

Abstract
This study aimed to investigate the influence of prophylactic ankle taping on two balance tests (static and dynamic balance) and one jump test, in the push off and the landing phase. Fifteen active young subjects (age: 21.0 ± 4.4 years) without previous ankle injuries volunteered for the study. Each participant performed three tests in two different situations: with taping and without taping. The tests were a counter movement jump, static balance, and a dynamic posturography test. The tests and conditions were randomly performed. The path of the center of pressures was measured in the balance tests, and the vertical ground reaction forces were recorded during the push-off and landing phases of the counter movement jump. Ankle taping had no influence on balance performance or in the push off phase of the jump. However, the second peak vertical force value during the landing phase of the jump was 12% greater with ankle taping (0.66 BW, 95% CI -0.64 to 1.96). The use of prophylactic ankle taping had no influence on the balance or jump performance of healthy young subjects. In contrast, the taped ankle increased the second peak vertical force value, which could be related to a greater risk of injury produced by the accumulation of repeated impacts in sports where jumps are frequently performed.
Key points.
Ankle taping has no influence on balance performance.
Ankle taping does not impair performance during the push-off phase of the jump.
Ankle taping could increase the risk of injury during landings by increasing peak forces.
Key words: Biomechanics, propioception, force platform, ground reaction forces, center of pressure
Introduction
Ankle sprains represent from 38 to 50% of the total sport injuries (Jones et al., 2000; Leaf et al., 2003; Thacker et al., 1999; Verbrugge, 1996). Garrick and Requa, 1988 estimated that one-sixth of the total time lost by sport injuries was attributed to ankle sprains. Functional taping and ankle braces are passive preventive measures frequently utilised in sports (Osborne and Rizzo, 2003; Robbins and Walked, 1998). Studies on the influence of functional taping on sports tasks during actual competition are scarce (McCaw and Cerullo, 1999; Riemann et al., 2002), and most of them only analyse the passive ROM restriction (Hume and Gerrard, 1998). The studies that analyse jump tests and static balance are the most common among those that assess the influence of ankle taping on performance tasks in sports (Hume and Gerrard, 1998; Cordova et al., 2002). Research that studied jump performance focused on the changes in jump height with taped subjects (Burks et al., 1991; Mackean et al., 1995; Verbrugge, 1996). Some of them reported decreases in jump performance (Burks et al., 1991; Mackean et al., 1995; Verbrugge, 1996), but this remains a controversial issue.
In addition, a few studies have analysed drop landings and functional taping (McCaw and Cerullo, 1999; Riemann et al., 2002), showing decreases in the time to dissipate landing forces and adverse effects on the landing kinematics. The risk of ‘overuse’ injuries will increase if the ability to reduce landing forces is impaired by limiting the mobility of the lower extremities (Dufek and Bates, 1991; Hewett et al., 2005).
The studies on balance have focused on the centre of pressure (COP) trajectories to evaluate performance (Bennell and Goldie, 1994; Cordova et al., 2002; Feuerbach and Grabiner, 1993; Hertel et al., 1996; Kinzey et al., 1997; Paris, 1992). Better performance is shown by shorter trajectories or narrower areas of the COP. Nonetheless, some authors have utilised less accurate methods to evaluate balance, such as counting the number of times the subject needed to keep his balance (Bennell and Goldie, 1994), or the time spent by the subject on a fixed bar (Paris, 1992). There are contradictory results on the influence of preventive ankle taping on balance tests. Hertel et al., 1996 found no differences between subjects with and without taping in three balance tests. One of them was performed with static monopodal stance and the other two were dynamic tests. However, other authors such as Bennell and Goldie, 1994 concluded that ankle taping led to a decreased postural control in similar balance tests.
