

Abstract
Aim/Objective:
To determine the pattern of morbidity and outcome among patients referred to the Pediatric Surgery Unit of the Lagos University Teaching Hospital (LUTH) following circumcision.
Materials and Methods:
Retrospective descriptive study of all patients with complications of circumcision who were managed in LUTH between 2008 and 2010.
Results:
There were 36 patients. The age range was between 2 days and 9 years (median-3 months). Fifteen cases (42.9%) were due to urethro-cutaneous fistula while there were six cases (16.7%) of postcircumcision bleeding. There were four cases (11.1%) each of partial penile amputation and buried penis. There were also cases of meatal stenosis, penile implantation cyst and glanulo-preputial skin bridge. With respect to the treatment offered, eleven (30.6%) patients had urethroplasty for the urethro-cutaneous fistulae while seven (19.4%) patients had penile refashioning for the buried penis and penile amputation. Appropriate surgical treatments were performed for the other complications.
Conclusion:
Urethrocutaneous fistula and penile amputation are the commonest complications of circumcision for which referral is made to LUTH. Treatment outcome was satisfactory. Health education and legislation to ensure procedure is performed by qualified medical and paramedical staff may reduce the morbidity.
KEYWORDS: Circumcision morbidity, indications, specialist care
INTRODUCTION
Circumcision, the surgical removal of the prepuce, is probably the most commonly performed procedure in the neonatal period.[1] It remains the commonest surgical operation in males in West Africa as only very few cultures do not observe it in the subregion.[2] While the indication for the procedure is often sociocultural[1] and the procedure is performed by different categories of clinical staff including doctors and nurses as well as auxiliary nurses and traditional circumcisionists; most of the major complications need the attention of the specialist surgeon-often Pediatric Surgeons or Urologists.[2,3] Most of the complications associated with the procedure are as a result of lack of adequate depth and attention to details of this simple procedure.[4,5] It is to be noted that re-do surgeries of this procedure is more difficult to perform and the outcome is often not as good as when it is well performed the first time.
Although the procedure is straightforward and simple to perform, complications from this procedure are as varied as the many different methods of (and probably as many men) performing the procedure. Careful attention to the steps of this procedure as well as avoidance of the pitfalls will reduce the complications following this common surgery.[3,5]
Complication rates as low as 1-3% has been reported in literature[6–8] however, in Nigeria, higher complication rates as high as 20% has been documented.[3] Majority of these complications would not require the intervention of the surgeon; however, more difficult complications will require the specialist's expertise.
The aim of this study is to document the pattern of complications of circumcision for which referral was made to the Paediatric Surgical Unit of Lagos University Teaching Hospital and treatment offered.
MATERIALS AND METHODS
A retrospective analysis of data from pediatric surgical outpatient clinic records, theater registers and casenotes were performed over a 24-month period. The records of all male children under the age of fifteen years who presented on account of complications of circumcision were studied.
The information retrieved included age of the patients, the specific complication(s) necessitating referral and the details of the surgical treatment offered. Data on the qualification of staff that performed the surgery and the kind of facility where the surgery was performed could not be retrieved for all the patients from the case notes and hence were not analyzed. The data was analyzed using SPSS version 13.0.
RESULTS
There were 36 cases of complications following male circumcision during the study period necessitating some form of surgical intervention or admission to the hospital. All of these were referred from other centers. During the study period, there were 1100 referrals in the pediatric surgery out- patient clinic and 472 admissions via the children emergency department. During the same period, there were 27 cases of circumcision performed in the unit. Hence the circumcision load was 4% of patient load in the unit; more than half of which is due to complications from referrals from peripheral hospitals.
The age range was between 2 days and 9 years with a median age of 3 months. Fifteen cases (41.7%) were due to urethro-cutaneous fistula while there were 6 cases (17.1%) of postcircumcision bleeding. There were four cases (11.1%) each of partial penile amputation and buried penis. There were three cases (8.3%) of meatal stenosis while there were two cases (5.6%) of penile implantation cyst and skin bridges each [Table 1.]
