

Abstract
Objective:
The study aimed to develop a national reference on birth weight-specific neonatal survival in the State of Qatar to facilitate parental counseling.
Study Design:
This was a retrospective, analytic, and comparative study.
Materials and Methods:
The birth weight-specific neonatal mortality data for the years 2003 and 2010, collected from the admission and discharge registers of the neonatal intensive care unit, were stratified using the stratifications given in Vermont Oxford Network (VON) 2007 annual report. Category-wise birth weight-specific mortality and relative risk (RR) of death were compared between Qatar data (2003 and 2010) and VON 2007 report.
Results:
Qatar's neonatal mortality rate (NMR) dropped from 5 of 1000 in 2003 to 4.4 of 1000 in 2010 (P=0.443) which was significant for birth weight categories 501–750 g and 751–1000 g (P=0.026 and P=0.05, respectively). Qatar's NMR in 2010 was significantly lower than VON's NMR during 2007 (P<0.001) though VON's NMR was significantly lower among birth weight categories 751–1000 g and 1001–1500 g (P=0.001 and P=0.003, respectively). The RR of mortality decreased with increasing birth weight. The decline was very sharp for birth weight categories between 500 and 1500g. The RR was 25 times higher in babies with birth weight less than 750 g as compared to babies with birth weight ≥ 2550 g, both in Qatar and VON data. For birth weight categories 751–1000 g and 1001–1500 g, the RR was twice in Qatar as compared to the VON report (16.8 versus 7.8, and 5.5 versus 2.7, respectively).
Conclusions:
Qatar's current overall and birth weight-specific NMRs are comparable with the VON report except in birth weight categories 751–1000 g and 1001–1500 g which were higher in Qatar. This needs further in-depth qualitative analysis.
Keywords: Birth weight, neonatal mortality, Qatar
INTRODUCTION
The association between birth weight and mortality is the strongest in epidemiology.[1] Babies weighing less than 1500 g have a mortality risk at least 100-fold higher than those with an optimal weight (the weight associated with the lowest mortality).[1] Worldwide neonatal survival has improved significantly over the last four decades,[2,3] particularly so in the developed countries which have witnessed an increasing survival of extremely low-birth-weight babies during this period.[4,5,6,7,8] Our recent publications,[9,10,11] as well as other international publications,[2,3] have confirmed that State of Qatar's current neonatal survival rates and short-term morbidities are comparable with most developed world countries. However, birth weight-specific neonatal mortality has never been reported from Qatar. The increasing survival of extremely low birth weight babies brings a new challenge to the practicing neonatologists who are faced, almost on a daily basis, with the parental question of “what are the chances of my baby's survival?” An up-to-date knowledge of the unit-based birth weight-specific mortality as well as its comparative study with the international benchmarks provides a handy reference for both the parents and the neonatologist. We conducted our current study to fill this gap in knowledge.
MATERIALS AND METHODS
This retrospective analytic study was conducted as a part of the background studies of Perinatal Neonatal Outcomes Research Study in the Arabian Gulf (PEARL Study) which is Qatar's prospective National Perinatal Epidemiologic Study funded by Qatar National Research Fund (grant no. QNRF-NPRP-09-390-3-097, IRB approval protocol no. 9211/09). PEARL Study, a joint collaborative research project between Hamad Medical Corporation (HMC), Doha, Qatar, and University of Gloucestershire, Gloucester, United Kingdom, was launched on January 1, 2011, with an aim to establish a National Neonatal Perinatal Registry for Qatar called Q-Peri-Reg.
The 2003 and 2010 birth weight-specific mortality data for the current study (IRB approval protocol no. 8208/08) were ascertained from the admission and discharge registers of neonatal intensive care unit (NICU) and Maternity Unit, Women's Hospital, HMC, which is the largest state-run maternity hospital in the country. The hospital is accredited by the United States Joint Commission International (JCI)for the standard and quality of health care it provides. More than 87% of State's term deliveries and 100% of <32-week gestation deliveries take place in this hospital. Therefore, for all practical purposes, the data from Women's Hospital represent Qatar's national data, particularly for babies delivered with <32 weeks gestation and with <1500 g birth weight. Women's Hospital hosts Qatar's only tertiary care neonatal unit which has a total of 80 neonatal cots including 37 intensive care cots. All high-risk and very sick babies born in the State are admitted to this unit.
