

Abstract
This twelve months survey compared injury risk and injury types by genders (312 females, 262 males) in 15- to 35-year-old cross-country skiers, swimmers, long- distance runners and soccer players. More male than female athletes reported at least one acute injury (44% vs. 35%, p < 0.05), and more male than female runners reported at least one overuse injury (69% vs. 51%, p < 0.05). When the incidence of acute and overuse injuries both separately and combined was calculated per 1000 training hours, per 1000 competition hours and all exposure hours combined we found no gender differences in either of these comparisons. After adjustment for sport event males were at increased risk for posterior thigh overuse injuries compared to females (relative risk (RR) 5.8, 95% confidence interval (CI) 1.3 to 26.4, p < 0.05) while females were at increased risk for overuse injuries in the ankle compared to males (RR 3.1, 95% CI 1.0 to 9.3, p < 0.05). After adjustment for exposure time (injuries/1000 exposure hours) significance of the difference between the sexes in overuse injury to the ankle persisted (female 0.11 vs. male 0.02 injuries/1000 exposure hours, p < 0.05). Six athletes had an anterior cruciate ligament (ACL) injury, of whom four were female soccer players. After combining all reported acute and overuse ankle and knee injuries, the proportion of athletes with such injury was higher in the female compared to male soccer players (75% and 54% respectively; p < 0.05), but no difference was found in such injuries when calculated per 1000 exposure hours. In conclusion, we found some gender differences in sport-related injuries, but most of these differences seemed to be explained at least in part by differences in the amount of training.
Key points.
Only a few sport injury studies have compared in-jury rates between the sexes
Overall gender-related risk for acute and overuse injuries in top-level athletes between the sexes was small
Some gender differences in the specific anatomical locations of injuries as well as in specific injuries in sports were found
Some of these differences seem to be explained by the differences in the amount of training
Key words: Male, female, athletic injuries, acute injury, over-use injury
Introduction
In general patterns of injuries in athletes have been assumed to be more sport- specific than gender-specific. Presently, most sport injury studies that have investigated gender differences have focused exclusively on knee injuries (Arendt and Dick, 1995; Dugan, 2005). To date, only a few sport injury studies have compared acute injury rates (Kujala et al., 1995) or overall injury rates (de Loes et al., 2000; Sallis et al., 2001) between the sexes.
Previous studies have found similar overall injury rates in men and women (Lanese et al., 1990; Sallis et al., 2001). In contrast some sports and recreation-related injury studies have shown male athletes to be at greater risk for injury than their female counterparts (Conn et al., 2003; Dempsey et al., 2005). Powell and Barber-Foss, 2000 and Elias et al. (2001) have reported that female soccer players had a higher incidence of injury than males.
Male athletes have been reported to have a higher risk for severe sport- related injuries than female athletes (Conn et al., 2003). Only a few studies have reported on gender differences in injuries related to cross-country skiing (Sandelin et al., 1980) and swimming (McMaster and Troup, 1993).
Specific to body location, females athletes have been reported to have more injuries to the hip (Sallis et al., 2001; Satterthwaite et al., 1999), lower leg and shoulder than male athletes, while males had more injuries in the thigh than females (Sallis et al., 2001). In marathon runners Satterthwaite et al., 1999 noticed that males had greater risk for hamstring and calf injuries than female runners. de Loes et al., 2000 reported that overall risk for knee injury in 12 sports was significantly higher for females than males. Similarly Arendt and Dick, 1995 found that knee injuries were more prevalent among female than male soccer players.
Overall, the literature of gender differences in injuries is limited. It is not known precisely whether the gender differences found are sport-specific only and thus related to training behaviors, or whether the difference in risk is related to biological gender differences.
Our purpose was to study differences in sport-related injuries between male and female elite athletes in four sports with different loading patterns. The sports were cross-country skiing, swimming, long-distance running and soccer.
Methods
Subjects
A questionnaire was sent to competitive top-ranking Finnish female and male athletes (age 15 - 35 years) after each competitive season. Overall, 1200 questionnaires were distributed with the sample represented four different sports and loading modalities for 300 cross-country skiers (repetitive loading to upper and lower extremities with pliant movements), 268 swimmers (repetitive loading to upper extremities without impact loads), 265 long-distance runners (repetitive loading to lower extremities with moderate impact loads) and 367 (21 teams) soccer players (higher for impact loads and sprains). The long-distance runners whose running distance was from 1500m to marathon were included in to the study. After excluding participants over 35 years of age and soccer teams with a low response rate, the final study target group consisted of 1075 athletes (Ristolainen et al., in press, 2009). The study protocol was approved by the ethics committee of the University of Jyväskylä.
Questionnaire
The 12-month structural retrospective sport injury questionnaire included items on anthropometry, training history, training and competition volume as well as on acute and overuse sport injuries during the past 12-month period. In addition, questions were asked about the anatomical location of the injury, type of injury and situation in which the injury was sustained (in training or competition). Female athletes were also asked about if the menstruation had begun, and in what age they started, the regularity or irregularity of menstrual cycle (oligo- or amenorrhea). The menstrual irregularity was defined as 6 menstruations or less per year or missing menstruation (Bennell and Alleyne, 2007). Also the number of menstrual cycles was asked during the past 12 months. The questionnaire has been previously validated against interview data (Eloranta and Tittonen, 2006; Karhula and Pakkanen, 2005).