Therefore, studies on the effects of ankle taping during specific movements, such as jumps or balance tasks, are scarce, and its influence on sports performance is controversial. The present study analysed the changes in ground reaction forces and the path of the COP during balance tests. The performance of taped subjects during static and dynamic balance tasks could be improved by the increase in exteroceptive input provided by the taping (Feuerbach and Grabiner, 1993). From previous studies, we hypothesised that prophylactic ankle taping on uninjured subjects would decrease their jump performance and increase the peak vertical forces during the landing phase. On the other hand, we expected an increase in the subjects’ performance in the balance tasks, especially in the static balance tests. More biomechanical research on the effects of functional taping on sports performance is necessary to clarify its effects during actual sports tasks. Therefore, the research question of this study was: does prophylactic ankle taping influence on performance of two balance tests (static and dynamic balance) and the push off and landing phase of one jump test?
Methods
Design
The subjects performed the experiment in three different days. In the first session, anthropometric measurements and a clinical assessment of the subjects’ ankles were performed. The second day was used to familiarise the subjects with the test protocols, and the balance and jump tests were performed on the third day. Sessions 2 and 3 were separated by no more than one week. Before participation, all the subjects were informed of the risks associated with the experimental protocol and they were asked to sign a written consent form approved by the Institutional Review Board of the Faculty of Sports Sciences of the University of Castilla-La Mancha.
Participants
Fifteen physically active subjects, seven men and eight women, volunteered for the study. Their physical characteristics are given in Table 1. The participants are regularly involved in recreational sports, at least twice a week, but none of them had competed professionally. None of the subjects have used ankle taping or bracing (Bennell and Goldie, 1994) or have had lower limb injuries in the last 6 months (Greene and Hillman, 1990; Gross et al., 1991). An experienced physiotherapist confirmed this information with a medical history and a physical examination, including ligamentous and range-of-motion tests one week before testing. The subjects performed all the tests with indoor court shoes.
Table 1.
Characteristics of the participants in the study. Data are means (±SD).
| Age (years) | 21.0 (4.4) |
|---|---|
| Height (m) | 1.72 (.09) |
| Body mass (kg) | 71.1 (11.4) |
| Lower limb length (cm) | 87.5 (6.8) |
| Fat free mass (kg) | 59.9 (12.0) |
Intervention
The anthropometric characteristics were determined using a calibrated scale with height rod (Seca Ltd, Hanover, Germany), an anthropometer (GPM, SiberHegner Ltd., Zurich, Switzerland), a 1.5-m flexible tape (Holtain, Croswell, Crymmych, UK), a bicondylar caliper (GPM, SiberHegner Ltd., Zurich, Switzerland), and skinfold calipers (Holtain, Croswell, Crymmych, UK). Fat mass was calculated from six skinfold measurements (triceps, subscapular, umbilicus, suprailium, thigh, and lower leg) according to the equations of Carter, 1982. Fat free mass (FFM) was calculated by subtracting fat mass from total mass and muscular mass (expressed as a percentage of total mass) was calculated by subtracting bone and residual mass from FFM.
A prophylactic taping, modified Gibney closed-basket-weave (Wilkerson, 1991) (designed for subjects without previous ankle injuries to restrict ankle inversion) was done in both ankles by a physiotherapist, with a prewrap, to protect the Achilles tendon and restrict ankle inversion. Two adhesive anchors were applied to the skin according to the subjects’ body dimensions (Figure 1). The inferior adhesive anchor was applied over the metatarsal head with six active strips that limited ankle inversion, and 13–17 strip locks were utilised, depending on the size of the lower limb.
Figure 1.
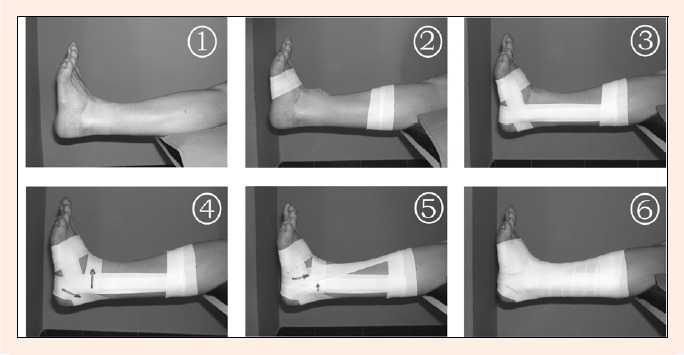
Ankle taping procedure. The superior anchor (second photo) was applied in a standardised way according to the subject’s body dimensions, at 35% of the distance from the lateral malleolus to the fibula head.