We used the Vermont Oxford Network (VON)[12] low birth weight and expanded database report of 2007 as an international benchmark for all comparative purposes. Following the pattern in the VON report, we categorized babies with birth weight <1000 g into 250 g categories and babies with birth weight >1000 g into 500 g categories. Because of their dismal outcome, babies with birth weight <500 g were excluded from the study. The mortality in each birth weight category was calculated as the percentage of total live births in the same category. Babies declared nonviable in the delivery room, any possible home deaths, very late neonatal deaths (>28 days of corrected postnatal age), and babies dying after discharge from the hospital were not included in the study because their number was very small and statistically insignificant. To make the comparisons even, the delivery room deaths in the VON 2007 report were also excluded during the calculation of birth weight-specific mortality rates.
Statistical analysis
Data were entered and analyzed in Epi Info, version 3.5.1 (2008). Frequency with percentage was calculated for neonatal mortality across different birth weight categories from Qatar during 2003 and 2010 and the VON 2007 report. We compared the neonatal mortality in each birth weight category in Qatar during 2003 with that during 2010, and that in Qatar during 2010 with the VON 2007 report. The risk ratio (RR) with 95% confidence intervals and two-tailed P-value based on chi square test were calculated to determine the significant difference at a level of 5%. In order to determine trends in neonatal mortality across different birth weight categories in Qatar during 2010 and VON 2007 data, we calculated the RR between each birth weight category and normal birth weight (≥2500 g).
RESULTS
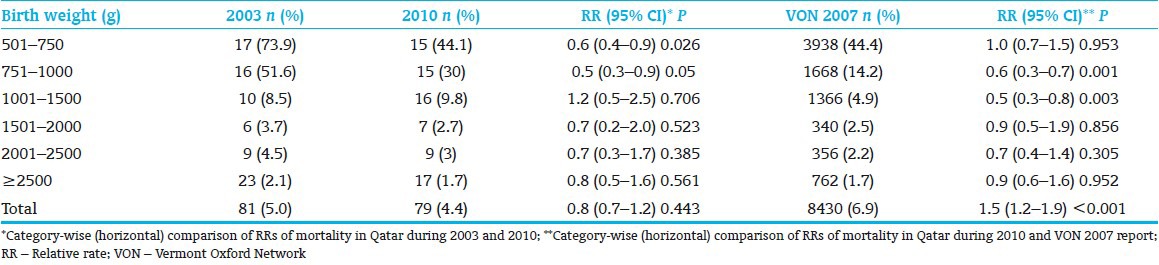
Qatar's Neonatal Mortality Rate (NMR) dropped from 5 per 1000 in 2003 to 4.4 per 1000 in 2010 with a 20% decrease in the RR of death (RR 0.8; 95% CI 0.7–1.2; P=0.443; Table 1). Qatar's NMR during 2010 was significantly lower than VON report's NMR during 2007 with 1.5 times less RR of death in Qatar (RR 1.5; 95% CI 1.2–1.9; P<0.001). Between 2003 and 2010, Qatar's birth weight-specific mortality improved significantly only in birth weight categories 501–750 g and 751–1000 g (P=0.026 and P=0.05, respectively). There was no difference in birth weight-specific NMRs between Qatar 2010 and VON 2007 data except for birth weight categories 751–1000 g and 1001–1500 g in which VON report's mortality rate was significantly better (P=0.001 and P=0.003, respectively).
Table 1.