Table 1.
Complications of circumcision occurring in different age groups of patients

With respect to the treatment offered, 11 (73.3%) of the fifteen patients with urethro-cutaneous fistulae had urethroplasty while 7 patients had penile refashioning for the buried penis and penile amputation. A patient with buried penis is awaiting surgery. All the six patients who had post circumcision bleeding had haemostatic sutures applied while three patients with meatal stenosis had meatotomy. Four patients with urethro-cutaneous fistula and one with buried penis are still awaiting definitive surgery because they are still infants. The patient with implantation cyst had simple excision biopsy while the two patients with skin bridges had excision of the bridge.
DISCUSSION
Circumcision is a commonly performed surgical procedure by medical practitioners and paramedical staff alike. The procedure is routinely performed within the neonatal period in our environment usually due to religious and cultural reasons.[2] The complications following this procedure include those occurring intra-operatively and postoperatively.[9,10] The latter could occur in the immediate postoperative period or much later.
Intraoperative complications of circumcision include excessive primary hemorrhage and injury to adjacent structures including the glans penis, the urethra, penile shaft and even the scrotum as well as the neurovascular bundle of the penis.[9,11–14]
Immediate postoperative complications include: reactionary hemorrhage, meatitis, tetanus infection, wound infection, wound dehiscence, necrotizing fasciitis, penile amputation and occasionally septicemia.[15–17] Late presentation includes urethro-cutaneous fistulas, penile torsion, buried penis, implantation cysts and death which can occur at any time.[14,15]
Of the circumcision done in our department in the period under review, there were no complications necessitating surgical intervention or admission in the hospital. Most of the complications were those of mild meatitis which responded to antibiotics therapy.
However, we treated more patients with complications of circumcision from peripheral referrals than patients presenting for circumcision within our unit. This is not unexpected-the commonest indication for circumcision in our setting is socio-religious and cultural reasons and virtually all males are circumcised. As a result, a single center cannot cater for the circumcision needs of a cosmopolitan city like Lagos. Thus, most of the circumcisions in our environment are performed in the peripheral centers by medical officers, nurses, auxiliary nurses and traditional circumcisionists.[2] Furthermore, majority of circumcisions of male children born in our center are also performed outside by other categories of health workers rather than by specialists in the teaching hospital. While the exact reason for this could not be ascertained, long waiting list in the teaching hospital as well as cost implication might be responsible for this trend.
In this series, the commonest complication is urethro-cutaneous fistula. This finding is consistent with the findings of Bode et al.[2] in an earlier study in the same center. Similarly, Aina[18] also reported urethro-cutaneous fistula as the commonest complication in his series. It is one of the most severe and most feared complications of circumcision. This is understandable since most of the complications are treatable without any intervention by a specialist. However, for fistulas the need for a specialist necessitates the referral to us. Urethro-cutaneous fistula is an abnormal communication between the urethra and penile skin and this usually occurs around the corona of the glans. This site corresponds to the site of the frenular artery which is a cause of troublesome bleeding during the procedure. Attempt to arrest this bleeder by means of a ligature often causes a bite of the urethra resulting in this complication. Repair is usually accomplished by means of transverse closure of the defect in 2 layers or use of Mathieu style skin flap or double pedicle skin flap depending on the size and number of the fistula(e) [Figures 1a and 1b].[19,20]
Figure 1.