Each participant performed the three tests in two different situations: with taping (T) and without taping (NT). The tests were as follows: countermovement jump (Figure 2), static balance (Figure 3), and a dynamic posturography test (Figure 4). The tests and conditions (T-NT) were randomly performed. Static balance tests were performed on a force platform (Piezoresistive force platform Dinascan 600M; IBV, Valencia, Spain). The force data were digitally converted and stored in a computer for subsequent analysis using the software Estabilometría (IBV, Valencia, Spain). The force-time data from the countermovement jump were assessed on a Quattro Jump Portable Force Plate System (Kistler, Winthertur, Switzerland) at 500 Hz. This sample rate has been previously utilised for assessing landings in the studies of Hopper et al., 1999 and Ozguven and Berme (1988). The forces were normalised and expressed as times body weight (BW). A standardised 10-min warm-up was carried out by the participants before each session. The warm-up consisted of 5 min at 175 W on a cycle ergometer Ergomedic 894 Ea (Monark, Varberg, Sweden), stretching of the lower limb muscles directed by the researcher, and six jumps (three submaximal and three maximal).
Figure 2.
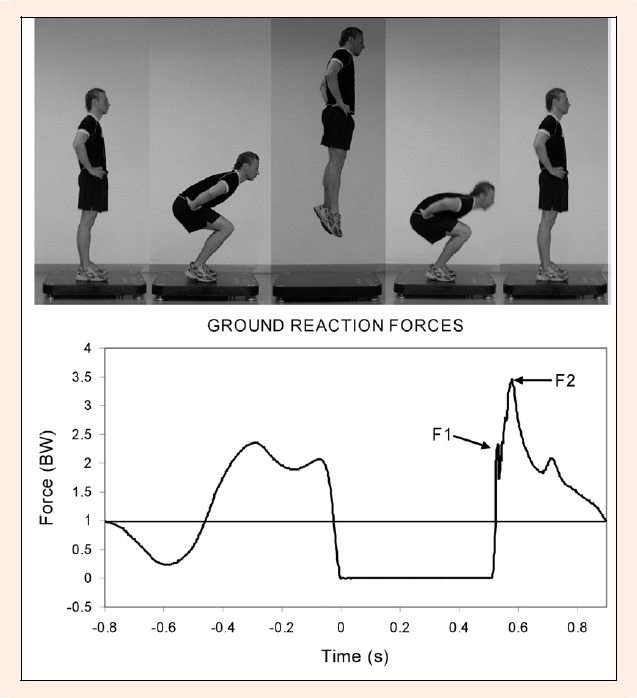
Sequence and force-time data from a countermovement jump. The first (F1) and second (F2) peak vertical force values in the landing phase are shown.
Figure 3.
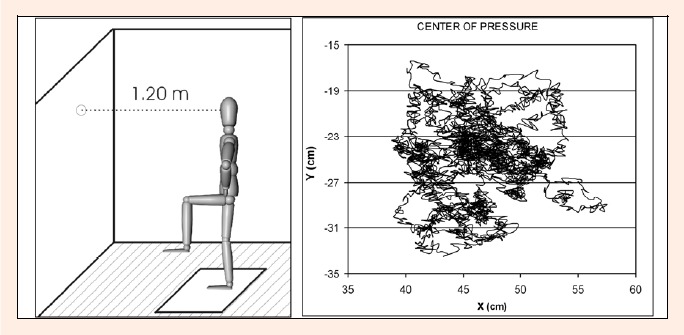
Subject’s position (left) and path of the centre of pressures (right) during the static balance test.
Figure 4.