The term acute injury was defined as an injury that occurs suddenly or accidentally, interrupting the athlete´s training or performing in a competition or causing an identifiable trauma. An acute injury was any physical injury which kept the athlete away from at least one training session, or competition, or needed a physician’s care. The term overuse injury was defined as an injury that causes pain during exercise loading without any noticeable external cause of injury. The injury gradually caused worsening pain during or after exercise. The pain got worse when the loading was continued and might cause the exercise to be stopped completely.
Statistics
The statistical analyses were done with the Statistical Package for the Social Sciences, version 15.0 (Norusis/SPSS, Inc., Chicago, Illinois). We calculated the results as absolute injury rates, comparing between the sexes. We then calculated injury rates as number of injuries per 1000 exposure hours i.e. hours spent on any type of training or on performing in competitions separately and combined. Injury rates were calculated separately for acute, overuse and all injuries. X2 statistics, t tests and analysis of variance (ANOVA) were applied to calculate statistical differences in gender distributions and between sports. Poisson regression was used to calculate the injury risk, adjusted for sport event, between the sexes.
Results
Six hundred and thirty-nine out of 1200 (53%) returned a questionnaire, from which 574 (312 female and 262 male) agreed to participate to this study. Final participation response rate was 48%. To investigate the reasons for not responding we sent one-page questionnaire to long-distance runners (99 athletes) who did not respond to our long questionnaire. The most common reported reason for non-response was the length of the questionnaire. Females reported less training (566 hours/year [h/yr]) during the past twelve months than males (636 h/yr, p < 0.05). The athletes reported on average 16.2 competition hours per year (female: 14.8 and male: 17.9, p = 0.08) for the whole sample. The average number of competition hours varied by sport because of different duration of competitions i.e. in swimmers vs. soccer players. Detailed sex-specific, anthropometric and training and competition information are shown in Table 1.
Table 1.
Anthropometrics and training data in four different sports. Data are means (±SD).
| CC skiing | Swimming | LD running | Soccer | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ♂ (n = 62) | ♀ (n =87) | ♂ (n= 71) | ♀ (n =83) | ♂ (n = 67) | ♀ (n = 76) | ♂ (n = 62) | ♀ (n = 66) | ♂ (n = 262) | ♀ (n = 312) | |
| Age (years) | 24.0 (4.1) | 21.8 (4.3)* | 19.0 (2.9) | 18.3 (2.9) | 25.3 (5.2) | 23.5 (5.3)* | 22.9 (3.0) | 21.1 (3.8)* | 22.7 (4.6) | 21.2 (4.5)** |
| Height (m) | 1.80 (.06) | 1.68 (.05)** | 1.84 (.07) | 1.70 (.06)** | 1.80 (.06) | 1.67 (.05)** | 1.83 (.06) | 1.67 (.06)** | 1.82 (.06) | 1.68 (.06)** |
| Body weight (kg) | 74.0 (6.1) | 59.3 (5.5)** | 78.8 (8.4) | 62.0 (6.7)** | 66.8 (6.6) | 53.5 (5.1)** | 78.8 (6.1) | 62.1 (7.0)** | 74.6 (8.5) | 59.2 (7.0)** |
| BMI (kg·m-2) | 22.8 (1.1) | 20.9 (1.4)** | 23.3 (1.8) | 21.4 (1.9)** | 20.6 (1.3) | 19.2 (1.3)** | 23.6 (1.2) | 22.2 (1.8)** | 22.6 (1.8) | 20.9 (1.9)** |
| CMP (days/year) | 43.9 (28.4) | 34.5 (25.7)* | 14.5 (15.6) | 12.0 (10.9) | 20.5 (25.0) | 12.0 (19.1)* | 11.4 (11.5) | 18.0 (20.4)* | 22.2 (24.4) | 19.5 (21.9) |
| Compet. (n/year) | 28.0 (7.7) | 26.0 (8.5) | 12.6 (6.6) | 11.8 (5.4) | 19.8 (11.4) | 18.1 (11.8) | 30.1 (13.4) | 32.4 (14.3) | 22.2 (12.2) | 21.6 (12.7) |
| RestTR(days/week) | 0.8 (0.5) | 0.9 (0.4) | 1.1 (0.6) | 1.1 (0.3) | 0.6 (0.6) | 0.9 (0.5)** | 1.3 (0.5) | 1.4 (0.6) | 1.0 (0.6) | 1.1 (0.5)* |
| RestC (days/week) | 1.2 (0.6) | 1.2 (0.5) | 1.4 (0.8) | 1.2 (0.5) | 0.9 (0.7) | 1.3 (0.7)** | 1.7 (0.5) | 1.6 (0.5) | 1.3 (0.7) | 1.3 (0.6) |
| Start training (age) | 7.4 (2.7) | 7.8 (3.4) | 8.0 (2.1) | 8.0 (2.2) | 11.7 (3.9) | 12.6 (5.5) | 6.2 (1.6) | 7.8 (2.3)** | 8.4 (3.4) | 9.0 (4.1) |
| Tr years | 12.9 (4.1) | 10.7 (4.6)* | 10.1 (2.9) | 9.7 (3.2) | 11.8 (5.3) | 9.1 (4.7)* | 15.1 (3.6) | 12.5 (3.6)** | 12.4 (4.4) | 10.4 (4.3)** |
| Tr hours | 594 (161) | 522 (142)* | 779 (340) | 755 (309) | 568 (283) | 532 (220) | 584 (262) | 445 (144)* | 636 (285) | 566 (242)* |
| Compet. hours | 17.4 (7.3) | 10.1 (7.4)** | 2.6 (12.8) | 0.7 (1.3) | 8.4 (9.5) | 7.1 (8.0) | 45.3 (20.1) | 47.8 (21.7) | 17.9 (21.0) | 14.8 (20.7) |
CC = Cross-country, LD = Long distance, BMI = body mass index, CMP = camping days, Compet. = competitions, RestTR = rest days during training season, RestC = rest days during competition season, Tr years = training years at least 2 times/wk, Tr hours = training hours in a year (hours/year, all kind of exercise), Compt. Hours = competition hours in a year.* p < 0.05, ** p < 0.001 Differences are shown between male and female in each sport and all sports together.
