was to evaluate different aspects of performance required during athletic participation. Twenty participants completed the functional testing. One male participant withdrew from testing due to a hamstring injury sustained during the pre-test of the 40-yard dash. All participants were required to perform one functional performance test (e.g. vertical jump) during a given session. Testing sessions lasted approximately one hour.
Anaerobic power
To measure anaerobic power, we used a countermovement vertical jump (CMJ) test, which has been shown to produce greater power than other vertical jump tests (Harman et al., 1990). Maximum CMJ height was assessed using a Vertec™ (Sports Imports, Columbus, OH) vertical jump stand. The Vertec™ is a telescoping upright stand with colored plastic vanes. Each vane is spaced in 1.27 cm (½ inch) increments. Subjects were instructed to stand with their feet shoulder width apart and flat on the ground directly under the Vertec™ and reach up as high as possible. The standing reach height was determined from the height of the highest vane the subject was able to touch. To keep the starting feet position consistent, due to the fact that seven post tests were performed by each subject, a piece of tape was used to mark the starting position for each subject. Subjects jumped off of both legs as high as possible while reaching up to touch the vanes. Subjects were allowed one jump and the height of the highest vane touched was subtracted from the standing reach height, recorded, and used in the statistical analysis.
Peak power and average power generated during the CMJ were estimated using two separate equations. Johnson & Bahamonde (1996) developed two formulas for estimating peak power and average power output in university athletes. Both the peak (r = 0.88) and average power (r = 0.82) output were highly correlated with the derived equations and therefore, an acceptable means to estimate peak and average power output (Johnson and Bahamonde, 1996). The equations which best predicted peak power and average power are as follows (Johnson and Bahamonde, 1996):
| Ppeak (W) = 78.5 * VJ(cm) + 60.6 *mass(kg) - 15.3 * height(cm) - 1308 |
| Pavg (W) = 41.4 * VJ(cm) + 31.2 *mass(kg) - 13.9 * height(cm) + 431 |
Estimating the average or peak power during a vertical jump allows insight beyond the given performance, which is especially useful when comparing individuals of different somatotypes.
Speed
Straight sprint speed is most commonly measured using the 36.58-meter dash (40-yard) (Nitka, 2006; Pauole et al., 2000; Porcari et al., 1996). The 40-yard has been used in many different sports at many different levels to assess an athlete’s speed (Nitka, 2006). The 40-yard dash has demonstrated high intraclass reliability across trials indicating it is an acceptable means of measuring speed with only one trial (Pauole et al., 2000). A 40-yard lane was set-up on an indoor track surface and markers were placed at the start and finish. Prior to testing, all subjects lightly jogged one lap (200 M) as a warm-up followed by four to six trials at a submaximal level. No static or dynamic stretching of any kind was allowed. Following the practice trials, subjects were given a brief rest period of 60s prior to the pre-test. Times were measured using a hand-held stopwatch. All participants were instructed to start from a two-point standing position on the timer’s signal. The timer stood at the finish and recorded the time from the start of movement until the subject crossed the finish line.
Agility
Agility was measured using a standard T- test. The T-test has demonstrated high reliability across trials with a reliability coefficient of 0.98 indicating that only one trial is necessary to obtain a true T-test score (Pauole et al., 2000). This test was administered using the protocol outlined by Semenick, 1990. Four 22. 86 cm (nine inch) collapsible agility cones were arranged as shown in Figure 1. At the tester’s signal, the subject sprinted forward 9.14 M (10 yards) and touched the tip of the cone (B) with their right hand. Then they performed a lateral shuffle to the left 4.57 m (five yards) and touched the tip of the cone (C) with the left hand. Subjects then continued to shuffle 9.14 m (10 yards) to the right and touched the tip of the cone (D) with their right hand. They then shuffled 4.57 m (five yards) to the left and touched point B with their left hand. Finally, subjects back peddled 9.14 m (10 yards), passing through the finish at point A. Time was measured using a hand-held stopwatch.
Figure 1.
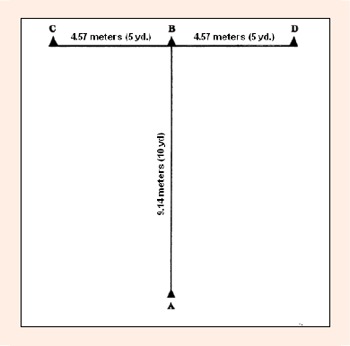
Diagram of the T-test.