Comparison of birth weight-specific mortality in Qatar during 2003 and 2010 and VON report during 2007
The RR of mortality decreased with increasing birth weight both in Qatar and VON data [Table 2]. The decline was very sharp for birth weight categories between 500 and 1500 g. As compared to babies with birth weight ≥2500 g, the RR of mortality was 25 times, 17 times, and 5.5 times higher (P<0.001) in babies with birth weight 500–750 g, 751–1000 g, and 1001–1500 g, respectively, in Qatar during 2010. In babies with birth weight >1500 g, the RR was 1.5 times higher which is statistically significant (P<0.001) in VON but not in Qatar's data. For birth weight categories 751–1000 g and 1001–1500 g, the RR of mortality was twice in Qatar as compared to VON (16.8 versus 7.8 and 5.5 versus 2.7 respectively) which has produced a spindle-shaped gap between the RR curves of Qatar 2010 data and VON 2007 data at these birth weight points [Figure 1]. Qatar's 2010 RR curve is also significantly shifted to the right as compared to Qatar's 2003 RR curve at these birth weight points.
Table 2.
The RR of mortality for each birth weight category as compared with normal birth weight (≥2500 g) category: Qatar (2010) and VON (2007) data
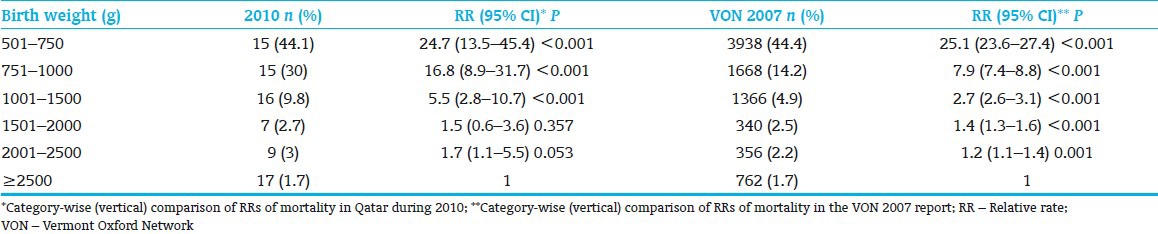
Figure 1.
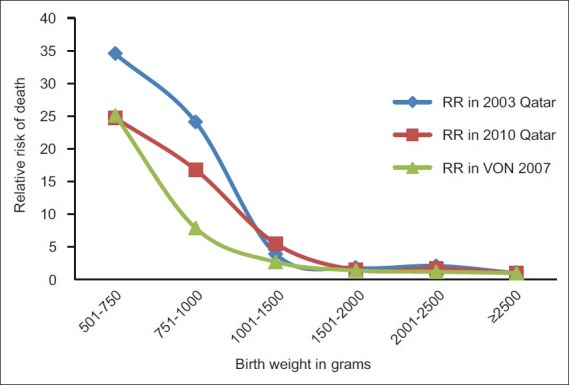
Trends in the gestational age-specific relative risk of neonatal mortality in Qatar during 2003 and 2010 and VON during 2007 (reference group babies with birth weight ≥2500 g)
DISCUSSION
Birth weight is a very strong indicator of an individual baby's intact survival.[13] Although birth weight alone may not be the cause of mortality, the association is robust.[1] Babies with a low birth weight are at higher risk of a poor perinatal outcome and long-term cognitive and motor impairments.[13,14] The proportion of babies with birth weight under 2500 g is a widely used indicator for assessing the population at risk, and historical series exist for many countries.[14] Our study has generated the most updated birth weight category-wise neonatal survival profile for Qatar [Table 1] which has demonstrated that the outcomes are not much different from the developed countries.
