

Abstract
Previous literature has shown that sedentary older women rely on peripheral adaptations to improve cardiorespiratory fitness with endurance training i.e. they show minimal increases in central parameters (cardiac output, Q) in response to endurance training. The purpose of this study therefore was to determine whether endurance trained older women were able to preserve maximal exercise Q and were characterized by a high stroke volume (SV) when compared to physically inactive older women. Trained (n = 7) and untrained (n = 1 0) women attended two maximal and one submaximal laboratory session. Breath-by-breath analysis was conducted using mass spectrometry and Q was assessed using acetylene open circuit inert gas wash-in. Multivariate analysis of variance and paired samples t-tests were used to determine between and within group differences. Trained women had a significantly higher VO2max (37.5 vs. 24.1 ml-1·kg·min-1) compared to untrained women. There were no differences for peripheral oxygen extraction (VO2/Q) at either submaximal or maximal work rates; however trained women had a significantly higher SV at maximal (119.3 vs. 94.6 ml) exercise compared to untrained women. In both trained and untrained women, SV did not rise significantly between submaximal and maximal exercise. Conclusion: Highly fit, endurance trained older women are able to preserve central parameters of VO2max. Peripheral oxygen extraction is similar between older trained and untrained women.
Key points
Older women are able to preserve stroke volume with high volumes of endurance training.
Stroke volume of endurance trained older women does not continue to rise until maximal exercise, as is the case in young endurance trained adults.
Peripheral oxygen extraction does not differ between endurance trained and physically inactive older women.
Key words: cardiac output, aging, exercise, running, VO2max
Introduction
In those who are endurance trained, a higher maximal oxygen uptake (VO2max) is typically due to both a higher maximal cardiac output (Q) and peripheral oxygen extraction (arterio-venous oxygen difference, (a-v)O2diff); however, research has shown that this may not be the case among older women. While exercise training studies among older women do result in increases in VO2max, changes in the central component are minimal (Spina, 1999; Stachenfeld et al., 1998). In fact, this lack of central adaptation among older women was recently observed in a 12 week training study conducted in our laboratory with a group of recreationally active older (aged 69 ± 7) and younger (aged 25 ± 5) women (Murias et al., 2010a). While both age groups had a similar percent improvement in VO2max, the majority of the increase in older women was attributed to a widened peripheral oxygen extraction [(a-v)O2diff] compared to a greater contribution of Q among younger women. In older men, the increase in VO2max with training was mainly attributable to an increased Qmax and maximal stroke volume (SV), similar to that observed in the young women (Murias et al., 2010b). Thus, it seems that a lack of central adaptation may limit the ability of older women to improve their cardiac function and VO2max with exercise.
The volume and/or intensity of the exercise stimulus may also play an important role in attenuating age-related declines in cardiac function and VO2max; decreases in volume and engaging in light-moderate intensity exercise are associated with fewer improvements (Eskurza et al., 2002; Kemi et al., 2005; Swain and Franklin, 2006). Further, it is thought that individuals who were highly active in the past may have a greater trainability of central and peripheral systems despite recent inactivity, suggesting a potential reserve (Paterson and Cunningham, 1999). Finally, it is possible that genetically pre-determined individual differences and trainability might influence the ability for improvement in each of the components of VO2max (Bouchard and Rankinen, 2001).
There is limited data available on the parameters of VO2max in endurance trained older women. Nevertheless, in contrast to the concept that endurance training in older women results in minimal changes in stroke volume, McCole et al., 2000 reported that the higher VO2max of endurance-trained postmenopausal women compared with sedentary counterparts was attributable to higher SVs. The purpose of this study therefore was re-examine the exercise response in endurance-trained older women to determine which parameters, central or peripheral, are responsible for greater VO2max (associated with high volumes of endurance training) in endurance trained older women as compared to older women who are physically inactive and have an "average" VO2max. It was hypothesized that endurance trained women would have a higher maximal Q and SV but also a greater maximal (a-v)O2diff.
