

Abstract
Background:
Assault, though a major cause of maxillofacial injuries in the developed nations, has not been adequately investigated among Nigerian population. This study aimed to analyze the pattern of maxillofacial injuries caused by assault in our institution.
Methods:
A descriptive clinical survey of patients with assault-induced oral and maxillofacial injuries presenting to our maxillofacial surgery clinic/emergency ward was carried out. Demographic data and pattern of injuries obtained from patients’ record and department trauma database were analyzed.
Results:
156 patients presented with oral and maxillofacial injuries between October 2009 and December 2010. Thirty-four cases were due to assault and male to female ratio was 1.8:1. The mean age of the patients was 21.4±6.26 years (age range 2–48 years). 23.6% (n=8) of the injuries were due to domestic violence between spouses while 35.3% (n=12) resulted from fight. Students unrest and armed robbery attack accounted for six cases each (17.7%, n=6), while there were two cases due to child battering. 64.3% (n=22) of the injuries sustained involved soft tissues while 35.7% involved hard tissues. Contusion was the most common isolated soft tissue injury accounting for 56% (n=10) while dentoalveolar fracture was the most encountered hard tissue injury (62.5%, n=16).
Conclusion:
There is need for preventive strategies to reduce the incidence of assault-induced maxillofacial injuries.
KEYWORDS: Assault, oral and maxillofacial injuries, pattern
INTRODUCTION
The etiology of maxillofacial injuries varies from one country to another and even within the same country depending on the prevailing socioeconomic, cultural, and environmental factors.[1–4] Road traffic crashes (RTC), assaults, sports, falls occupational hazards are documented causes of oral and maxillofacial injuries.[1,4–8] Animal attack is another cause of facial injuries that has been reported in the northern part of Nigeria.[9] Being the most exposed part of the human body, the maxillofacial region is vulnerable to varying degree of injuries when the individual is subjected to physical trauma.[2,5] Skeletal and soft tissue injuries of the face constitute quite a significant portion of the workload of the oral and maxillofacial surgeons in Nigeria.[4–7] Therefore, Periodic verification of the etiology of maxillofacial injuries helps to recommend ways in which maxillofacial injuries can be averted.[1]
In the past, road traffic crashes (RTC) used to be the most common cause of facial fractures globally.[8–11] The trend is different in the developed countries where assault appeared to have overtaken RTC as the leading cause of oral and maxillofacial injuries.[12–14] However, RTC still remain the leading cause of maxillofacial injuries in developing countries, Nigeria inclusive.[15–19] Other causes of oral and maxillofacial injuries have received little attention in the Nigerian literature probably because of the predominance of RTC in the etiology of such injuries.
Assault-induced maxillofacial injuries have been under-reported in the literature despite increase in cases of altercations worldwide[20] and available reports were mostly from foreign literature.[21,22] One of the few reports on assault related maxillofacial injuries is the study done by Olasoji et al.[20] on prevalence of assault-induced oral and maxillofacial injuries in North-eastern part of Nigeria. He attributed the increasing wave of assault-induced maxillofacial injuries to the nomadic life style of the people of the region. The present study was conceived because of dearth of studies on assault related maxillofacial injuries among Nigerian population. The aim of the study was to determine the prevalence and pattern of assault-induced oral and maxillofacial injuries in our institution.
METHODOLOGY
The study was carried out by recruiting patients who presented at the Accident and emergency ward and maxillofacial surgery clinic of the University Teaching Hospital, Ado-Ekiti. The hospital is a major referral center covering Ekiti and adjoining Ondo and Kogi state in south-western Nigeria. It is a descriptive clinical study including oral and maxillofacial assault cases that presented between October 2009 and December 2010. Inclusion criteria include history of assault and confirmation of maxillofacial injury on examination and investigation. Ethical approval was obtained from our institution's ethics committee.
Age, sex, mechanism of assault, and examination findings concerning injury pattern were documented. Radiological investigation was also carried out where necessary. All patients received treatments based on the diagnosis. Patients who had soft tissue abrasions and contusions were treated conservatively.
Data obtained on the prevalence, Pattern of injuries and assault mechanism were summarized in tables and figures. Descriptive analysis of data was done with Statistical Package for Social Sciences (SPSS) version 17.
RESULTS
Of the 156 cases of oral and maxillofacial injuries seen between October 2009 and December 2010, 34 cases were due to assault. There were 22 males and 12 females (ratio 1.8:1). The mean age of the patients was 21.4±6.26 years (age range 2–48 years) and more than 50% of the patients were between 21 and 30 years of age [Figure 1].