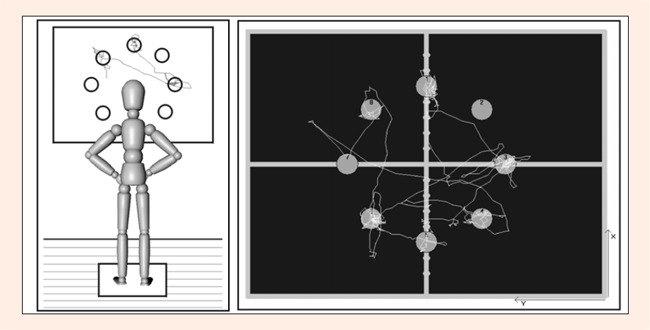
Schematic illustration of the postural sway test (left) and typical representation of the path of the centre of pressures on the force platform (right).
Outcome measures
Countermovement jump: The subjects performed the test on the force platform with the hands placed on the hips during the whole jump. The knee angle during the counter movement was not controlled. The participants performed three valid trials and the one with the greatest jump height was recorded for further analysis (Figure 2). The variables analysed during the push-off phase of the jump test were jump height (h), from the flight time, peak vertical forces (PF) and peak power (PP), obtained from the integration of the force-time record. In addition, in the landing phase, we analysed the first and second peak vertical force values (F1 and F2), the time that elapsed from the feet contact to F1 and F2 (T1 and T2, respectively), and the time from feet contact until the vertical ground reaction forces reached the subject’s weight for the first time after the landing movement (TBW).
Static balance on monopodal stance: The subjects had to remain as still as possible standing on the right leg, with the left lower limb at 90° of hip and knee flexion, during 15 s. Their hands had to be placed on the hips throughout the test, and the feet were placed in the same location on the plate in all the trials. The aim of the test was to keep to the minimum the area in which the movement of the subject was taking place, defined by the trajectory of the COP (Figure 3).
The variables analysed were the area covered by the COP and the average position in the antero- posterior axis (average of X values) and medial-lateral axis (average of Y values). Three trials were completed and the best performance, that is, the one with the lower area, was recorded for subsequent statistical analysis.
Postural sway test: Dynamic balance was measured using computerised dynamic posturography: the subjects were in standing position on a force platform with hands on hips, and balance was assessed by modifying visual feedbacks and asking the participants to score a circle as fast and as accurately as possible in response to the changes in the visual feedback by moving their bodies. Eight red circles, projected in a wide screen in front of the subject, were randomly lit for periods of 4-6 s. The test lasted 40 s. The analysis of the transitional period from one lit centre to another included the calculation of the time to reach the lit centre and the percentage of the time during which the subject remained inside the centre as a percentage of the overall time of the lighting of the centre (hits). The best of three trials, that is, the one with the longest time into the target, was recorded for subsequent analysis (Figure 4).
All the variables analysed were recorded from the best trials because we aimed to compare maximal performance and not patterns obtained by averaging the data from several trials (Bosco et al., 1999; Macpherson et al., 1995).
The reliability of the main variables was assessed with the intraclass correlation coefficient (ICC) and the typical error, from three measurements of each variable (Hopkins, 2000). In a pilot study, carried out with six subjects, the ICCs were very high for all the variables (0. 94-0.99). Typical errors in the jump height, F2 value, area covered by COP in the test of the static balance on monopodal and hits from the postural sway test were 0.16 cm, 0.11 BW, 7.37 cm2 and 2. 47%, respectively.
Data analysis
Based on the data obtained in a pilot study, the minimal number of subjects required with a power of 0.8 and a level of significance α of 0.05 was calculated to be 14, considering differences in F2 between T and NT. Descriptive statistics included mean and standard deviations; relationships between variables were examined using Spearman´s correlation test. Differences between T and NT conditions were assessed with the Wilcoxon matched-pair test. Significance was accepted at the level of P < 0.05.