Active range of motion
AROM was assessed on the subjects, self-reported dominate ankle (19 right foot dominate, 1 left foot dominate). Using a universal 30.48 cm (12 inch) goniometer, dorsiflexion, plantar flexion, forefoot eversion, and forefoot inversion were measured at the ankle. Clapper and Wolf, 1988 have found an intratester reliability of .92 for dorsiflexion and intratester reliability of .96 for plantar flexion using a universal goniometer. Inversion (r = 0.95) and eversion (r = 0.96) have been found to have high intratester reliability as well (Clapper and Wolf, 1988). Three measurements were taken in each direction by the primary author (S.M.P) and the average was recorded. All subjects sat in the short-sitting position (knees flexed to 90 degrees) at the end of a table. To ensure a more consistent measure, marks were placed on bony prominences to correctly align the goniometer during measurements. To accurately measure dorsiflexion and plantar flexion, the fulcrum of the goniometer was centered over the apex of the lateral malleolus, the stable arm was aligned with the fibular head, and the movable arm was kept parallel to the fifth metatarsal (Norkin and White, 2003). To measure forefoot inversion and forefoot eversion, the fulcrum of the goniometer was centered at the midpoint between the malleoli, the stable arm was aligned with the tibial tuberosity, and the movable arm was kept aligned with the second metatarsal (Norkin and White, 2003).
Treatment
Each participant was treated with a cold whirlpool immersion. The cold whirlpool temperature was maintained at 10° Celsius to emulate a standard athletic training room model. Temperature was closely monitored with a battery operated digital thermometer from Acu-Rite (Chaney Instrument Co., Lake Geneva, WI). The digital thermometer consisted of a 10 foot water-resistant wire with a submersible probe attached on the end and was accurate to the nearest tenth of a degree. The probe was placed near the bottom of the cold whirlpool and secured in place with tape. Each participant was immersed bilaterally to the fibular head (Figure 2) and instructed to maintain this position for the standard treatment time of twenty minutes. By choosing to immerse subjects to this level one major joint and muscle group were cooled. The whirlpool’s turbines were turned on and directed away from the subject’s lower legs.
Figure 2.

Cold whirlpool immersion.
Statistical analysis
All statistical procedures were completed using SPSS (Version 14.0, SPSS Inc. Headquarters, Chicago, IL). Means and standard deviations were calculated as descriptive statistics for age, height, weight, and body mass index (BMI). A repeated measures multivariate analysis of variance (MANOVA) was used to analyze agility (T-test), speed (36.58-meter dash), and power (CMJ) across time. Separate one-way repeated measures analysis of variance (ANOVA) procedures were used to analyze dorsiflexion, plantar flexion, eversion, inversion, average power, and peak power across time. Both average and peak powers were not included in the MANOVA because they are functions of the CMJ height. A preset alpha level of α = 0.05 was used for all statistical procedures. To maintain an overall significance level of α = 0.05 for each response, a Bonferroni corrected level of significance was used to compare each of the seven post-test measurements to the pre-test measurement for each dependent variable.
Results
Anaerobic power
Mean vertical jump scores demonstrated that the CMJ test was significantly lower than the pre-test CMJ height at all post tests following cold whirlpool immersion (Figure 3). Consequently, average power was significantly lower than the pre-test average power at all post tests following cold whirlpool immersion (Table 2). Peak power was also significantly lower than the pre-test peak power at all post tests following cold whirlpool immersion (Table 2).
Figure 3.
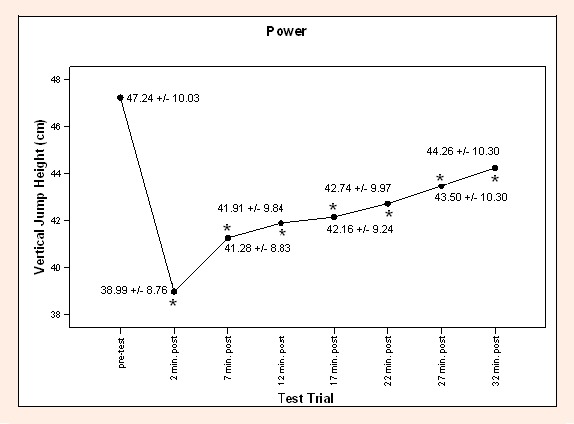
Mean vertical jump heights for males and females.