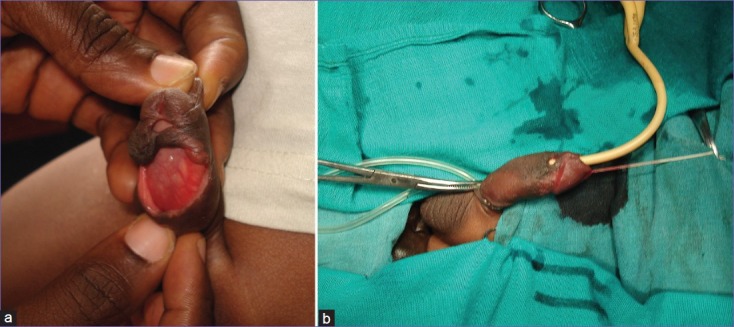
(a) Multiple urethrocutaneous fistula. Solid arrow: normal external urethral meatus. Dotted arrows: distal urethrocutaneous fistula. Double triangle: proximal urethrocutaneous fistula; (b) Simple, single orifice urethrocutaneous fistula.
Seven patients had refashioning of the penis; four were performed for patients with partial amputation of the penis while three were performed on account of buried penis. Of those with partial amputation of the penis, two of the patients had the whole of the glans amputated while in one patient part of the glans was amputated and in the last patient, the distal half of the penile shaft was chopped off. The treatment offered included early urethral catheterization to prevent meatal stenosis, administration of parenteral antibiotics to prevent sepsis. Penile refashioning was accomplished by releasing fibrous bands around the penile shaft after degloving the penis.
Although excessive bleeding secondary to excessive primary hemorrhage or reactionary hemorrhage has been reported to be the commonest complication following circumcision with an incidence of 0.1%-35%, we however noted that it is not the commonest reason for which referral to specialist center was made. This may be due to the fact that most cases of postcircumcision bleeding can be effectively treated by non-specialists by application of firm pressure, adrenaline soaked gauze packing and suture ligation.[9] The patients with postcircumcision bleeding presented within 48 hours of the procedure. Only one of them had bleeding dyscrasia-hemophilia. He had fresh frozen plasma transfused twice along with whole blood, sustained pressure dressings with adrenaline and application of haemostatic sutures to control his bleeding. The other patients were bleeding from the frenular vessels and careful application of “figure-of-eight” suture, taking care not to injure the urethra, sufficed.
Three patients with meatal stenosis following circumcision had meatotomy. This was accomplished by calibrating the meatus to accept a mosquito artery forceps. A lip of a curved Metzebaum scissors was introduced and the ventral urethra was cut followed by a muco-cutaneous anastomosis. The patient with implantation cyst had simple excision biopsy while two patients with preputio-glanular skin bridges had a sharp incision of the bridge after clamping with artery forcep for about 3-5 minutes following xylocaine without adrenaline infiltration.
In our series, we did not treat any patients with other possible complications of circumcision like redundant skin, meatitis, tetanus infection, wound infection, wound dehiscence, necrotizing fasciitis and septicaemia. This may be due to fewer numbers of cases in this series as well as the fact that most of these complications are treated medically and therefore, patients were commonly referred to the paediatricians.