Figure 1.

Showed the age distribution of assaulted patients in this series. It can be deduced that most victims of assault induced facial injuries are between 20 to 30 years of age
Causes of assault-induced maxillofacial injuries in our series include domestic violence, interpersonal altercation (fight), child battering, students’ unrest, and armed robbery attack. Figure 2 shows the distribution of assault cases by etiology. Interpersonal altercation (fight) accounted for 35.3% of the injuries while 23.6% of the injuries were due to domestic violence between spouses. Students unrest and armed robbery attack accounted for six cases each (17.7%, n=6), while there were two cases due to child battering. It is worthy to note that the assaulted victims of domestic violence were all females and the most common means of assault is the fist. There is higher male preponderance in other injury types [Table 1]. Apart from the fist, weapons such as broken bottles (n=3), knife (n=5), machete (n=4), and pipes (n=2) were used for assault. None of the patients in this study had gunshot injury.
Figure 2.
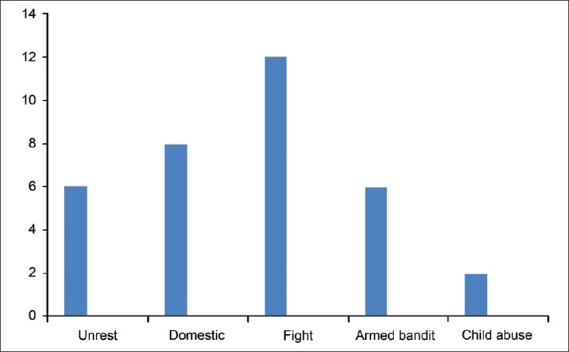
Showed the causes of oral and maxillofacial injuries in the patients studied. The figure revealed that fight accounted for more cases of injuries (n=12) followed by domestic violence (n=8). Other causes of injuries are armed robbery attack (n=6), students’ unrest (n=6) and child abuse (n=2)
Table 1.
Pattern of injury

Injury pattern revealed that 64.3% (n=22) of the injuries sustained involved soft tissues while 35.7% involved hard tissues. Contusion was the most common isolated soft tissue injury accounting for 56% (n=10) of such injuries while dentoalveolar fracture was the most encountered hard tissue injury (62.5%, n=16). There were two cases each of mandibular and nasal bone fractures [Table 2].
Table 2.
Etiology and pattern of injury

All patients received initial treatments aimed at control of hemorrhage and prevention of infection by antibiotic medication. Soft tissue lacerations were carefully sutured after wound debridement while contusions were treated conservatively. Nasal fractures were reduced with Walsham's nasal forceps, dentoalveolar fractures were treated by splinting the segments with 0.5 mm soft stainless steel wire while mandibular fractures were immobilized with 2.0 mm titanium locking plates. All patients were treated under local anesthesia except the mandibular fractures where patients had to be intubated for general anesthesia.
DISCUSSION
Although RTC remain the leading cause of oral and maxillofacial injuries in most developing countries, other causes such as assaults, industrial accident, and sport-related injuries have increased over time.[22–27] The situation is different in the developed nations where assaults and interpersonal altercations are the leading cause of oral and maxillofacial injuries.[28]
The prevalence of assault in our study was 21.8% this is comparable to previous studies where assault cases constituted less than 20%. On the contrary, Olasoji et al.,[4] reported a prevalence of 57.1% from the north eastern part of the country. He attributed this to the nomadic lifestyle of the people in the region where animals are moved over several kilometers of land grazing over farms and destroying cash crops in the process, this frequently leads to fight between farmers and cattlemen.