* Denotes p < 0.05 compared with pre-test. (* is not readable please resize legends in the figure)
Table 2.
Calculated peak and average power. Data are means (±SD).
| Time | Peak Power (W) | Average Power (W) |
|---|---|---|
| Pre-Test | 4020 (1078) | 2173 (518) |
| 2 minutes | 3372 (1028) * | 1831 (491) * |
| 7 minutes | 3552 (1036) * | 1925 (496) * |
| 12 minutes | 3602 (1112) * | 1952 (537) * |
| 17 minutes | 3622 (1073) * | 1962 (517) * |
| 22 minutes | 3666 (1087) * | 1986 (524) * |
| 27 minutes | 3726 (1128) * | 2017 (546) * |
| 32 minutes | 3786 (1116) * | 2049 (537) * |
* Denotes p < 0.05 compared with pre-test at the 0.05 level
Speed
Mean 40-yard dash times were significantly increased at 2, 7, 12, and 22 minutes following the cold whirlpool immersion than the pre-test time as shown in Figure 4. There were no differences in times during the 40-yard dash pre-test and 17, 27, and 32 minutes post cold whirl pool immersion.
Figure 3.
Mean vertical jump heights for males and females.
* Denotes p < 0.05 compared with pre-test. (* is not readable please resize legends in the figure)
Agility
Mean agility scores revealed a significant increase at 2 and 7 minutes following the cold whirlpool immersion (Figure 5). There were no differences between the agility pre-test and post tests at 12, 17, 22, 27, and 32 minutes.
Figure 5.
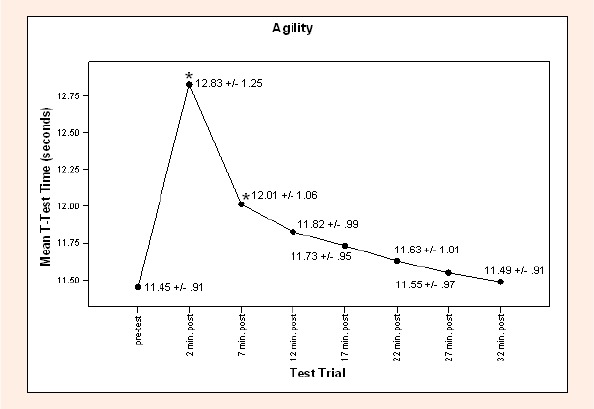
Mean T-test time for males and females.
* Denotes p < 0.05 compared with pre-test. (* is not readable please resize legends in the figure)
Active range of motion
Dorsiflexion was significantly lower than pre-test dorsiflexion at 7 and 12 minutes following treatment (P7min = 0.008, P12min = 0.026). There were no differences between dorsiflexion of the pre-test and post-tests at 2, 17, 22, 27, and 32 minutes following the cold whirlpool treatment. There were also no differences in plantar flexion, inversion and eversion.
Discussion
Our results indicated that a 20 minute, 10°C cold whirlpool treatment applied to the lower legs had an immediate and subsequent impairment on functional performance. CMJ heights, peak power, and average power were impaired for at least 32 minutes, thereby never reaching pre-test baseline levels. Both the T-test and 40-yard dash times were also impaired immediately after treatment and for at least 7 and 22 minutes following treatment, respectively. Dorsiflexion was decreased 7 and 12 minutes following cold whirlpool immersion, while plantar flexion, inversion, and eversion appeared to be unaffected by cold whirlpool immersion.
