

Description
Wilson's disease (WD) is an inborn error of copper metabolism with an autosomal recessive pattern of inheritance. It is caused by ATP7B mutation leading to abnormal accumulation of copper in various tissues, particularly the liver and the brain. MRI abnormalities occur in virtually 100% of patients with neurological dysfunction.1 The classical MRI findings include the face of a giant panda sign, the face of a miniature panda sign and bright claustrum signs.
This case illustrates a 16-year-old boy born of non-consanguinity with normal birth and development studying in the seventh standard presented with progressive neurological illness in the form of generalised dystonia involving all four limbs and a face with fixed vacant smile (risus sardonicus) for past 2 years. He had rest as well as kinetic limb tremor and cognitive impairment predominantly affecting executive function and memory with positive family history of (elder brother of age 18 year) WD. Laboratory investigation revealed the following: serum copper level of 60 µg/dL (N 85–150 µg/dL), serum ceruloplasmin level of 6.0 mg/dL (N 15–60 mg/dL), 24 h urinary copper, that is, 170 µg/day (normal 50–70 µg/day) with normal liver function test. Other routine blood investigations were non-contributory. Ultrasonogram of abdomen was normal except mild coarse echo texture of liver. Ophthalmological examination showed a thin rim of golden brown-coloured Kayser-Fleischer rings in the bilateral peripheral cornea (figure 1). An MRI of the brain with fluid-attenuated inversion recovery sequence showed the face of a giant panda sign, that is, hyperintensity in the midbrain tegmentum with normally hypointense red nucleus (eyes), preservation of signal intensity of the pars reticulate of the substantia nigra (ears), low signal intensity of the superior colliculous (chin) (figure 2). There is a thin rim of the T2 hyperintense lesion seen in the claustrum known as the bright claustrum sign (figure 3). The pontine section also revealed the face of a miniature panda sign where hypointensity of medial longitudinal fasciculus and central tegmental tract forming the eyes, hyperintensity of aqueduct opening into the fourth ventricle, the nose and mouth and the superior cerebellar peduncle form the panda's cheeks (figure 4). The above findings are consistent with diagnosis of WD. Neuroimaging findings similar to WD can be seen in number of other conditions such as Leigh disease, hypoxic–ischaemic encephalopathy, methyl alcohol poisoning, Japanese B encephalitis and in extrapontine myelinolysis. The characteristic clinical features of these entities distinguish them from WD.2
Figure 1.

Thin rim of golden to brown coloured Kayser-Fleischer rings present in bilateral cornea.
Figure 2.
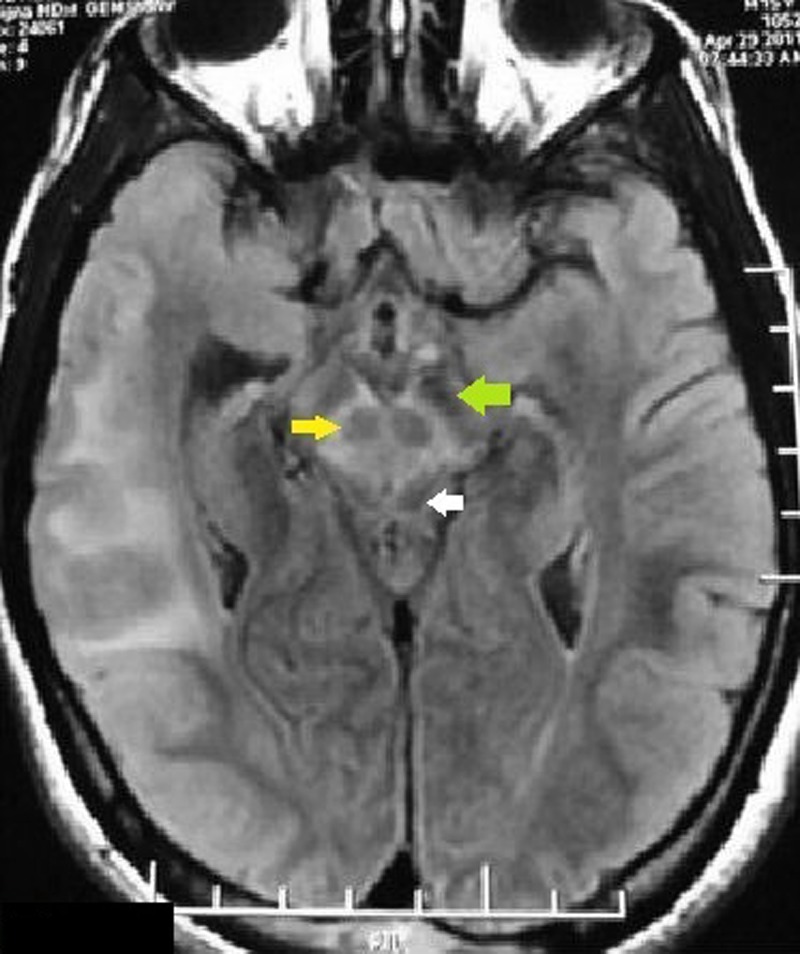
MRI of brain with fluid-attenuated inversion recovery sequence showing the face of a giant panda sign, that is, increased signal intensity in the midbrain tegmentum with normally hypointense red nucleus (eyes, yellow arrow), preservation of signal intensity of the pars reticulate of substantia nigra (ears, green arrow), low signal intensity of superior colliculous (chin, white arrow).
Figure 3.