Results
Tables 2 and 3 show the means, standard deviations, percentage differences, and the levels of significance of the variables studied in the balance and jump tests, respectively. There were only significant differences in the average of X values in the static balance test (3.23 cm, 95% CI -1. 28 to 7.74) and in the F2 value of the landing (0.66 BW, 95% CI -0.64 to 1.96), with greater values noted in the T condition in both cases.
Table 2.
Differences between taped and untaped conditions in terms of balance performance variables. Data are means (±SD).
| Balance tests | |||||
|---|---|---|---|---|---|
| Postural sway | Static balance | ||||
| Time (s) | Hits (%) | Average X (cm) | Average Y (cm) | Area (cm2) | |
| NT | 2.125 (.273) | 60.00 (10.89) | 40.2 (5.1) | -30.3 (19.0) | 88.17 (50.09) |
| T | 2.284 (.271) | 60.23 (11.90) | 43.4 (6.9) * | -27.1 (17.9) | 91.14 (38.88) |
| % difference | 7.55 | .37 | 8.05 | 10.60 | 3.36 |
NT = without ankle taping; T = with ankle taping
* = p < 0.05
The most important correlations between the T and NT conditions are shown in Table 4. There were significant correlations among variables in all the tests, with the exception of the postural sway test. There was a significant negative correlation between F2 and T2 in both conditions (T: r = -0.66 (95% CI -0.88 to -0.23), p < 0.01; NT: r = -0.58, (95% CI -0.85 to -0.10), p < 0.05).
Table 4.
Main correlations found between the taped and untaped conditions.
| Variable | r |
|---|---|
| Static balance area | .80 *** |
| PF | .73 ** |
| PP | .92 *** |
| h | .98 *** |
| F1 | .93 *** |
| F2 | .87 *** |
| T1 | .61 * |
| T2 | .83 *** |
| TBW | 1.00 *** |
Static balance area = area covered by the centre of pressures during the static balance test; PF = peak vertical force; PP = peak power; h = jump height; F1 = first peak vertical force value; F2 = second peak vertical force value; T1 = time elapsed from contact to F1; T2 = time elapsed from contact to F2; TBW = time from feet contact until the vertical ground reaction forces reach the subject´s weight for the first time after the landing
* p < 0.05
** p < 0.05
p < 0.001
Discussion
In the T condition, there were no performance decreases in the balance tests (Table 2). These results agree with the studies of Hertel et al., 1996 and Paris, 1992, who found no differences between taped and untaped subjects in static balance tests. Nonetheless, Bennell and Godie (1994) reported performance decreases with ankle taping, whereas Feuerbach and Grabiner, 1993 found performance improvements. This discrepancy could be explained by the different body positions during the balance tests. For example, the subjects of Bennell and Goldie carried out the test with the free leg 10 cm above the ground level and with their eyes closed, a less stable situation than the one utilised in the present study. In addition, there were differences in the ankle taping influence on the subjects in the static and dynamic balance tests: in the static test, the pressure on the ankle by the taping could increase the exteroceptive inputs and therefore improve balance control; however, in the dynamic test, the ROM restriction imposed by the taping could decrease the balance performance. The differences found in the average position of X values during the static balance test between the T and NT conditions showed that ankle taping slightly modified the position of the COP during the test and led to a performance decrease in this test, although the differences in the area covered by the COP were not significant. The correlations found in all the tests, with the exception of postural sway, showed that ankle taping would have a similar influence over all the subjects (Table 4).
Contrary to previous reports (Burks et al., 1991; Mackean et al., 1995; Verbrugge, 1996), there were no performance decreases during the push-off phase of the jump. The studies that have found lower jump heights with taping used jump tests with arm swing, without a standardisation of the arm or body movement before the push-off phase. The subjects in the present study started from still position and were not allowed to perform any preparatory movements before the jump. The ankle taping might have a different degree of influence, depending on the jump test utilised. The restriction produced by the taping in the movements of the push-off phase and the greater coordination required in the less standardised jump tests, and even in those performed in actual competitions, could lead to lower jump heights compared with the jump tests performed from still position and without arm swing because the jump tests performed in the present study did not include preparatory movements like lateral or forward displacements before the push-off phase.