Methods
Study design and participants
The study was cross-sectional in nature. Participants were recruited from the London, Ontario area. Inclusion was limited to women between the ages of 60-85 years without any chronic cardiovascular, respiratory or musculoskeletal conditions and to those who were cleared by a physician upon completing a stress test. Older women were deemed eligible for the trained (T) group (n = 10) if they had participated in an endurance event (e.g., 5k or marathon) that required training in the past 6 months or if they were currently training for an endurance event. Older women in the untrained (UT) group (n = 10) were those who were recreationally active but were not meeting the minimum physical activity recommendations (Paterson and Warburton, 2010). All participants provided informed consent prior to testing and all procedures were approved by The University of Western Ontario Research Ethics Board for Health Sciences Research Involving Human Subjects.
Protocol
Maximal: Participants performed a maximal cycle ergometer ramp test to exhaustion (T: 20 Watts (W)·min-1; UT: 15 W·min-1) on a Lode Corival 400 cycle ergometer (Lode BV, Groningen, The Netherlands) to determine VO2max and to estimate gas exchange threshold (GET). GET was defined as the VO2 at which exhaled CO2 (VCO2) began to increase out of proportion to VO2 along with a systematic rise in minute ventilation-to-VO2 ratio and end-tidal PO2 (Beaver et al., 1986; Whipp et al., 1986). Within 5 minutes of completing this test, participants performed an acetylene wash-in for Qmax determination (described below) during constant load cycling exercise to volitional fatigue at approximately 85% of the peak power output achieved during the ramp incremental test. That is, when the participant indicated that they felt they could only sustain exercise for one more minute, the Q measures were initiated. Usually this was in the time frame of 3 minutes into the 85% bout. This protocol (described elsewhere Murias et al., 2010a; 2010b; Rossiter et al., 2006)) was performed to confirm the attainment of VO2max and for determination of Qmax. VO2max was defined as the highest average VO2 observed for 20 consecutive seconds during the ramp test to exhaustion. This protocol was repeated on a separate day to confirm VO2max and Qmax; the highest VO2 and an average of the two Q measures were used for analysis.
Submaximal: On a third day, participants were asked to repeatedly cycle at a power output corresponding to approximately 90% of their GET; three 6 minute bouts of submaximal (SM) exercise were separated by 6 minutes of unloaded cycling at 20W. SM Q was measured when a steady state in gas exchange was achieved. VO2 and Q obtained from the three bouts were averaged to provide one SM number for analysis.
Measures
Gas exchange measurements were similar to those previously described (Babcock et al., 1994). Briefly, inspired and expired flow rates were measured using a low dead space (90 ml) bidirectional turbine (VMM 110; Alpha Technologies, Akron, OH), which was calibrated before each test. Inspired and expired gases were sampled continuously (every 20 ms) at the mouth and analyzed for concentrations of O2, CO2, nitrogen (N2), acetylene (C2H2), and helium (He) by mass spectrometry (MGA-1100; Perkin Elmer, St. Louis, MO) after calibration. Breath-by-breath alveolar gas exchange was calculated by using algorithms of Beaver et al., 1981. Heart rate (HR) was monitored continuously by electrocardiogram using PowerLab (ADInstruments, Colorado Springs, CO) with a three-lead arrangement. Data were recorded using LabChart 7.0 (ADInstruments, Colorado Springs, CO) on a separate computer.