CONCLUSION
In conclusion, circumcision could have significant morbidity associated with it. Urethro-cutaneous fistula and penile amputation were the commonest complications of circumcision for which referral was made to our center and urethroplasty and refashioning of the penile shaft were the commonest surgeries performed by us to correct circumcision complications. Health education of the populace on the need to perform circumcision by qualified personnel as well as regular certification and re-certification of Medical and Para-Medical staff is necessary to reduce the significant morbidity from this otherwise simple procedure.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gerhaz EW, Haarmann C. The first cut is the deepest. Medicolegal aspects of male circumcision? BJU Int. 2000;86:332–8. doi: 10.1046/j.1464-410x.2000.00103.x. [DOI] [PubMed] [Google Scholar]
- 2.Bode CO, Kene-Ewulu I. Complications of male circumcision in Lagos: Analysis of 90 cases. Nig Qt J Hosp Med. 1997;7:129–33. [Google Scholar]
- 3.Okeke LI, Asinobi AA, Ikuerowo SO. Epidemiology of complications of male circumcision in Ibadan, Nigeria. BMC Urol. 2006;6:21. doi: 10.1186/1471-2490-6-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cohen MS. Circumcision. In: Nyhus LM, Baker RJ, Fischer JE, Holmes CR, editors. Mastery of Surgery. Philadelphia: Lippincott Williams and Wilkins; 1996. [Google Scholar]
- 5.Ademuyiwa AO, Bode CO. Complications of neonatal circumcision: Avoiding common pitfalls in a common procedure. Afr J Paediatr Surg. 2009;6:134–6. doi: 10.4103/0189-6725.54786. [DOI] [PubMed] [Google Scholar]
- 6.Wiswell TE, Geschke DW. Risks from circumcision during the first month of life compared with those for uncircumcised boys. Pediatrics. 1989;83:1011–5. [PubMed] [Google Scholar]
- 7.Manji KP. Circumcision of the young infant in a developing country using the Plastibell. Ann Trop Paediatr. 2000;20:101–4. doi: 10.1080/02724936.2000.11748116. [DOI] [PubMed] [Google Scholar]
- 8.O’Brien TR, Calle EE, Poole WK. Incidence of neonatal circumcision in Atlanta, 1985-1986. South Med J. 1995;88:411–5. doi: 10.1097/00007611-199504000-00005. [DOI] [PubMed] [Google Scholar]
- 9.Williams N, Kapila L. Complications of circumcision. Br J Surg. 1993;80:1231–6. doi: 10.1002/bjs.1800801005. [DOI] [PubMed] [Google Scholar]
- 10.Kaplan GW. Complications of circumcision. Urol Clin North Am. 1983;10:543–9. [PubMed] [Google Scholar]
- 11.Ahmed A, Mbibu NH, Dawam D, Kalayi GD. Complications of traditional male circumcision. Ann Trop Pediatr. 1999;19:113–7. doi: 10.1080/02724939992743. [DOI] [PubMed] [Google Scholar]
- 12.Feinberg AN, Brust RA, Walker TA. Bleeding at circumcision: Patient or operator issue? Clin Pediatr (Phila) 2010;49:760–3. doi: 10.1177/0009922810364658. [DOI] [PubMed] [Google Scholar]
- 13.Weiss HA, Larke N, Halperin D, Schenker I. Complications of circumcision in male neonates, infants and children: A systematic review. BMC Urol. 2010;10:2–4. doi: 10.1186/1471-2490-10-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Krill AJ, Palmer LS, Palmer JS. Complications of circumcision. Scientific World Journal. 2011;11:2458–68. doi: 10.1100/2011/373829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Menahem S. Complications arising from ritual circumcision: Pathogenesis and possible prevention. Isr J Med Sci. 1981;17:45–8. [PubMed] [Google Scholar]
- 16.Naimer SA, Trattner A. Are sterile conditions essential for all forms of cutaneous surgery? The case of ritual neonatal circumcision. J Cutan Med Surg. 2000;4:177–80. doi: 10.1177/120347540000400401. [DOI] [PubMed] [Google Scholar]
- 17.Hsiao AL, Chen L, Baker MD. Incidence and predictors of serious bacterial infections among 57- to 180-day-old infants. Pediatrics. 2006;117:1695–701. doi: 10.1542/peds.2005-1673. [DOI] [PubMed] [Google Scholar]
- 18.Aina AO. Post-circumcision complications. W Afr J Surg. 1979;3:153–7. [Google Scholar]
- 19.Baskin LS, Canning DA, Synder HM, 3rd, Duckett JW., Jr Surgical repair of urethral circumcision injuries. J Urol. 1997;158:2269–71. doi: 10.1016/s0022-5347(01)68233-8. [DOI] [PubMed] [Google Scholar]
- 20.Chtourou M, Attyaoui F, Ben Younes A, Rekik H, Horchani A. Repair of urethrocutaneous fistula with double skin flap. Report of 32 cases. Prog Urol. 2000;10:261–4. [PubMed] [Google Scholar]