Peak age incidence of 21–30 years found in our study is in agreement with the literature probably because people in this age group are in the active phase of livelihood and are likely to be involved in assaults more than other age groups. Also, we found a higher male preponderance in agreement with other studies; however those involved in domestic violence in this study were all female victims of assault by the spouse. Poor socioeconomic condition and stress from unemployment could lead to aggressive tendencies by men and this often leads to assault on wives. The influence of alcohol consumption on domestic violence has also been reported in the literature,[22,29] though we could not establish such in this study. Some of the patients in our series were victims of politically motivated violence and students’ unrest. Similarly, quite a number of maxillofacial injuries are seen during cult clashes in higher institutions. This is unlike European and American studies where most of the fights occurred in the street, club or pub.[1,28]
Contusion was the most common soft tissue injury in our series. This may be explained by the fact that fist was the commonest means of assault, and it causes subcutaneous tissue injury while preserving the continuity of the overlying skin. Most authors also reported contusion as the most common soft tissue injury to the maxillofacial region.[30] Facial lacerations were caused by sharp objects such as knife and machete. Dentoalveolar fracture constituted 62.5% of hard tissue injuries in our study. This finding may be due to the fact that assaults are less likely to cause mandibular ormid-facial fractures which are more commonly related to road traffic crashes. Moreover, dentoalveolar injuries related to RTC and other causes are under-reported in most maxillofacial injury surveys. However, Gassner andco-workers[23] in a large survey of maxillofacial injuries involving 9543 patients reported an incidence of 49.9% of dentoalveolar injuries. Similar findings were reported in studies where dental oral tissues were included.[26] In conclusion, assault-induced oral and maxillofacial injuries constitute a significant workload of maxillofacial surgeons and as such prevention strategies should be embarked on. Increasing unemployment rate and the poor per capital income of an average Nigerian which has decreased by more than 75% during the past 25 years are contributory to violent conduct. Assault-induced oral and maxillofacial injuries can be curbed if unemployment is tackled and education of youth is adequately addressed.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Adeyemo WL, Ladeinde AL, Ogunlewe MO, James O. Trends and characteristics of oral and maxillofacial injuries in Nigeria: A review of the literature. Head Face Med. 2005:1–7. doi: 10.1186/1746-160X-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ugboko VI, Odusanya SA, Fagade OO. Maxillofacial fractures in a semi-urban Nigerian teaching hospital. A review of 442 cases. Int J Oral Maxillofac Surg. 1998;27:286–9. doi: 10.1016/s0901-5027(05)80616-2. [DOI] [PubMed] [Google Scholar]
- 3.Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern Nigeria. Br J Oral Maxillofac Surg. 2002;40:140–3. doi: 10.1054/bjom.2001.0716. [DOI] [PubMed] [Google Scholar]
- 4.Oji C. Maxillofacial injuries. Plast Reconstr Surg. 1996;97:866–8. doi: 10.1097/00006534-199604000-00035. [DOI] [PubMed] [Google Scholar]
- 5.Fasola AO, Nyako EA, Obiechina AE, Arotiba JT. Trends in the characteristics of maxillofacial fractures in Nigeria. J Oral Maxillofac Surg. 2003;61:1140–3. doi: 10.1016/s0278-2391(03)00671-2. [DOI] [PubMed] [Google Scholar]
- 6.Fasola AO, Obiechina AE, Arotiba JT. An audit of midfacial fractures in Ibadan, Nigeria. Afr J Med Med Sci. 2001;30:183–6. [PubMed] [Google Scholar]
- 7.Ajagbe HA, Daramola JO, Oluwasanmi JO. Civilian-type facial injuries. A retrospective study of cases seen at the university college hospital, Ibadan. Niger Med J. 1977;7:432–6. [Google Scholar]
- 8.Sastry SM, Sastry CM, Paul BK, Bain L, Champion HR. Leading causes of facial trauma in the major trauma outcome study. Plast Reconstr Surg. 1995;95:196–7. doi: 10.1097/00006534-199501000-00039. [DOI] [PubMed] [Google Scholar]
- 9.Ugboko VI, Olasoji HO, Ajike SO, Amole AOD, Ogundipe OT. Facial injuries caused by animals in Northern Nigeria. Br J Oral Maxillofac Surg. 2002;40:433–7. [PubMed] [Google Scholar]