The immediate decreases in CMJ height, peak power, and average power were in agreement with several studies (Bergh and Ekblom, 1979; Cross et al., 1996; Evans et al., 1995; Ferretti et al., 1992; Gallant et al., 1996; Greicar et al., 1996; Markovic et al., 2004). In a similar study, Greicar et al., (1996) examined the effects of cryotherapy on functional performance immediately following treatment, 15, 30, and 45 minutes post treatment. Greicar’s (1996) examination of functional power noted immediately following a bilateral 20 minute, 1° C cold whirlpool immersion five centimeters above the superior pole of the patella, vertical jump height decreased by 31%. However, in the present study CMJ height was only decreased by 17.5% immediately following treatment. The delayed effects of cryotherapy on functional power at 15, 30, and 45 minutes post treatment were also significantly lower, vertical jump height was decreased by 18%, 14%, and 12%, respectively (Greicar et al., 1996). At similar time intervals (17 and 32 minutes post treatment) in the present study it was noted that vertical jump height was decreased by 10.8 % and 6.3 %, respectively. It appears there is a positive relationship between the muscle temperature and the height of a vertical jump. Bergh and Ekblom, 1979 best demonstrated this relationship finding the height of the jump decreased with a decrease in muscle temperature at a rate of 4.2% x degree C-1. Decreases in CMJ height can be attributed to changes in dynamic strength following the application of cold. Ruiz et al., 1993 contended ice caused a significant decrease in both concentric and eccentric quadriceps strength immediately following a 25 minute ice application. From this study, it appeared the decrease in concentric strength was of a short duration and no significant differences were found after moderate exercise, while eccentric strength was still significantly decreased following moderate exercise (Ruiz et al., 1993). Howard et al., 1994 investigated the use of ice immersion and strength and concluded that strength is impaired at higher movement velocities which are required during athletic activity.
The results of our study were also consistent with Greicar’s (1996) examination of agility using a carioca test and found immediately following the treatment that time was increased by 21%. The, more functional, T-test for agility demonstrated an increase of 10.8% immediately following treatment. However, there were no significant differences noted at 15, 30, or 45 minutes following treatment. Cross et al., 1996 also found a significant increase in shuttle run times from 6.54s to 6.71s immediately following a 20 minute 13° Celsius treatment leading the author’s to conclude cold applied to the lower leg and ankle does, indeed, have a detrimental effect on agility performance immediately following treatment. Therefore, it appeared that agility was affected immediately following cold application, but was unclear exactly when agility returned to baseline levels.
Contrary findings to our study also exist. In 1995, Evans et al. studied three different agility tests (carioca maneuver, co-contraction test, shuttle run) following a 20 minute, 1° Celsius ice immersion to the dominant foot and ankle, noting there were no significant differences between the control group and the ice immersion group, suggesting cryotherapy applied specifically to a joint may not alter agility. Furthermore, the results of our study also conflict with those of Knight et al., 1994 who found by cooling the foot and ankle, tricpes surae, or both via ice bag application functional agility (carioca maneuver, co-contraction test, shuttle run) was unaffected. Shuler et al., 1996 also reported cyrotherapy did not affect functional agility during a cutting task.
Speed, a component of agility, has not been studied in great detail. Bergh & Ekblom (1979) are the pioneer researchers who attempted to quantify the effects of muscle temperature on speed. They found sprint performance measured on a bicycle ergometer was significantly reduced with a decreased muscle temperature. In a study examining the effects of cold application on 40-yard dash, Richendollar et al., 2006 found the application of a cold pack to the anterior thigh decreased sprint times as well.
Along with changes in strength, the decreased agility and speed performance in our study can be attributed to increased joint and tissue stiffness. Cold application to connective tissue results in increased stiffness and decreased extensibility as temperatures decrease (Hunter and Willians, 1951). In the present study, the ankle joint was cooled along with the triceps surae complex. However, it was unclear whether joint stiffness was the result of connective tissue and muscle stiffness or if it was related to a thickening of joint synovial fluid. The literature indicates synovial fluid thickens in response to decreased temperature (Geisbrecht and Bristow, 1992; Hunter et al., 1952; Hunter and Willians, 1951). Consequently, Hunter et al., 1952, observed an increased resistance to movement in conjunction with a decrease in speed of movement caused by an increase in synovial fluid.
Functional performance decrements may also be related to the stretch-reflex phenomenon. As noted by Davies & Young (1983) the impaired ability of the muscle spindle to trigger the stretch-reflex may have decreased the amount of elastic potential which could be produced during the eccentric loading phase of muscular contraction. It was evident by the work of Bergh & Ekblom (1979) that muscular contraction speed and the capacity to generate force are reduced by cold.
The effect of cryotherapy on AROM is seldom investigated. However, significant deficits in ankle AROM due to the cold whirlpool immersion may hinder performance as a normal amount of AROM is required to complete sport-specific activities. All of the impairments noted in power, speed, and agility in the present study could be partially attributed to a decrease in AROM. However, dorsiflexion was decreased at 7 and 12 minutes following treatment and returned to baseline shortly thereafter. While plantar flexion, inversion, and eversion where not significantly affected. Other research investigating cold water immersion and delayed onset muscle soreness (DOMS) found no significant differences in AROM (Comeau and Potteiger, 2000; Kuligowski et al., 1998). Another investigation found a decrease in AROM and attributed it to collagen stiffness following the cold application (Gulick, et al., 1996).