There was an increase of 0.66 BW (95% CI -0.64 to 1.96) in F2 values in the T condition. The higher F2 values may be associated with a greater risk of injury (Dufek and Bates, 1991; Hewett et al., 2005; Louw et al., 2006) because, in actual competitions, the unpredictable environment (team mates, the ball, the opponents, etc.) makes it difficult to focus attention on the landing movement. Therefore, it is very important to have automated movement patterns and avoid large peak forces during the landings while the subjects are focusing their attention on other aspects of the game. The participants of the present study had no previous experience with ankle taping and the results may have been different if they were accustomed to wearing ankle taping.
There was a low but significant negative correlation between F2 and T2 (T: r = -0.66, p < 0.01 and NT: r = -0.58, p < 0.05). If the ankle plantarflexors do enough eccentric work during the first moments after feet contact, F2 will appear later in the force-time record, and the F2 value will be lower because part of the force will have been absorbed by the plantarflexor muscles and, therefore, this peak value will be delayed in time. Most types of ankle tapings limit the ankle plantarflexion ROM, which can increase even more the F2 value.
Conclusion
In conclusion, the use of prophylactic ankle taping had almost no influence on the balance or jump performance of healthy young subjects. In contrast, ankle taping could increase the risk of injury during landings because the peak forces were increased in the taped condition. This fact points to a proper use of ankle taping, only when it is required, like in those instances where alternative methods such as propioception, technique training, or strengthening of the ankle stabilizer muscles have failed. Future research should evaluate the effects of landing training on the force values to teach subjects who need ankle taping to decrease the vertical force values and, consequently, the risk of injury.
Table 3.
Differences between taped and untaped conditions in the counter movement jump test. Data are means (±SD).
| Jump tests | ||||||||
|---|---|---|---|---|---|---|---|---|
| Push off phase | Landing phase | |||||||
| PF (BW) | PP (W/kg) | h (cm) | F1 (BW) | F2 (BW) | T1 (s) | T2 (s) | TBW (s) | |
| NT | 2.48 (.23) | 46.92 (9.90) | .33 (.10) | 2.49 (.94) | 5.38 (1.61) | .017 (.009) | .057 (.023) | .350 (.169) |
| T | 2.52 (.29) | 45.82 (8.18) | .32 (.10) | 2.41 (1.22) | 6.04 (1.87) * | .013 (.005) | .052 (.019) | .327 (.143) |
| % difference | 1.37 | 2.35 | .98 | 3.28 | 12.35 | 23.62 | 6.43 | 16.88 |
NT = without ankle taping; T = with ankle taping; PF = peak vertical force; PP = peak power; h = jump height; F1 = first peak vertical force value; F2 = second peak vertical force value; T1 = time elapsed from contact to F1; T2 = time elapsed from contact to F2; TBW = time from feet contact until vertical ground reaction forces reach the subject´s weight for the first time after the landing
* = P < 0.05
Acknowledgments
This study was partially supported by the European Social Fund and by the Council of Education of the Junta de Comunidades de Castilla-La Mancha, Spain.
Biographies

Javier Abián-Vicén
Employment
Research Fellow, Faculty of Sports Sciences, University of Castilla-La Mancha, Spain.
Degree
MSc
Research interests
Biomechanics, ankle taping, risk of knee injury in landings.
E-mail: Javier.abian@uclm.es

Luis M. Alegre
Employment
Assistant Professor, Faculty of Sports Sciences, University of Castilla-La Mancha, Spain.
Degree
PhD
Research interests
Biomechanics, muscle mechanics.
E-mail: luis.alegre@uclm.es

J. Manuel Fernández-Rodríguez
Employment
Physical Therapist, Associate Professor.
School of Physiotherapy and Nursery, University of Castilla-La Mancha., Spain.
Degree
Pt
Research interests
Prophylactic taping, rehabilitation.