Central and peripheral components: Q was measured using the acetylene (C2H2) open-circuit inert gas wash-in method and analyzed using custom data acquisition software. This technique was described and validated previously (Johnson et al., 2000). Briefly, a pneumotachograph (Model 3800; Hans Rudolph, Kansas City, MO) and transducer (MP45-871; Validyne, Northridge, CA) were attached to a non-rebreathing Y valve (Model 7900; Hans Rudolph), which was connected to a manual valve that allowed switching inspired gases between room air and a bag containing a mixture of C2H2 (0.7%), O2 (21%), He (9%), and balance N2. This technique has been shown to be highly reliable, with decreasing error as exercise intensity increases (Dibski et al., 2005). Further, this method compares well to other techniques and provides values that are reliable at maximum exercise (Barker et al., 1999). Data analysis for the calculation of Q was performed immediately after each manoeuvre using equations reported previously (Johnson et al., 2000) and a fixed blood solubility factor (0.74 ml C2H2 (STPD)·ml blood-1·atm-1). These calculations were conducted automatically by the computer software program upon completion of each test. Prior to the maximal and SM exercise tests, participants were asked to complete one to two maneuvers of the Q technique in order to obtain baseline (i.e., resting) measures.
The Fick equation was used to calculate (a-v)O2diff as follows: (a-v)O2diff ml O2·100 ml-1 blood = (VO2 L·min-1/ Q L·min-1)X 100. SV was calculated as follows: SV ml·beat-1 = Q ml·min-1/ HR bpm. The slope of the line between SM and maximal VO2 was also calculated for SM and maximal SV for each participant using the following formula (SVmax-SV SM)/(VO2max-VO2 SM).
Statistical analysis
Data are presented as means ± standard error (SE). Pearson correlation coefficients were calculated for SM and maximal Q to determine reliability. Independent samples t-tests were used to compare sample characteristics, the four main outcomes (Q, SV, HR and (a-v)O2diff ) and VO2 (at SM and maximal exercise) as well as the slope (compared to zero) between the T and UT group. Paired samples t-tests were used to determine within group differences for each of the four main outcomes from SM to maximal exercise. Finally, multivariate analysis of variance and pairwise comparisons were conducted using HR, SV and (a-v)O2diff first for SM then for maximal data. This analysis was used to ensure that findings from independent samples t-tests were accurate and because of the relatedness of the three variables. All statistics were conducted in SPSS 17.0 (SPSS Inc., Chicago, IL). Statistical significance was declared when p < 0.05.
Results
All participants were post-menopausal; two participants in the T group were on hormone replacement therapy. One participant from the T group was not included in any analyses as we were unable to obtain reliable measures of Q; maximal Q values of two participants from the T group were also eliminated as two reliable measures could not be obtained. The correlation between the two Q measures for the remaining T and UT was 0.87 (CI: 1.00) at maximal exercise and 0.69 (CI: 0.64) at SM exercise. In the T group, 4 participants had run or were training for half and full marathons, 4 were training for 5-10K races and one was a master athlete speed walker; participants were training 4-6 days per week for durations of 45-90 minutes per session. Sample characteristics are presented in Table 1. Age, weight, BMI and resting heart rate were significantly different between groups. No differences were observed for Q L·min-1 or SV ml·beat-1 at rest. VO2max ml·kg-1·min-1 of the T group (37.5 ml·kg-1·min- 1) was 55.6% greater than in the UT group (24.1 ml·kg-1·min-1, p < 0.05). The greater VO2max of the T group was accompanied by a 30.6% greater Qmax (T: 19.2 ± 1.0, UT: 14.7 ± 1.0, p < 0.05) and 26.1% greater SVmax (T: 119.3 ± 6.3, UT: 94.6 ± 7.0, p < 0.05). Maximal exercise HR (T: 160.9 ± 3.2, UT: 156.1 ± 3.2, p > 0.05) and (a-v)O2diff (T: 11.9 ± 0.6, UT: 11.3 ± 0.8, p > 0.05) did not differ between groups. Data for maximal exercise Q, SV, HR and (a-v)O2diff versus VO2 are shown in Figure 1. Maximal power output was significantly higher in the T (182 ± 3 W) compared to UT (115 ± 6 W, p < 0.001).
Table 1.