Among the low birth weight babies, those with birth weight under 1500 g are at the highest risk of mortality and morbidity.[14] Our study has confirmed the same pattern of risk of mortality. The relative risk of mortality decreased sharply (P<0.001) while moving from a birth weight of 500 g to 1500 g [Table 2 and Figure 1]. The same was the pattern in the 2007 report of VON which is a database of more than 800 NICUs worldwide, most of these being in North America and Europe.[12]
Babies may have a low birth weight either because of preterm birth or intrauterine growth restriction (IUGR) or for both these reasons. As Allen Wilcox[13] has stated, not all premature babies are small and not all small babies are premature. Both low birth weight due to preterm birth and IUGR are a major cause of adverse perinatal outcomes and later impairments in life.[14] Mortality and morbidity are increased among infants born at term whose birth weights are at or below the third percentile for their gestational age.[15] Our study included both groups of low birth weight babies, preterm as well as IUGR. The PEARL Study has recently reported on the incidence of low birth weight and IUGR in Qatar.[16] The study has shown that the incidence of low birth weight in Qatar is independent of parental ethnicity. However, the incidence of IUGR is significantly higher in the non-Qatari population as compared to the Qatari population.[16] Therefore, a new study which shall independently determine the short- and long-term mortality and morbidity outcomes of low birth weight due to preterm birth and low birth weight due to IUGR is indicated. The PEARL Study is currently ascertaining these data prospectively from the State of Qatar and will probably be able to get them published by early next year.
According to our study, Qatar's NMR dropped steadily from 5 per 1000 in 2003 to 4.4 per 1000 in 2010 which was statistically not significant (P=0.443). In another of our recent article under publication,[17] we have shown that Qatar's NMR had become almost static between 2008 and 2010. The same phenomenon was observed by the developed countries during 1990's. By 1990, virtually all NICUs had survival rates of ≥90% for infants with birth weight ≥1000 g.[5,6,7,8,18,19] From 1991 to 1997, the overall Extremely Low Birth Weight (ELBW) survival increased steadily at an approximate rate of 4% per year. However, from 1997 to 2001, there was no significant improvement in the survival of ELBW infants except those with birth weight between 500 and700 g.[19] Having achieved an NMR comparable to that in many developed countries,[3,9,10,17] Qatar is now passing through the stage of achieving survival at the limits of viability. The same pattern has recently been reported from Sharjah.[20] There is a need to report similar data from Other regional countries particularly those constituting Gulf Cooperation Council (GCC) countries, which, like Qatar, have passed through very rapid socioeconomic, educational, and health care development over the last three decades.
SUMMARY
Qatar's current overall NMR, birth weight-specific NMR, and relative risk (RR) of death are comparable to most developed countries. Like most developed countries, the RR of mortality in Qatar increased sharply when the birth weight was ≤1500 g. Future studies to independently determine the outcome of low birth weight due to preterm birth and low birth weight due to IUGR are highly indicated.
ACKNOWLEDGMENT
We are thankful to Mohammad Tahir Yousafzai, statistician, PEARL study, for his support in data analysis and synthesis of tables and graphs. Perinatal Neonatal Outcomes Research Study in the Arabian Gulf (PEARL Study) is a 3-year prospective joint collaborative research project of Hamad Medical Corporation, Doha, Qatar, and University of Gloucestershire, United Kingdom, which has been exclusively funded by the Qatar National Research Fund (QNRF) through grant no. QNRF-NPRP-09-390-3-097. QNRF (www.qnrf.org) is the research funding body of Qatar Foundation (www.qf.org.qa).
Footnotes
Source of Support: Qatar National Research Fund (grant no. QNRFNPRP-09-390-3-097)
Conflict of Interest: None declared.
REFERENCES
- 1.Basso O, Wilcox AJ, Weinberg CR. Birth weight and mortality: Causality or confounding? Am J Epidemiol. 2006;164:303–11. doi: 10.1093/aje/kwj237. [DOI] [PubMed] [Google Scholar]
- 2.Rajaratnam JK, Marcus JR, Flaxman AD. Neonatal, Post neonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: A systematic analysis of progress towards Millennium Development Goal 4. Lancet. 2010;375:1988–2008. doi: 10.1016/S0140-6736(10)60703-9. [DOI] [PubMed] [Google Scholar]
- 3.World Health Statistics 2010. World Health Organisation. [Last accessed on 6th July 2011]. Available from: http://www.who.int/gho .