Acute Injuries
Two hundred and twenty-five athletes (39%) reported 432 acute injuries. More male than female athletes reported an acute injury (44% vs. 35%, p < 0.05); this was especially seen in soccer players (84% vs. 64%, p = 0.01). However, after the acute injuries were calculated per 1000 exposure hours (training and competition hours combined), no gender differences were found (Table 2). Moreover, no gender difference was found in any specific sports in acute injuries sustained in a competition when calculated per 1000 competition hours.
Table 2.
Injuries and injury rates between men and women in four different sports during the past twelve-month period.
| CC skiing | Swimming | LD running | Soccer | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ♂ (n = 62) | ♀ (n =87) | ♂ (n= 71) | ♀ (n 83) | ♂ (n = 67) | ♀ (n = 76) | ♂ (n = 62) | ♀ (n = 66) | ♂ (n = 262) | ♀ (n = 12) | |
| Acute injuries | ||||||||||
| No of injuries (n) | 24 | 41 | 54 | 39 | 36 | 31 | 111 | 96 | 225 | 207 |
| No of injured athletes n (%) | 16 (26) | 25 (29) | 27 (38) | 22 (27) | 21 (31) | 20 (26) | 52 (84) | 42 (64)* | 116 (44) | 109 (35)† |
| No of injured athletes with two or more injuries n (%) | 5 (31) | 10 (40) | 14 (52) | 10 (46) | 10 (48) | 8 (40) | 32 (62) | 31 (74) | 61 (53) | 59 (55) |
| Injuries per 1000 exposure hours (n/1000h) | 0.57 | 0.85 | 0.95 | 1.24 | 1.19 | 0.85 | 3.64 | 3.11 | 1.53 | 1.43 |
| Overuse injuries | ||||||||||
| No of injuries (n) | 45 | 65 | 55 | 62 | 66 | 59 | 34 | 47 | 200 | 233 |
| No of injured athletes n (%) | 30 (48) | 44 (51) | 36 (51) | 43 (52) | 46 (69) | 39 (51)‡ | 24 (39) | 30 (46) | 136 (52) | 156 (50) |
| No of injured athletes with two or more injuries n (%) | 13 (43) | 16 (36) | 12 (33) | 16 (37) | 16 (35) | 16 (41) | 5 (21) | 10 (33) | 46 (34) | 58 (37) |
| Injuries per 1000 exposure hours (n/1000h) | 1.19 | 1.46 | 0.97 | 1.92 | 1.89 | 1.48 | 1.18 | 2.14 | 1.31 | 1.73 |
| All injuries | ||||||||||
| No of injuries (n) | 69 | 106 | 109 | 101 | 102 | 90 | 145 | 143 | 425 | 440 |
| No of injured athletes n (%) | 35 (57) | 58 (67) | 45 (63) | 54 (65) | 55 (82) | 52 (68) | 57 (92) | 52 (79)§ | 192 (73) | 216 (69) |
| No of injured athletes with two or more injuries n (%) | 22 (63) | 30 (52) | 26 (58) | 26 (48) | 29 (53) | 27 (52) | 42 (74) | 40 (77) | 119 (62) | 123 (57) |
| Injuries per 1000 exposure hours (n/1000h) | 1.77 | 2.33 | 1.94 | 3.25 | 3.15 | 2.45 | 4.90 | 5.32 | 2.89 | 3.25 |
* Proportion of injured athletes with acute injuries was higher in male soccer players than in female players (p < 0.01). † Proportion of injured athletes with acute injuries was higher in male athletes than in female counterparts (p < 0.05). ‡ Proportion of injured athletes with overuse injuries was higher in male long-distance runners than female runners (p < 0.05). § Proportion of injured athletes with all injuries was higher in male soccer players than in female players (p < 0.05).