Sample characteristics for trained and untrained women. Data are means (±SE).
| Trained (n= 7) | Untrained (n= 10) | |
|---|---|---|
| Age (years) | 62.7 (1.2) | 68.8 (2.0) * |
| Weight (kg) | 59.8 (3.5) | 66.8 (1.7) |
| Height (m) | 1.60 (.03) | 1.60 (.02) |
| BMI (kg·m-2) | 22.5 (.9) | 26.2 (.8) * |
| SBP (mmHg) | 129.4 (5.6) | 131.7 (3.4) |
| DBP (mmHg) | 72.4 (2.6) | 69.6 (2.3) |
| Resting Q (L·min-1) | 4.3 (.2) | 4.6 (.2) |
| Resting SV (ml beat-1) | 62.4 (4.5) | 60.6 (3.3) |
| Resting HR (bpm) | 62 (4) | 72 (4) |
| VO2max (L·min-1) | 2.26 (.06) | 1.61 (.07) * |
| VO2submax (L·min-1) | 1.30 (.05) | 1.09 (.04) * |
BMI: Body Mass Index; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure, Q: Cardiac Output; SV: Stroke Volume; HR: Heart Rate; VO2max: Maximal Oxygen consumption; VO2submax: Submaximal Oxygen Consumption.
* p < 0.05
Figure 1.
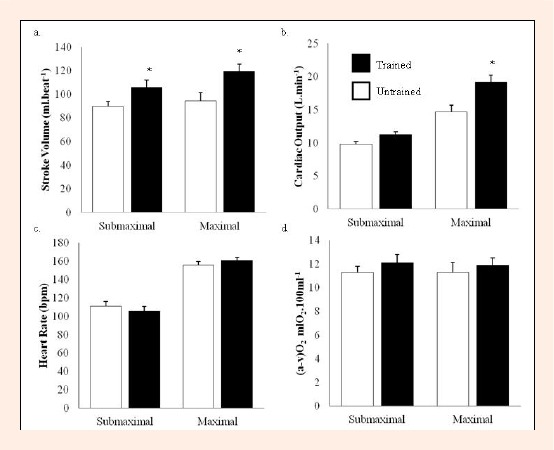
Measures of maximal and submaximal Q, SV, HR and (a-v)O2diff in trained and untrained participants by VO2. * p < 0.05 between groups
Figure 1 also shows data for SM exercise. The SM exercise SV was significantly higher in the T (105.7 ± 6.4) versus UT (89.7 ± 4.3, p = 0.046). The SM exercise power output differed significantly between the T (52 ± 2 W) and UT (40 ± 0 W, p < 0.001), however, these work rates elicited similar SM exercise HR, indicating similar relative intensities of exercise.
Within groups, HR and Q increased significantly from baseline to SM and maximal exercise as well as from SM to maximal exercise. For SV, the UT and T group had significant increases from baseline to SM (T: 69.4%, p = 0.003; UT: 48.0 %, p < 0.001) and maximal exercise (T: 91.2%, p < 0.001; UT: 56.1%, p < 0.001). From SM to maximal exercise, SV increased by 12.9% (p = 0.26) in the T and 5.5% (p = 0.32) in the UT; these were not significant increases. The regression between SV and VO2 indicated a slope of 16.2 ± 12.1 ml increase of SV per L·min-1 of VO2 in the T and 0.5 ± 12.5 in the UT; neither were significantly different from zero. An approximate 20% increase from SM to maximal was observed in 4 of the 7 T and only 2 of the 10 UT; the remaining either stayed the same or decreased.
Discussion
TThis study assessed differences in central and peripheral components of VO2max between older endurance trained and recreationally active women. Our primary finding is that T women have significantly higher Q and SV during maximal exercise, exclusively explaining the higher cardiorespiratory fitness observed in this group. The corollary, contrary to our hypothesis, is that there were no differences between groups for (a-v)O2diff at SM or maximal exercise. A secondary finding is that SV does not increase (significantly) from SM to maximal exercise in both UT and T older women; however, given the small participant numbers it is possible that SV might increase in the T.