E-mail: ultralauf@ischulze.de
Amador J. Lara
Employment
Research Fellow, Faculty of Sports Sciences, University of Castilla-La Mancha, Spain.
Degree
MSc
Research interests
Biomechanics, strength training.
E-mail: Amador.lara@uclm.es

Marta Meana
Employment
Associate Professor, Department of Physical Activity and Sports, Catholic University San Antonio, Murcia, Spain.
Degree
PhD
Research interests
Biomechanics, ankle taping, training performance.
E-mail: mmeanariera@gmail.com
Xavier Aguado
Employment
Professor, Faculty of Sports Sciences, University of Castilla-La Mancha, Spain.
Degree
PhD
Research interests
Biomechanics, ankle taping, injury prevention, muscle mechanics.
E-mail: xavier.aguado@uclm.es
References
- Bennell K.L., Goldie P.A. (1994) The differential effects of exter-nal ankle support on postural control. Journal of Orthopaedic and Sports Physical Therapy 220, 287-295 [DOI] [PubMed] [Google Scholar]
- Bosco C., Colli R., Intoini E., Cardinale M., Tsarpela O., Maella A., Tihanyi J., Viru A. (1999) Adaptive responses of human skeletal muscle to vibration exposure. Clinical Physiology 19, 183-187 [DOI] [PubMed] [Google Scholar]
- Burks R.T., Bean B.G., Marcus R., Barker H.B. (1991) Analysis of athletic performance with prophylactic ankle devices. American Journal of Sports Medicine 119, 104-106 [DOI] [PubMed] [Google Scholar]
- Carter J.E. (1982) Anthropometric instruments and measurements used in the Montreal Olympic Games anthropological project. Physical structure of olympics athletes. Part I: MOGAP. Carter J.E.L., Karger Basel.Medicine and Sport Science; 16, 150-155 [Google Scholar]
- Cordova M.L., Ingersoll C.D., Palmieri R.M. (2002) Efficacy of prophylactic ankle support: an experimental perspective. National Athletic Trainers 37, 446-457 [PMC free article] [PubMed] [Google Scholar]
- Dufek J.S., Bates B.T. (1991) Biomechanical factors associated with injury during landing in jump sports. Sports Medicine 12, 326-337 [DOI] [PubMed] [Google Scholar]
- Feuerbach W., Grabiner M.D. (1993) Effect of the aircast on unilateral postural control: amplitude and frequency variables. Journal of Orthopaedic and Sports Physical Therapy 77, 149-154 [DOI] [PubMed] [Google Scholar]
- Garrick J.G., Requa R.K. (1988) The epidemiology of foot and ankle injuries in sports. Clinics in Sports Medicine 7, 29-36 [PubMed] [Google Scholar]
- Greene T.A., Hillman S.K. (1990) Comparison of support provided by a semirigid orthosis and adhesive ankle taping before, during, and after exercise. American Journal of Sports Medicine 18, 498-506 [DOI] [PubMed] [Google Scholar]
- Gross M.T., Lapp A.K., Davis M. (1991) Comparison of Swede-o-universal ankle support and aircast sport-stirrup orthoses and ankle tape in restricting eversion-inversion before and after exercise. Journal of Orthopaedic and Sports Physical Therapy 13, 11-19 [Google Scholar]
- Hertel J.N., Guskiewicz K.M., Kahler D.M., Perrin D.H. (1996) Effect of lateral ankle joint anesthesia on center of balance, postural sway, and joint position sense. Journal of Sport Rehabilitation 5, 111-119 [Google Scholar]
- Hewett T.E., Myer G.D., Ford K.R., Heidt R.S., Colosimo A.J., Mclean S.G., van den Bogert A.J., Paterno M.V., Succop P. (2005) Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes. American Journal of Sports Medicine 33, 492-501 [DOI] [PubMed] [Google Scholar]
- Hopkins W.G. (2000) Measures of reliability in sports medicine and science. Sports medicine 30, 1-15 [DOI] [PubMed] [Google Scholar]