There were only a few significant gender differences in what body locations acute injuries occurred. A higher proportion of female athletes than male athletes had an acute injury at the heel (p < 0.05). More male than female athletes had an acute injury in the upper back (p < 0.05). After adjustment for sport event these differences were no longer statistically significant. The locations of acute injuries by genders are shown in more detail in Figure 1.
Figure 1.
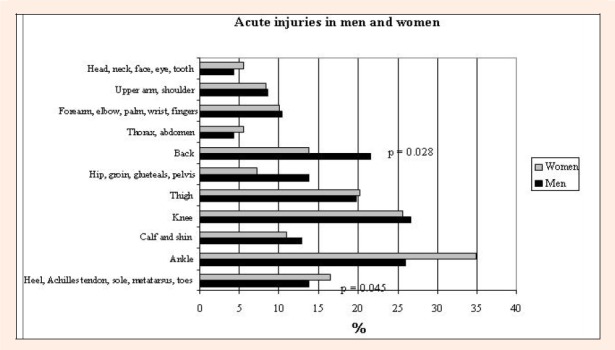
Location and proportions (%) of acute injuries by gender. A higher proportion of female than male athletes had acute injury in the heel (6% vs. 1%, p < 0.05). A higher proportion of male than female athletes had acute injury in the upper back (4% vs. 0 %, p < 0.05).
A higher proportion of men than women reported an acute muscle injury (44% vs. 31%, p < 0.05). After adjustment for sport event the difference was no longer statistically significant. A higher proportion of female (46%) than male athletes (33%) reported an acute ligament injury (p < 0.05) (Figure 2); this was seen especially in soccer players (71% vs. 42%, p < 0.01).
Figure 2.
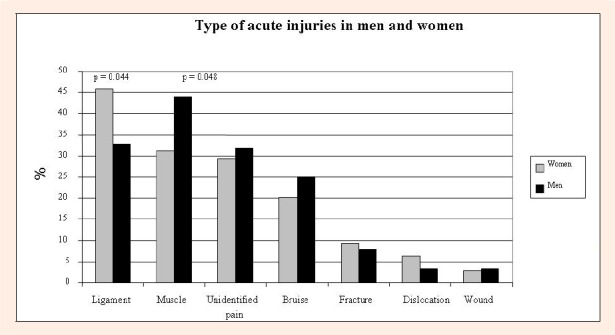
Proportion (%) of subjects with at least one acute injury in different tissues by gender. A higher proportion of female than male athletes had ligament injuries (46% vs. 33%, p < 0.05). A higher proportion of male than female athletes had muscle injuries (44% vs. 31%, p < 0.05).
Overuse Injuries
Four hundred and thirty-three overuse injuries were sustained by 292 athletes (51%). Overuse injuries were more prevalent among male than female runners (69% vs. 51%, p < 0.05), but there was no statistical significant difference found when the overuse injuries were calculated per 1000 exposure hours (Table 2).
The specific anatomical locations of overuse injuries by gender are shown in Figure 3. A higher proportion of men than women reported an injury in the posterior thigh (p < 0.01). This was especially seen in soccer players (p < 0.05). After adjustment for sport event male athletes were at increased risk for posterior thigh overuse injuries compared to female (RR 5.8, 95% CI 1.3-26.4, p < 0.05). In addition, more men than women reported toe (p < 0.05) and upper back (p < 0.05) injuries. A higher proportion of female than male athletes reported ankle (p < 0.05) injuries (Figure 3). After adjustment for sport event the risk for overuse ankle injury was greater in females than males (RR 3.1, 95% CI 1.0-9.3, p < 0.05). The ankle injury rate per 1000 exposure hours was also greater in female than male athletes (0.11 vs. 0.02, p < 0.05). A higher proportion of female than male cross-country skiers reported an overuse injury at the heel (p < 0.05), the injury rate being 0.14 in females and 0.0 in males per 1000 exposure hours (p < 0.05). There was found no gender differences in the proportion of overuse injuries by tissue type (Figure 4).
Figure 3.
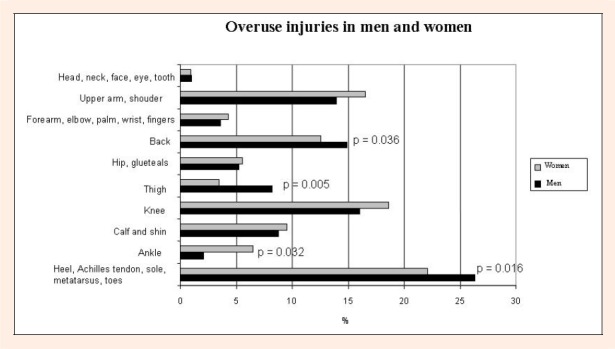
Location and proportions (%) of overuse injuries by gender. A higher proportion of male than female athletes had overuse injuries in the posterior thigh (8% vs. 1%, p < 0.01), toe (4% vs. 0%, p < 0.05), and upper back (4% vs. 1%, p < 0.05). A higher proportion of female than male athletes had overuse injuries in the ankle (9% vs. 3%, p < 0.05).
Figure 4.