- 4.Haig D. Meditations on birth weight: Is it better to reduce the variance or increase the mean? Epidemiology. 2003;14:490–2. doi: 10.1097/01.EDE.0000070402.42917.f4. Erratum: Epidemiology 2003;14:632. [DOI] [PubMed] [Google Scholar]
- 5.O’shea TM, Klinepeter KL, Goldstein DJ, Jackson BW, Dillard RG. Survival and developmental disability in infants with birth weights of 501 to 800 g, born between 1979 and 1994. Pediatrics. 1997;100:982–6. doi: 10.1542/peds.100.6.982. [DOI] [PubMed] [Google Scholar]
- 6.Allen MC, Donohue PK, Dusman AE. The limit of viability: Neonatal outcome of infants born at 22 to 25 weeks’ gestation. N Engl J Med. 1993;329:1597–601. doi: 10.1056/NEJM199311253292201. [DOI] [PubMed] [Google Scholar]
- 7.Hack M, Fanaroff A. Outcomes of extremely immature infants: A perinatal dilemma. N Engl J Med. 1993;329:1649–50. doi: 10.1056/NEJM199311253292210. [DOI] [PubMed] [Google Scholar]
- 8.Hack M, Friedman H, Fanaroff A. Outcomes of extremely low birth weight infants. Pediatrics. 1996;98:931–7. [PubMed] [Google Scholar]
- 9.Salameh K, Rahman S, Al Rifai H, Masoud A, Lutfi S, Abdouh G, et al. An analytic study of trends in perinatal and neonatal mortality rates in the state of Qatar over a 30 years period (1977-2007): A comparative study with regional and developed countries. J Perinatol. 2009;29:765–70. doi: 10.1038/jp.2009.89. [DOI] [PubMed] [Google Scholar]
- 10.Rahman S, Salameh K, Bener A, El Ansari W. Socioeconomic associations of improved maternal, neonatal, and perinatal survival in Qatar. Int J Womens Health. 2010;2:311–8. doi: 10.2147/IJWH.S12426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Parappil H, Rahman S, Salama H, Al Rifai H, Parambil NK, El Ansari W. Outcomes of 28+1 to 32+0 weeks gestation babies in the state of Qatar: Finding facility-based cost effective options for improving the survival of preterm neonates in low income countries. Int J Environ Res Public Health. 2010;7:2526–42. doi: 10.3390/ijerph7062526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Vermont Oxford Network. 2007 Database summaries. [Last accessed on 10th July 2011]. Available from: http://www.vtoxford.org .
- 13.Wilcox AJ. On the importance– and the unimportance–of birthweight. Int J Epidemiol. 2001;30:1233–41. doi: 10.1093/ije/30.6.1233. [DOI] [PubMed] [Google Scholar]
- 14.Europeristat Project. Perinatal Health Report. 2008. [Last accessed on 10th July 2011]. Available from: http://www.europeristat.com .
- 15.McIntire DD, Bloom SL, Casey BM, Leveno KJ. Birth weight in relation to morbidity and mortality among newborn infants. N Engl J Med. 1999;340:124–8. doi: 10.1056/NEJM199904223401603. [DOI] [PubMed] [Google Scholar]
- 16.Abdulkader ZM, Rahman S, Nimeri N. Incidence of low birth weight and intrauterine growth restriction across various ethnicities in the state of Qatar – A PEARL study analysis. Qatar Med J. doi: 10.5339/qmj.2012.2.10. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rahman S, El Ansari W, Bener A, Salameh K, Al Nimeri N, El Tinay S, et al. Have neonatal mortality rates in Qatar become static? A PEARL study analysis. East Mediterr Health J. In press. [PubMed] [Google Scholar]
- 18.Hack M, Horbar JD, Malloy MH, Tyson JE, Wright E, Wright L. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Network. Pediatrics. 1991;87:587–96. [PubMed] [Google Scholar]
- 19.Meadow W, Lee G, Lin K, Lantos J. Changes in mortality for extremely low birth weight infants in the 1990s: Implications for treatment decisions and resource use. Pediatrics. 2004;113:1223–9. doi: 10.1542/peds.113.5.1223. [DOI] [PubMed] [Google Scholar]
- 20.Yaseen H, Yaseen H. Survival of extremely premature infants at the largest moh referral hospital in UAE: Comparable results to developed countries. J Pediatr Sci. 2010;2:e18. [Google Scholar]