

Abstract
Leiomyomas are benign tumors arising from smooth muscle of the uterus. Intravenous leiomyomatosis is characterized by intraluminal growth of benign smooth muscle into either venous or lymphatic vessels outside the limits of myoma. It commonly extends into the pelvic veins and manifests as worm-like protrusions of tumor emanating from veins at the parametrial margins of hysterectomy specimen. The tumor can cause life-threatening symptoms if it involves inferior vena cava or right atrium. We report a case of intravenous leiomyomatosis of the uterus managed at our institution.
KEYWORDS: Intravenous leiomyomatosis, myometrium, uterus
INTRODUCTION
Leiomyomas are benign tumors arising from smooth muscle of the uterus. Although the radiological diagnosis is straight forward in most cases, Leiomyomas can occur in unusual locations or present with unusual growth patterns that make the diagnosis more challenging. Intravenous leiomyomatosis (IVL) is a rare tumour characterized by intraluminal growth of benign smooth muscle into either venous or lymphatic vessels outside the limits of myoma.
CASE REPORT
A 32-year-old woman was admitted with complaints of abdominal swelling and pain since 6 months. Pain abdomen was intermittent and confined to lower abdomen. She also had feeling of incomplete voiding of urine with overflow and stress incontinence since 3 months. Menstrual cycles were normal and there was no menorrhagia. She has one living child and underwent tubectomy 6 years ago. Abdominal examination revealed irregular, nontender uterine mass of 24 weeks pregnant size. Pelvic ultrasound showed bulky uterus measuring 9×6.8×4.3 cm, with multiple hypoechoic lesions in anterior and posterior myometrium, the largest one measuring 11×8.8×7 cm. Computed tomography (CT) scan was not done due to unavailability of the facility in the rural set-up as well as the unaffordability of the patient. As the mass was very big and the patient was symptomatic and had already completed her family, the decision of total abdominal hysterectomy was taken. Abdomen was opened by midline vertical incision. During surgery, multiple large subserosal, intramural, and submucosal fibroids ranging from 5×4 cm to 20×30 cm were seen. During surgical removal, the tumor showed worm-like projections into the pelvic veins [Figure 1]. A presumptive diagnosis of intravenous leiomyomatosis was made. Ovaries appeared healthy and were retained. There were no technical difficulties in removing the uterus. The tumor was very vascular; it started bleeding profusely from the cut margins. Bilateral hypogastric artery ligation was done which reduced uterine blood supply and enabled easy removal of the uterus. Hemostasis was well achieved. The tumor weighed 6.7 kg. The postoperative course was uneventful and she has been in good health for 16 months after the operation. Microscopic examination demonstrated the tumor cells invaginating the vascular tree with no evidence of atypia.
Figure 1.
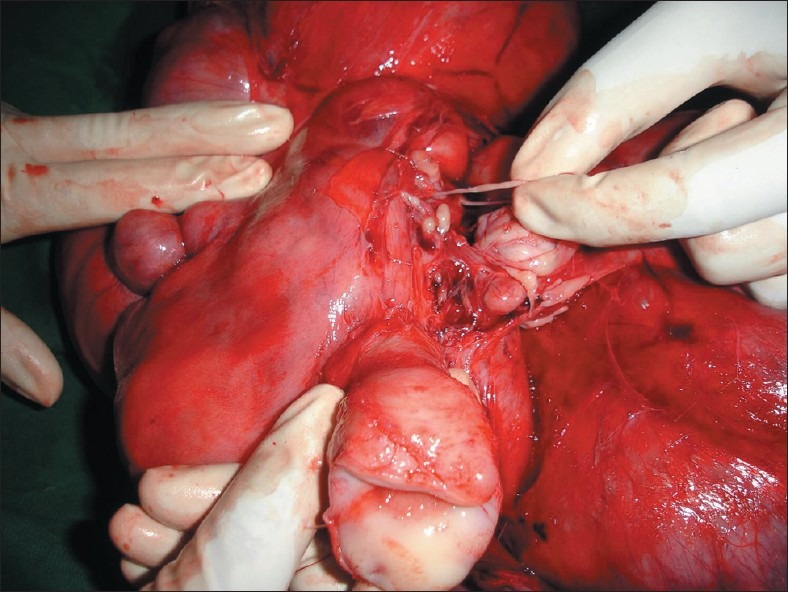
Inravenous leiomyomata
DISCUSSION
Intravenous leiomyomatosis was first described by Birch-Hirschfeld in 1896 and defined by Norris and Parmlyin in 1975.
The neoplasm may result from the invasion of myometrial sinuses by either leiomyomatosis cells or proliferating smooth muscle cells, arising directly from the venous wall of the uterine or pelvic veins.[1]
Most of the patients present in the 5th and 6th decades of life. Female gonadal steroids play a major role in the pathogenesis as the condition is associated with high estrogen levels.[2]
Early diagnosis may be difficult because patients may be asymptomatic despite extensive intravenous extension.[3] Symptoms may be associated with uterine myomas. Although there may be some difficulties in distinguishing such lesions from low-grade sarcomas, they are different histologically from sarcomatosis uteri because the intravenous plug is mainly smooth muscle in origin. The tumor behaves like a benign tumor, and the mitotic index is low with most active lesions showing only one mitosis per 15 high-power fields. Conservative surgery is usually adequate as the intravenous extensions are probably incapable of independent parasitic existence and remain dormant after removing the uterus. The prognosis is excellent even when tumor is left in pelvic veins. Extension of benign leiomyomatosis up to vena cava and right atrium has been reported. Several cases requiring open heart surgery to remove the intracardiac thrombosis have been successful without recurrence.
Intravenous leiomyomatosis is a rare but an important clinical situation. Knowledge about this condition and its recognition is important to provide the best treatment for the patients.
CONCLUSION
Prophylactic hypogastric artery ligation is safe and effective to reduce uterine blood supply before attempting hysterectomy for vascular uterine tumors. Though intravenous leiomyomatosis imitates malignant neoplasm regarding its pattern of growth and extension, it must be differentiated histologically from malignant tumors to avoid overtreatment. Since intravenous leiomyomatosis has a tendency for recurrence, long-term follow-up of patients is recommended.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Yaguchi C, Oi H, Kobayashi H, Miura K, Kanayama N. A case of intravenous leiomyomatosis with high levels of hyaluronan. J Obstet Gynaecol Res. 2010;36:454–8. doi: 10.1111/j.1447-0756.2009.01147.x. [DOI] [PubMed] [Google Scholar]
- 2.Quade BJ, Dal Cin P, Neskey DM, Weremowicz S, Morton CC. Intravenous leiomyomatosis: Molecular and cytogenetic analysis of a case. Mod Pathol. 2002;15:351–6. doi: 10.1038/modpathol.3880529. [DOI] [PubMed] [Google Scholar]
- 3.Worley MJ, Jr, Aelion A, Caputo TA, Kent KC, Salemi A, Krieger KH, et al. Intravenous leiomyomatosis with intracardiac extension: A single-institution experience. Am J Obstet Gynecol. 2009;201:574.e1–5. doi: 10.1016/j.ajog.2009.06.037. [DOI] [PMC free article] [PubMed] [Google Scholar]