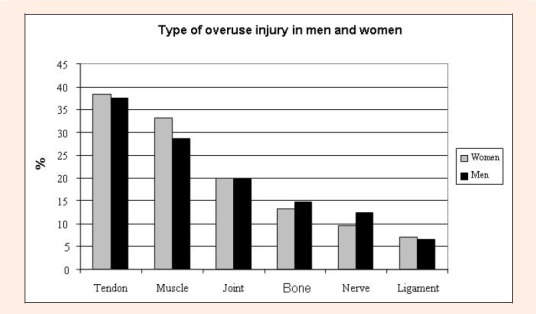
Proportion (%) of subjects with at least one overuse injury by tissue type and by gender.
All Injuries
A significantly higher proportion of male (92%) than female soccer players (79%, p < 0.05) reported at least one injury during the past twelve months. The same trend was found in long-distance runners, among whom 68% of female and 82% of male runners reported injury (p = 0.06 between the sexes).
When combining acute and overuse injuries of the ankle and the knee among all athletes, no difference was observed in the proportion of injured athletes between females (49%) and males (41%) (p = 0.13). After repeating the same analysis within sports between the sexes, the only significant difference was seen among soccer players. The proportion of female players with such an injury was higher than the proportion of male players (75% and 54% respectively; p < 0.05). In our study an anterior cruciate ligament (ACL) injury was identified in six cases, four of which were women. Five of these ACL injuries occurred in soccer players and one female player had been injured twice.
Menstrual Irregularities and Injuries
Menstrual irregularities were reported by 40 (13%) women and were more common among long-distance runners (26%) than soccer players (6%, p = 0.002) or swimmers (6%, p = 0.001). Cross-country skiers (16%) reported menstrual irregularities more often than swimmers (6%, p = 0.05) and the same trend was seen also in soccer players (6%, p = 0.07). The only difference between athletes with regular and those with irregular menses was found in overuse injury among cross-country skiers (46% vs. 85%, p = 0.01).
Discussion
The primary goal of our study was to investigate gender differences in sport-related injuries during the previous twelve months in four sports with different loading patterns. More male than female athletes had at least one acute injury. Also more male than female long-distance runners had at least one overuse injury. However, when we calculated the incidence of acute or overuse injuries as the number of injuries per 1000 exposure hours, we found no gender differences. A few gender differences were observed in the anatomical location of injuries. The main difference was a greater number of overuse injuries in the posterior thigh in male than female athletes, whereas females had a greater risk for overuse injuries to the ankle. The risk for such injuries remained after adjustment for sport event. A higher proportion of female soccer players had more combined acute and overuse injuries in the ankle and knee than male players.
More acute injuries per year have been reported among male than female athletes (Kujala et al., 1995; Sandelin et al., 1980). Powell and Barber-Foss, 2000 reported more acute injuries in girl than boy soccer players and Elias, 2001 showed slightly greater aggregate injuries in female than male soccer players. In addition, increased injury risk in female than male for swimmers (Sallis et al., 2001) and high-school cross-country runners (Rauh et al., 2000) has been reported. Overall, in accordance with our findings, Lanese et al., 1990 found no differences in overall injury incidence in different sports after adjustment for exposure time. However, Rauh et al., 2006 found gender differences after adjusting exposure time. It seems that possible gender differences in the injury rate may be partly due to or explained by differences in exposure time.
In a review, van Gent et al., 2007 reported that injury rates in the lower extremities were common in both female and male runners. The same finding was reported for cross-country skiers (Sandelin et al., 1980; Orava et al., 1985), which is in line with our results. An equal number of overuse injuries of the lower limbs was also found between males and females in sports other than swimming. In contrast to Sallis et al., 2001 and Satterthwaite et al., 1999 we found no gender difference between different groups of sport in injuries in the calf or hip. Sallis et al., 2001 studied injuries among athletes at the intercollegiate level and Satterthwaite et al., 1999 studied injuries and other health problems during a marathon race. Differences in study design, such as definition of the injury or different data collection methods, may explain these conflicting results.
Hamstring strains are common injuries in sports characterized by maximal sprinting, kicking and sudden acceleration (Lysholm and Wiklander, 1987). Waldén et al. (2005) reported that acute thigh injury in soccer players was the most common injury, causing a great amount of training and competition time loss. There is evidence showing that previous hamstring strains and age (Arnason et al., 2004) are independent risk factors for new hamstring strains. Thigh injuries may partly be explained by muscle fatigue, high training intensities, insufficient warm-up and hamstring tightness (Kujala et al., 1997), but the evidence for this is less convincing (Arnason et al., 2004; Bahr and Holme, 2003). In some cases the number of players per soccer team may be low and therefore the high amount of playing time per player may increase the risk for thigh injuries, and also the risk for overall injuries. In our study there was no difference between the sexes in acute thigh injuries. However, a higher proportion of our male than female athletes had overuse injuries in the posterior thigh, which is in line with the findings of earlier studies (Satterthwaite et al., 1999; Sallis et al., 2001) and clinical experience. Hosea et al., 2000 found in basketball players that females had greater overall risk for ankle injury than males. In our study females had a three-fold greater risk than males for overuse injury in the ankle. Higher joint laxity in females may contribute to this finding (Rozzi et al., 1999; Quatman et al., 2008).