- Hopper D.M., McNair P., Elliott C. (1999) Landing in netball: effects of taping and bracing the ankle. British Journal of Sports Medicine 33, 409-413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hume P.A., Gerrard D.F. (1998) Effectiveness of external ankle support. Sports Medicine 25, 285-312 [DOI] [PubMed] [Google Scholar]
- Jones D., Louw Q., Grimmer K. (2000) Recreational and sporting injury to the adolescent knee and ankle: prevalence and causes. Australian Journal of Physiotherapy 46, 179-188 [DOI] [PubMed] [Google Scholar]
- Kinzey S.J., Ingersoll C.K., Knight K.L. (1997) The effects of selected ankle appliances on postural control. Journal of Athletic Training 32, 300-303 [PMC free article] [PubMed] [Google Scholar]
- Leaf J.R., Keating J.L., Kolt G.S. (2003) Injury in the Australian sport of callisthenics: a prospective study. Australian Journal of Physiotherapy 49, 123-130 [DOI] [PubMed] [Google Scholar]
- Louw Q., Grimmer K., Vaughan C.L. (2006) Biomechanical outcomes of a knee neuromuscular exercise programme among adolescent basketball players: a pilot study. Physical Therapy in Sport 7, 65-73 [Google Scholar]
- Mackean L.C., Bell G., Burnham R.S. (1995) Prophylactic ankle bracing vs taping: effects on functional performance in female basketball players. Journal of Orthopaedic and Sports Physical Therapy 22, 77-81 [DOI] [PubMed] [Google Scholar]
- Macpherson K., Sitler M., Kimura I., Horodyski M. (1995) Effects of a semirigid and softshell prophylactic ankle stabilizer on selected performance tests among high school football players. Journal of Orthopaedic and Sports Physical Therapy 21, 147-152 [DOI] [PubMed] [Google Scholar]
- McCaw S.T., Cerullo J.F. (1999) Prophylactic ankle stabilizers affect ankle joint kinematics during drop landings. Medicine and Science in Sports and Exercise 31, 702-707 [DOI] [PubMed] [Google Scholar]
- Osborne M.D., Rizzo T.D. (2003) Prevention and treatment of ankle sprain in athletes. Sports Medicine 33, 1145-1150 [DOI] [PubMed] [Google Scholar]
- Özgüven H., Berme N. (1988) An experimental and analytical study of impact forces during human jumping. Journal of Biomechanics 21, 1061-1066 [DOI] [PubMed] [Google Scholar]
- Paris D.L. (1992) The effects of the Swede-o, new cross, and McDavid ankle braces and adhesive ankle taping on speed, balance, agility and vertical jump. Journal of Athletic Training 27, 253-255 [PMC free article] [PubMed] [Google Scholar]
- Riemann B.L.S, hmitz R.J.G, le M.G.M, Caw S.T. (2002) Effect of ankle taping and bracing on vertical ground reaction forces during drop landings before and after treadmill jogging. Journal of Orthopaedic and Sports Physical Therapy 32, 628-635 [DOI] [PubMed] [Google Scholar]
- Robbins S., Waked E. (1998) Factors associated with ankle injuries. Sports Medicine 25, 63-72 [DOI] [PubMed] [Google Scholar]
- Thacker S., Stroup D., Branche C., Gilchrist J., Goodman R., Weitman E. (1999) The prevention of ankle sprains in sports. American Journal of Sports Medicine 27, 753-760 [DOI] [PubMed] [Google Scholar]
- Verbrugge J.D. (1996) The effects of semirigid air-stirrup bracing vs adhesive ankle taping on motor performance. Journal of Orthopaedic and Sports Physical Therapy 223, 320-325 [DOI] [PubMed] [Google Scholar]
- Wilkerson G.B. (1991) Comparative biomechanical effects of the standard method of ankle taping and a taping method designed to enhance subtalar stability. American Journal of Sports Medicine 19, 588-595 [DOI] [PubMed] [Google Scholar]