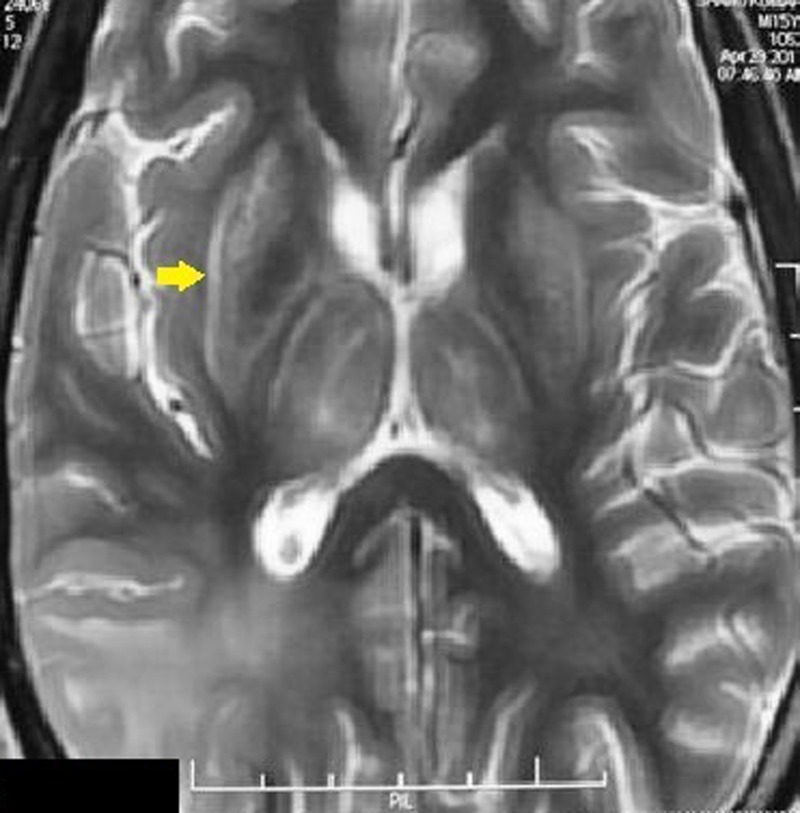
There is a thin rim of T2 hyperintensity in the claustrum known as the bright claustrum sign (yellow arrow).
Figure 4.
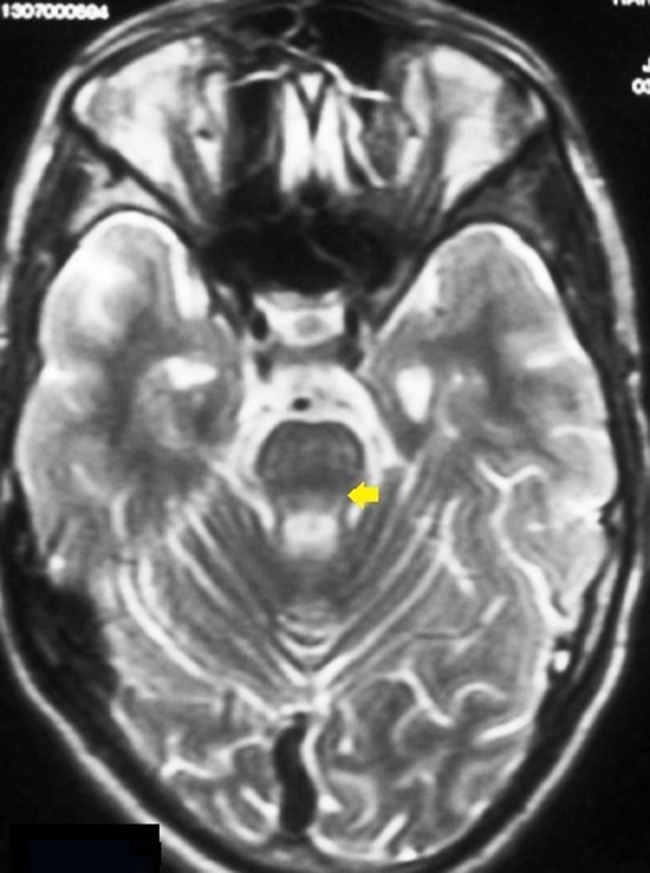
T2 sequence revealed the face of a miniature panda sign where hypointensity of medial longitudinal fasciculus and central tegmental tract (eyes), hyperintensity of aqueduct opening into the fourth ventricle (nose and mouth) and the superior cerebellar peduncle form the panda's cheeks (yellow arrow).
Inspite of the presence of excess copper within the brain, pathological findings are limited primarily to the basal ganglia, thalamus, mid brain and pons. Histopathology studies showed atrophy, spongy softening, cavitations, neuronal loss, increased cellularity and the presence of opalski cells.3 Though the classical neuroimaging findings are found only in few proportions of patient their presence yields the diagnostic clue.
Learning points.
A multitude of MRI abnormalities has been described in Wilson's disease which has diagnostic and prognostic implications.
Characteristics neuroimaging finding in Wilson's disease include the face of a giant panda sign, the face of a miniature panda sign and bright claustrum signs.
Apart from the above radiological features, parenchymal atrophy and alterations in signal intensity are also characteristics and can be found in most patients with Wilson's disease.
Footnotes
Contributors: AKP was involved in conception and design, analysis and interpretation of data, revising it critically for important intellectual content and approved the final version of the manuscript for publication.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Sinha S, Taly AB, Ravishankar S, et al. Wilson's disease: cranial MRI observations and clinical correlation. Neuroradiology 2006;2013:613–21 [DOI] [PubMed] [Google Scholar]
- 2.Das SK, Ray K. Wilson's disease: an update. Nat Clin Pract Neurol 2006;2013:482–93 [DOI] [PubMed] [Google Scholar]
- 3.Kim TJ, Kim IO, Kim WS, et al. MR imaging of the brain in Wilson disease of childhood: findings before and after treatment with clinical correlation. Am J Neuroradiol 2006;2013:1373–8 [PMC free article] [PubMed] [Google Scholar]