Similar to the study by McMaster and Troup, 1993 on elite swimmers, in our swimmers overuse injuries occurred mostly in the shoulder region and no gender differences were found. Upper back injuries were rare in our female swimmers. Sallis et al., 2001 reported more injuries in college female than male swimmers in the shoulder and back/neck region. They suggested that a possible explanation for this difference may be training intensity. However, we did not investigate the training intensity, but there was no gender difference in the amount of training during the past twelve months.
Female compared to male basketball or soccer players have shown increased risk for traumatic ankle injury (Hosea et al., 2000; Elias, 2001). Among our soccer players females had slightly more acute ankle injuries than males. Moreover, women had more overuse injuries in the ankle and in the wrist than men. While especially ankle injuries are common in both genders, effective methods of preventing sports injuries, such as use of insoles, external joint supports and multi-intervention training programs, have been proposed to prevent injuries (Aaltonen et al., 2007).
Women have been reported to have more knee injuries than men, especially ACL injuries (Arendt and Dick, 1995; de Loes et al., 2000; Dugan, 2005). Female soccer players at the time of injury have been found to be younger than male players (Bjordal et al., 1997). During the present one-year follow-up time only one male soccer player suffered from an ACL injury, but no age difference was found between the female soccer players who had ACL injury (22.3 yr) and those who did not (21.0 yr, p = 0.53). Overall, we found similar numbers of knee injuries between men and women in all four sports. Haapasalo et al., 2007 also found no gender differences in overall knee injury risk, except in endurance sports. When acute and overuse injuries in the ankle and knee were combined, female soccer players had more such injuries than male players, as has been found in earlier studies both for the ankle (Hosea et al., 2000; Elias, 2001) and for the knee (Arendt and Dick, 1995; de Loes et al., 2000; Dugan, 2005) separately. Such injuries may also cause long absence time from training and competition. However, in our study there was no difference between the sexes in time-loss from acute or overuse injury (data not shown). Injury severity is described in more details in our previous article (Ristolainen et al., in press, 2009).
Female sex has been found to be a risk factor for stress fractures in the military population (Mattila et al., 2007), but less so in athletes (Snyder et al., 2006). Iwamoto and Takeda, 2003 concluded in their review that male athletes tend to have more stress fractures than women. The findings are inconsistent as Bennell et al. (1996a, 1996b) found an association between menstrual disturbances and stress fractures among runners, but Sandelin et al., 1980 found no association when studying cross-country skiers. There was 9.0% of stress fractures in female and 8.8% in male athletes. Nearly 50 % of female’s stress fractures occurred to those female athletes with menstrual irregularities. So, the statistically non-significant association between menstrual irregularities and stress fractures may be due to low statistical power (type two error).
Approximately one out of every fourth female athletes report having a menstrual irregularity (Nichols et al., 2006; Torstveit and Sundgot-Borgen, 2005), and these have been more common in long-distance runners, ballet dancers and gymnasts than in swimmers (Nichols et al., 2006, Torstveit and Sundgot-Borgen, 2005). Our long-distance runners also had significantly more menstrual irregularities than soccer players and swimmers. However, we did not find any association between stress fractures and menstrual irregularities. After adjustment for exposure hours we found no association between menstrual irregularities and in the number of injuries.
In our study the average competition time between sports was fairly different (in particular between swimming and soccer playing). However, there were no difference between the sexes in the acute injury occurred in the competition within all athletes or within different sport.
We studied gender differences in four different sports, and the injury risk was counted per 1000 exposure hours. It should be noted that these sports types differed from each other in loading characteristics and that there was only one contact sport. This can be considered both a strength and a limitation in our study, as our results indicate that gender differences are independent of type of sport. However, the low number of injuries limited some sport-specific injury comparations. We sent the questionnaire to the participants immediately after the competition season, and in each sport the response rate was similar. The limitations of this study include the use of self-reported questionnaire. However, the questionnaire data were validated and reliability-tested against the interview data, and were shown to be accurate (Eloranta and Tittonen, 2006; Karhula and Pakkanen, 2005). Retrospective data collection is a limitation in our study. Also, the validation method we used does not exactly reveal the accuracy and coverage of the reported injuries, but was more adequate for measuring the reproducibility/repeatability of the data collection. Comparability between different sports should not be a problem in our study as the method applied was the same for all four sports studied. In addition, the athletes in each sport were on the top-ranking list in their sports, and for this reason were to some extent comparable despite their different sport events.
Conclusion
The overall gender-related risk for acute and overuse injuries in top-level athletes between the sexes was small. However, we found some gender differences in the specific anatomical locations of injuries as well as in specific injuries in sports. Some of these differences seem to be explained by the differences in the amount of training.
Acknowledgements
This study was supported by a grant from the ORTON Research Institute, ORTON Foundation.
Biographies

Leena Ristolainen
Employment
Development Manager, ORTON Ortho-paedic Hospital, ORTON Foundation, Helsinki, Finland.
Degree
PT, MSc
Research interests
Sport medicine.
E-mail: leena.ristolainen@orton.fi
Ari Heinonen
Employment
Professor of Physiotherapy, Department of Health Sciences, University of Jyväskylä, Finland.