For the aforementioned physiological effects of cryotherapy, functional performance was affected by cold’s negative influences (e.g. changes in strength, tissue stiffness, altered stretch-reflex). However, both the agility and speed functional performance tests returned to baseline levels much sooner than vertical jump. It is possible the quicker return to baseline times may be attributed to increased tissue rewarming through increased blood flow to the working muscles during exercise. Research has demonstrated moderate exercise significantly enhanced tissue rewarming (Myrer et al., 2001; Palmer and Knight, 1992). Myrer et al., 2001 noted 11 minutes following treatment, an ice-exercise group was .61°C colder than pretreatment levels while an ice-rest group was 8.05°C colder. Significant differences also existed 30 minutes following treatment. In the ice-exercise group, temperatures were .93°C colder than pretreatment compared to 6.95°C colder in the ice-rest group (Myrer et al., 2001). In our study, both the T-test and 40-yard dash trials took longer to complete than the CMJ. These longer times may have contributed to increased blood flow and consequently an increase in tissue temperatures and rewarming. Therefore, a more rapid incline of functional performance was evident. In a study examining the relationship between cryotherapy, active warm-up, and functional performance they concluded that a 6.5 minute warm-up was enough to negate the effects of a 20 minute crushed ice bag applied to the anterior thigh had on functional performance (Richendollar et al., 2006).
It should be noted that research has shown cold adaptation will occur, granted the modality is consistent in temperature and applied to the same area over several treatments (Carman and Knight, 1992). The participants in the present study were unaccustomed to the application of cryotherapy. Therefore, along with the physiological effect of cryotherapy some type of psychological effect may have also played a role in the decreased performance following treatment leading to a placebo effect. For example, subjects may have associated the cold whirlpool treatment with feeling stiff or uncoordinated and therefore, were apprehensive during movement resulting in decreases in performances. Further research is necessary in the area of functional performance on unaccustomed versus accustomed users of cryotherapy.
Other limitations to this investigation also exist. Fatigue may have played a roll in the trends of both speed and agility. However, based on our findings and the dependant variables chosen (anaerobic exercises) fatigue was most likely not a factor in the findings across time. A major limitation to this study is the uncertainty of muscle and joint temperatures. It was assumed the cold whirlpool treatment produced a therapeutic decrease in intramuscular and intraarticular temperatures. Consequently, the decreases in performance were attributed to the cold whirlpool treatment. Future research should examine the actual temperature produced during the treatment across time while these performance variables are measured. Furthermore, research should examine the effects body fat has as an insulator and accordingly functional performance.
Conclusion
Clinically, it should be acknowledged that following cryotherapy, an athlete will rarely go straight to maximal athletic performance. Traditionally, rehabilitation exercises may also be performed following treatment along with a thorough sub-maximal warm-up prior to engaging in vigorous activity. Our results demonstrated that power remained decreased for at least 32 minutes following treatment. While speed and agility returned toward baseline at the rate of 27 minutes and 12 minutes post treatment, respectively. If we had allowed our subjects to perform more vigorous activity, the decreases in functional performance may have been offset. Additionally, based on the present findings as well as past research the decreases in functional performance are likely dependant on the body area cooled as well as the temperature of the modality. Nonetheless our findings are not to be undervalued and sports medicine professionals should carefully weigh the consequences of returning athletes to strenuous activity immediately following cold whirlpool treatment.
Biographies
Stephen M. Patterson
Employment
Associate Athletic Trainer at Saint Cloud State University.
Degree
MSc
Research interests
The gender bias of ACL injuries and rehabilitation, lower extremity evaluation, cryotherapy and its effects on performance variables.
E-mail: smpatterson@stcloudstat.edu
Brian E. Udermann
Employment
Associate Professor in the Department of Exercise and Sports Science at the University of Wisconsin-La Crosse.
Degree
PhD
Research interests
Musculoskeletal Assessments of the Low Back.