- 10.Khan AA. A retrospective study of injuries to the maxillofacial skeleton in Harare, Zimbabwe. Br J Oral Maxillofac Surg. 1988;26:435–9. doi: 10.1016/0266-4356(88)90098-8. [DOI] [PubMed] [Google Scholar]
- 11.Magennis P, Shepherd J, Hutchison I, Brown A. Trends in facial injury. BMJ. 1998;316:325–6. doi: 10.1136/bmj.316.7128.325a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Adi M, Ogden GR, Chisholm DM. An analysis of mandibular fractures in Dundee, Scotland (1977 to 1985) Br J Oral Maxillofac Surg. 1990;28:194–9. doi: 10.1016/0266-4356(90)90088-3. [DOI] [PubMed] [Google Scholar]
- 13.Abiose BO. Maxillofacial skeleton injuries in the western states of Nigeria. Br J Oral Maxillofac Surg. 1986;24:31–9. doi: 10.1016/0266-4356(86)90037-9. [DOI] [PubMed] [Google Scholar]
- 14.van Hoof RF, Merkx CA, Stekelenbrg EC. The different patterns of fractures of the facial skeleton in four European countries. Int J Oral Surg. 1977;6:3–11. doi: 10.1016/s0300-9785(77)80066-5. [DOI] [PubMed] [Google Scholar]
- 15.Adekeye EO. The pattern of fractures of the facial skeleton in Kaduna, Nigeria. A survey of 1,447 cases. Oral Surg Oral Med Oral Pathol. 1980;6:491–5. doi: 10.1016/0030-4220(80)90068-7. [DOI] [PubMed] [Google Scholar]
- 16.Motamedi MH. An assessment of maxillofacial fractures: A 5-year study of 237 patients. J Oral Maxillofac Surg. 2003;61:61–4. doi: 10.1053/joms.2003.50049. [DOI] [PubMed] [Google Scholar]
- 17.Cheema SA, Amin F. Incidence and causes of maxillofacial skeletal injuries at mayo hospital in Lahore, Pakistan. Br J Oral Maxillofac Surg. 2006;44:232–4. doi: 10.1016/j.bjoms.2005.05.017. [DOI] [PubMed] [Google Scholar]
- 18.Khalil AF, Shaladi OA. Fractures of the facial bones in the eastern region of Libya. Br J Oral Surg. 1981;19:300–4. doi: 10.1016/0007-117x(81)90051-2. [DOI] [PubMed] [Google Scholar]
- 19.Adebayo ET, Ajike OS, Adekeye EO. Analysis of the pattern of maxillofacial fractures in Kaduna, Nigeria. Br J Oral Maxillofac Surg. 2003;41:396–400. doi: 10.1016/s0266-4356(03)00165-7. [DOI] [PubMed] [Google Scholar]
- 20.Olasoji HO. Maxillofacial injuries due to assault in Maiduguri, Nigeria. Trop Doct. 1999;29:106–8. doi: 10.1177/004947559902900216. [DOI] [PubMed] [Google Scholar]
- 21.Afzeilus LE, Rosen C. Facial fractures A review of 368 cases. In J Oral Surg. 1980;9:25–32. doi: 10.1016/s0300-9785(80)80003-2. [DOI] [PubMed] [Google Scholar]
- 22.McDade AM, McNicol RD, Ward-Booth P, Chesworth J, Moos KF. The aetiology of maxilla-facial injuries, with special reference to the abuse of alcohol. Int J Oral Surg. 1982;11:152–6. doi: 10.1016/s0300-9785(82)80002-1. [DOI] [PubMed] [Google Scholar]
- 23.Gassner R, Tuli T, Hachi O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: A 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg. 2003;31:51–61. doi: 10.1016/s1010-5182(02)00168-3. [DOI] [PubMed] [Google Scholar]
- 24.Arotiba GT. The aetiology of facial fractures in Lagos. Niger Postgrad Med J. 1996;3:37–42. [Google Scholar]
- 25.Kontio R, Suuronen R, Ponkkonen H, Lindqvist C, Laine P. Have the causes of maxillofacial fractures changed over the last 16 years in Finland. An epidemiological study of 725 fractures. Dent Traumatol. 2005;21:14–9. doi: 10.1111/j.1600-9657.2004.00262.x. [DOI] [PubMed] [Google Scholar]
- 26.Gassner R, Bosch R, Tuli T, Emshoff R. Prevalence of dental trauma in 6,000 patients with facial injuries: Implications for prevention. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87:27–33. doi: 10.1016/s1079-2104(99)70290-8. [DOI] [PubMed] [Google Scholar]
- 27.King RE, Scianna JM, Petruzelli GJ. Mandible fracture patterns: A suburban trauma center experience. Am J Otolaryngol. 2004;25:301–7. doi: 10.1016/j.amjoto.2004.03.001. [DOI] [PubMed] [Google Scholar]
- 28.Telfer MR, Jones GM, Shepherd JP. Trends in the aetiology of maxillofacial fractures in the United Kingdom (1977-1987) Br J Oral Maxillofac Surg. 1991;29:250–5. doi: 10.1016/0266-4356(91)90192-8. [DOI] [PubMed] [Google Scholar]
- 29.Le BT, Dierk EJ, Ueeck BA, Homer LD, Potter BF. Maxillofacial injuries associated with domestic violence. J Oral Maxillofac Surg. 2001;59:1277–83. doi: 10.1053/joms.2001.27490. discussion 1283-4. [DOI] [PubMed] [Google Scholar]
- 30.Fasola AO, Obiechina AE, Arotiba JT. Soft tissue injuries of the face: A 10 year review. Afr J Med Med Sci. 2000;29:59–62. [PubMed] [Google Scholar]