Degree
PT, PhD
Research interests
Sport medicine.
E-mail: ari.heinonen@sport.jyu.fi

Benjamin Waller
Employment
Physiotherapist, LIKES Sports Medicine Clinic, LIKES, Jyväskylä, Finland Department of Health Sciences, University of Jyväskylä, Finland.
Degree
BSc (Hons) Physiotherapy
Research interests
Sport medicine, aquatic sports and reha-bilitation.
E-mail: ben.waller@likes.fi
Urho M. Kujala
Employment
Professor of Sports & Exercise Medicine Department of Health Sciences, University of Jyväskylä, Finland.
Degree
MD, PhD
Research interests
Has published more than 150 scientific articles related to physical activity and health.
E-mail: urho.kujala@sport.jyu.fi
Jyrki A. Kettunen
Employment
Research Chief, ORTON Research Institute, ORTON Foundation, Helsinki, Finland.
Degree
PT, PhD
Research interests
Sport medicine, physiotherapy.
E-mail: jyrki.kettunen@orton.fi
References
- Aaltonen S., Karjalainen H., Heinonen A., Parkkari J., Kujala U.M. (2007) Prevention of sports injuries: systematic review of randomized controlled trials. Archives of Internal Medicine 167, 1585-1592 [DOI] [PubMed] [Google Scholar]
- Arendt E., Dick R. (1995) Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. American Journal of Sports Medicine 23, 694-701 [DOI] [PubMed] [Google Scholar]
- Arnason A., Sigurdsson S.B., Gudmundsson A., Holme I., Engebretsen L., Bahr R. (2004) Risk factors for injuries in football. American Journal of Sports Medicine 32, 5S-16S. [DOI] [PubMed] [Google Scholar]
- Bahr R., Holme I. (2003) Risk factors for sports injuries--a methodological approach. British Journal of Sports Medicine 37, 384-392 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennell K.L., Malcolm S.A., Thomas S.A., Wark J.D., Brukner P.D. (1996a) The incidence and distribution of stress fractures in competitive track and field athletes. A twelve-month prospective study. American Journal of Sports Medicine 24, 211-217 [DOI] [PubMed] [Google Scholar]
- Bennell K.L., Malcolm S.A., Thomas S.A., Reid S.J., Brukner P.D., Ebeling P.R., Wark J.D. (1996b) Risk factors for stress fractures in track and field athletes. A twelve-month prospective study. American Journal of Sports Medicine 24, 810-818 [DOI] [PubMed] [Google Scholar]
- Bennell K., Alleyne J. (2007) Women and activity-related issues across the lifespan. Clinical Sports Medicine: : Brukner P, Khan K.3th edition Sydney: The McGrow-Hill Companies; 749-772 [Google Scholar]
- Bjordal J.M., Arnly F., Hannestad B., Strand T. (1997) Epidemiology of anterior cruciate ligament injuries in soccer. American Journal of Sports Medicine 25, 341-345 [DOI] [PubMed] [Google Scholar]
- Conn J.M., Annest J.L., Gilchrist J. (2003) Sports and recreation related injury episodes in the US population, 1997-99.[see comment]. Injury Prevention 9, 117-123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Loes M., Dahlstedt L.J., Thomee R. (2000) A 7-year study on risks and costs of knee injuries in male and female youth participants in 12 sports. Scandinavian Journal of Medicine & Science in Sports 10, 90-97 [DOI] [PubMed] [Google Scholar]
- Dempsey R.L., Layde P.M., Laud P.W., Guse C.E., Hargarten S.W. (2005) Incidence of sports and recreation related injuries resulting in hospitalization in Wisconsin in 2000. Injury Prevention 11, 91-96 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dugan S.A. (2005) Sports-related knee injuries in female athletes: what gives? American Journal of Physical Medicine & Rehabilitation 84, 122-130 [DOI] [PubMed] [Google Scholar]
- Elias S.R. (2001) 10-year trend in USA Cup soccer injuries: 1988-1997. Medicine & Science in Sports & Exercise 33, 359-367 [DOI] [PubMed] [Google Scholar]
- Eloranta I., Tittonen T. (2006) The reliability and validity of sport injury questionnaire in questions concerning acute and overused injuries. (In Finnish: English abstract), Physiotherapy, University of Jyväskylä [Google Scholar]
- Haapasalo H., Parkkari J., Kannus P., Natri A., Jarvinen M. (2007) Knee injuries in leisure-time physical activities: a prospective one-year follow-up of a Finnish population cohort. International Journal of Sports Medicine 28, 72-77 [DOI] [PubMed] [Google Scholar]
- Hosea T.M., Carey C.C., Harrer M.F. (2000) The gender issue: epidemiology of ankle injuries in athletes who participate in basketball. Clinical Orthopaedics & Related Research 372, 45-49 [DOI] [PubMed] [Google Scholar]
- Iwamoto J., Takeda T. (2003) Stress fractures in athletes: review of 196 cases. Journal of Orthopaedic Science 8, 273-278 [DOI] [PubMed] [Google Scholar]
- Karhula K., Pakkanen S. (2005) The reliability and validity of sport injury questionnaire in the questions concerning recurrent and career-ending injuries. (In Finnish: Englih abstract; ). Available from URL: http://thesis.jyu.fi/05/URN_NBN_fi_jyu-2005378.pdf, in Physiotherapy, University of Jyväskylä [Google Scholar]