E-mail: udermann.bria@uwlax.edu
Scott T. Doberstein
Employment
Head athletic trainer and senior lecturer in the department of Sports Science at the university of Wisconsin-La Crosse.
Degree
MSc
Research interests
Lower extremity injuries, therapeutic modalities, clinical evaluation techniques.
E-mail: doberste.scot@uwlax.edu

David M. Reineke
Employment
Associate Professor of Statistics at the University of Wisconsin - La Crosse.
Degree
PhD
Research interests
Applied statistics.
E-mail: Reineke.davi@uwlax.edu
References
- Bergh U., Ekblom B. (1979) Influence of muscle temperature on maximal muscle strength and power output in human skeletal muscles. Acta Physiologica Scandinavica 107, 33-37 [DOI] [PubMed] [Google Scholar]
- Carman K.W., Knight K.L. (1992) Habituation to cold-pain during repeated cryokinetic sessions. Journal of Athletic Training 27(3), 223-230 [PMC free article] [PubMed] [Google Scholar]
- Comeau M.J., Potteiger J.A. (2000) The effects of cold water immersion on parameters of skeletal muscle damage and delayed onset muscle soreness. Journal of Athletic Training 35(2), S46 [Google Scholar]
- Cross K.M., Wilson R.W., Perrom D.H. (1996) Functional performance following and ice immersion to the lower extremity. Journal of Athletic Training 31(2), 113-116 [PMC free article] [PubMed] [Google Scholar]
- Clapper M.P., Wolf S.L. (1988) Comparison of the reliability of the orthoranger and the standard goniometer for assessing active lower extremity range of motion. Physical Therapy 68, 214. [DOI] [PubMed] [Google Scholar]
- Davies C.T.M., Young K. (1983) Effect of temperature on the contractile properties and muscle power of triceps surae in humans. Journal of Applied Physiology 55, 191-195 [DOI] [PubMed] [Google Scholar]
- Elveru R.A., Rothstein J., Lamb R.L. (1988) Goniometric reliability in a clinical setting: subtalar and ankle joint measurements. Physical Therapy 68, 672. [DOI] [PubMed] [Google Scholar]
- Evans T.A., Ingersoll C.D., Knight K.L., Worrell T. (1995) Agility following the application of cold therapy. Journal of Athletic Training 30(3), 231-233 [PMC free article] [PubMed] [Google Scholar]
- Ferretti G., Ishii M., Moia C., Cerretelli P. (1992) Effects of temperature on the maximal instantaneous muscle power of humans. European Journal of Applied Physiology 64, 112-116 [DOI] [PubMed] [Google Scholar]
- Gallant S.G., Knight K.L., Ingersoll C.D., Kovaleski J.E. (1996) Cryotherapy effects on leg press and vertical jump force. Journal of Athletic Training 31, S18 [Google Scholar]
- Geisbrecht G.G., Bristow G.K. (1992) Decrement in manual arm performance during whole body cooling. Aviation Space Environmental Medicine 63, 1077-1081 [PubMed] [Google Scholar]
- Greicar M., Kendrick Z., Kimura I. (1996) Immediate and delayed effects of cryotherapy on functional power and agility. Journal of Athletic Training 31, S32 [Google Scholar]
- Gulick D.T., Kimura I.F., Sitler M., Paolone A., Kelly J.D. (1996) Various treatment techniques on signs and symptoms of delayed onset muscle soreness. Journal of Athletic Training 31(2), 145-152 [PMC free article] [PubMed] [Google Scholar]
- Harman E.A., Rosenstein M.T., Frykman P.N., Sosenstein R.M. (1990) The effects of arms and countermovement on vertical jump. Medicine and Exercise in Sports and Exercise 22 (6), 825-833 [DOI] [PubMed] [Google Scholar]
- Hatzel B.M., Kaminski T.W. (2000) The effects of ice immersion on concentric and eccentric isokinetic muscle performance in the ankle. Isokinetic Exercise Science 8(2), 103-107 [Google Scholar]
- Howard R.L., Kraemer W.J., Stanley D.C., Armstrong L.E., Maresh C.M. (1994) The effects of cold immersion on muscle strength. The Journal of Strength and Conditioning Research 8(3), 129-133 [Google Scholar]
- Hunter J., Kerr E.H., Whillans M.G. (1952) The relationship between joint stiffness upon exposure to cold and the characteristics of synovial fluid. Canadian Journal of Medicine and Science 30, 367-377 [DOI] [PubMed] [Google Scholar]