- Kujala U.M., Orava S., Jarvinen M. (1997) Hamstring injuries. Current trends in treatment and prevention. Sports Medicine 23, 397-404 [DOI] [PubMed] [Google Scholar]
- Kujala U.M., Taimela S., Antti-Poika I., Orava S., Tuominen R., Myllynen P. (1995) Acute injuries in soccer, ice hockey, volleyball, basketball, judo, and karate: analysis of national registry data.[see comment] British medical journal 311, 1465-1468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanese R.R., Strauss R.H., Leizman D.J., Rotondi A.M. (1990) Injury and disability in matched men’s and women’s intercollegiate sports. American Journal of Public Health 80, 1459-1462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lysholm J., Wiklander J. (1987) Injuries in runners. American Journal of Sports Medicine 15, 168-171 [DOI] [PubMed] [Google Scholar]
- Mattila V.M., Niva M., Kiuru M., Pihlajamaki H. (2007) Risk factors for bone stress injuries: a follow-up study of 102,515 person-years. Medicine & Science in Sports & Exercise 39, 1061-1066 [DOI] [PubMed] [Google Scholar]
- McMaster W.C., Troup J. (1993) A survey of interfering shoulder pain in United States competitive swimmers. American Journal of Sports Medicine 21, 67-70 [DOI] [PubMed] [Google Scholar]
- Nichols J.F., Rauh M.J., Lawson M.J., Ji M., Barkai H.S. (2006) Prevalence of the female athlete triad syndrome among high school athletes. Archives of Pediatrics & Adolescent Medicine 160, 137-142 [DOI] [PubMed] [Google Scholar]
- Orava S., Jaroma H., Hulkko A. (1985) Overuse injuries in cross-country skiing. British Journal of Sports Medicine 19, 158-160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Powell J.W., Barber-Foss K.D. (2000) Sex-related injury patterns among selected high school sports. American Journal of Sports Medicine 28, 385-391 [DOI] [PubMed] [Google Scholar]
- Quatman C.E., Ford K.R., Myer G.D., Paterno M.V., Hewett T.E. (2008) The effects of gender and pubertal status on generalized joint laxity in young athletes. Journal of Science and Medicine in Sport 11, 257-263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rauh M.J., Margherita A.J., Rice S.G., Koepsell T.D., Rivara F.P. (2000) High school cross country running injuries: a longitudinal study. Clinical Journal of Sport Medicine 10, 110-116 [DOI] [PubMed] [Google Scholar]
- Rauh M.J., Koepsell T.D., Rivara F.P., Margherita A.J., Rice S.G. (2006) Epidemiology of musculoskeletal injuries among high school cross-country runners. American Journal of Epidemiology 163, 151-159 [DOI] [PubMed] [Google Scholar]
- Ristolainen L., Heinonen A., Turunen H., Mannström H., Waller B., Kettunen J.A., Kujala U.M. (2009) Type of sport is related to injury profile: A study on cross-country skiers, swimmers, long-distance runners and soccer players. A retrospective twelve-month study. Scandinavian Journal of Medicine & Science in Sports, in press [DOI] [PubMed] [Google Scholar]
- Rozzi S.L., Lephardt S.M., Gear W.S., Fu F.H. (1999) Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. American Journal of Sports Medicine 27, 312-319 [DOI] [PubMed] [Google Scholar]
- Sallis R.E., Jones K., Sunshine S., Smith G., Simon L. (2001) Comparing sports injuries in men and women. International Journal of Sports Medicine 22, 420-423 [DOI] [PubMed] [Google Scholar]
- Sandelin J., Kiviluoto O., Santavirta S. (1980) Injuries of competitive skiers in Finland: a three year survey. Annales Chirurgiae et Gynaecologiae 69, 97-101 [PubMed] [Google Scholar]
- Satterthwaite P., Norton R., Larmer P., Robinson E. (1999) Risk factors for injuries and other health problems sustained in a marathon. British Journal of Sports Medicine 33, 22-26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder R.A., Koester M.C., Dunn W.R. (2006) Epidemiology of stress fractures. Clinics in Sports Medicine 25, 37-52 [DOI] [PubMed] [Google Scholar]
- Torstveit M.K., Sundgot-Borgen J. (2005) Participation in leanness sports but not training volume is associated with menstrual dysfunction: a national survey of 1276 elite athletes and controls. British Journal of Sports Medicine 39, 141-147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walden M., Hagglund M., Ekstrand J. (2005) Injuries in Swedish elite football--a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scandinavian Journal of Medicine & Science in Sports 15, 118-125 [DOI] [PubMed] [Google Scholar]
- van Gent R.N., Siem D., van Middelkoop M., van Os A.G., Bierma-Zeinstra S.M., Koes B.W. (2007) Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. British Journal of Sports Medicine 41, 469-480; discussion 480. [DOI] [PMC free article] [PubMed] [Google Scholar]