- Hunter J., Willians M.G. (1951) A study of the effects of cold on joint temperature and mobility. Canadian Journal of Medicine and Science 29, 255-262 [DOI] [PubMed] [Google Scholar]
- Ingersoll C.D., Knight K.L., Merrick M.A. (1992) Sensory perception of the foot and ankle following therapeutic applications of heat and cold. Journal of Athletic Training 2, 231-234 [PMC free article] [PubMed] [Google Scholar]
- Johnson D.L., Bahamonde R. (1996) Power output estimate in university athletes. Journal of Strength and Conditioning Research 10(3), 161-166 [Google Scholar]
- Knight K.L., Ingersoll C.D., Trowbridge C., Connolly T.O., Cordova M.L., Hyink L.L., Wlech S.M. (1994) The effects of cooling the ankle, the triceps surae, or both on functional agility. Journal of Athletic Training 29(2), 165 [Google Scholar]
- Kuligowski L.A., Lephart S.M., Giannantonio F.P., Blanc R.O. (1998) Effect of whirlpool therapy on the signs and symptoms of delayed-onset muscle soreness. Journal of Athletic Training 33(3), 222-228 [PMC free article] [PubMed] [Google Scholar]
- LaRiviere J.A., Osternig L. (1994) The effects of ice immersion of joint position sense. Journal of Sport Rehabilitation 3, 58-67 [Google Scholar]
- Markovic G., Dizdar D., Jukic I., Cardinale M. (2004) Reliability and factorial validity of squat and countermovement jump tests. Journal of Strength and Conditioning Research 18(3), 551-555 [DOI] [PubMed] [Google Scholar]
- Mattacola C.G., Perrin DH. (1993) Effects of cold water application on isokinetic strength of the planter flexors. Isokinetic Exercise Science 3, 152-159 [Google Scholar]
- McGowin H. (1976) Effects of cold application on maximal isometric contraction. Physical Therapy Review 47, 185-192 [DOI] [PubMed] [Google Scholar]
- Myrer J.W., Myrer K.A., Measom G.J., Fellingham G.W., Evers S.L. (2001) Muscle temperature is affected by overlying adipose when cryotherapy is administered Journal of Athletic Training 36(1), 32-36 [PMC free article] [PubMed] [Google Scholar]
- Nitka M. (2006) The forty-yard dash for the high school athlete. Strength and Conditioning Journal 28(2), 24-25 [Google Scholar]
- Norkin C.C., White D.J. (2003) Measurement of joint motion: A guide to goniometry. 3rd edition F.A.Davis Company, Philadelphia [Google Scholar]
- Palmer J.C., Knight K.L. (1992) Ankle and thigh skin surface temperature changes with repeated ice pack application. Journal of Athletic Training 27, 319-323 [PMC free article] [PubMed] [Google Scholar]
- Pauole K., Madole K., Garhammer J., Lacourse M., Rozenek R. (2000) Reliability and Validity of the T-test as a measure of agility, leg power, and leg speed on college-aged men and women. Journal of Strength and Conditioning Research 14(4), 443-450 [Google Scholar]
- Porcari J.P., Pethan K.P., Ward K., Fater D., Terry L. (1996) Effects of training in strength shoes on 40-yard dash time, jumping ability, and calf girth. Journal of Strength and Conditioning Research 10(2), 120-123 [Google Scholar]
- Richendollar M.L., Darby L.A., Brown T.M. (2006) Ice bag application, active warm-up, and 3 measures of maximal functional performance. Journal of Athletic Training 41(4), 364-370 [PMC free article] [PubMed] [Google Scholar]
- Ruiz D.H., Myrer J.W., Durrant E., Fellingham G.W. (1993) The effect of cryotherapy on concentric and eccentric strength in the quadriceps muscle after sequential bouts of exercise. Journal of Athletic Training 28, 320-323 [PMC free article] [PubMed] [Google Scholar]
- Semenick D. (1990) The T-Test. NSCA Journal 12(1), 36-37 [Google Scholar]
- Shuler D.E, Ingersoll C.D., Knight K.L., Kuhlman J.S. (1996) Local cold application to the foot and ankle, lower leg, or both effects on a cutting drill. Journal of Athletic Training 31(2), S35 [Google Scholar]