An early study by Ogawa et al., 1992 assessed both VO2max and Qmax in 14 untrained (age 64 ± 4) and 13 endurance trained (age 57 ± 3) women during maximal treadmill exercise and attributed the greater VO2max in the endurance trained to a higher SV (85 vs. 74 ml·beat-1) and also a widened (a-v)O2diff (14.5 vs. 11.9 ml·100ml-1). Later, McCole et al., 2000 found that among sedentary (age 63 ± 5) and trained (age 64 ± 4) postmenopausal women, SV was primarily responsible for differences between VO2max. The findings of our study corroborate those of McCole et al., 2000. Using a treadmill protocol and acetylene rebreathing, McCole et al., 2000 found that trained women had a SVmax 40% higher than their age-matched sedentary peers. Our study was able to confirm this difference using a cycle ergometer protocol and the open-circuit acetylene wash-in techniques. Further, in both studies the difference in VO2max in the endurance trained versus untrained older women was attributable to the higher Q and SV with no between group differences in the maximal (a-v)O2diff . This is quite different from the recently confirmed findings of exercise training studies of older women in which the "short-term" gain in VO2max with training is accounted for by a widened maximal (a-v)O2diff with little improvement in SV (Murias et al., 2010a; 2010b; Spina, 1999).
Although the present study and that of McCole et al., 2000 concur in the comparison of the cardiovascular responses to exercise in the endurance trained versus untrained older women, the absolute values for maximal exercise Q and exercise SV differ considerably. The exercise Q to VO2 relationship is generally described as having a slope of 5 (to 6) L·min-1 with an intercept of 5 L·min-1 (i.e., Q (L·min- 1) = 5 (or 5.5) VO2 (L·min-1) + 5) (as reviewed by Proctor et al., 1998). Based on this relationship maximal Q values in the present study (T: Q 19.2 ± 1.0 L·min-1 at VO2 2.26 ± 0.06 L·min-1; UT: Q 14.7 ± 1.0 L·min-1 at VO2 1.61 ± 0.07 L·min-1) appear to be ~18% high for the T and ~5% high for UT; on the other hand the maximal data for McCole et al., 2000 are lower by ~15% in endurance trained and 20% in the sedentary group. For submaximal Q values, however, the present data were in close accord with the regression estimates (within 0.5 L·min- 1), with a SV of 106 mL·beat-1 in T and 90 mL·beat-1 in UT compared to values of 90 mL·beat-1 and 60 mL.beat-1, respectively per group by McCole et al., 1999. Thus, while differences between trained and untrained older women are confirmed, the expected SV of older women ranges from a low value of ~60 mL·beat-1 to ~90 mL·beat-1, and in the trained groups from 80 mL.beat-1 to 105 mL·beat-1. Proctor et al., 1998 in endurance trained older women, using the acetylene rebreathe, reported SV in the range of 80 mL·beat-1. These differences in absolute values for Q and SV could be related to participant characteristics; however, the age, endurance training history and VO2max of the groups in our study, McCole et al., 2000 and Proctor et al., 1998 are very similar. Differences in exercise mode as the reason is also unlikely as, if anything, a higher Q-VO2 and SV would be expected for treadmill (study of McCole et al., 2000) versus cycle (present study and Proctor et al., 1998). Differences may be due to use of the acetylene rebreathe (McCole et al., 2000; Proctor et al., 1998) versus open-circuit (present study) methods; however it is not known whether there are systematic differences between these methods, or the data simply reflects a variability in measurement using these indirect gas techniques. Our study of training in older women (Murias et al., 2010a) reported Q values close to those of the Q-VO2 regression equation with a SV of 106 mL·beat-1 pre-training and 110 mL·beat-1 after 12-weeks of training. Thus, while cross-sectional studies consistently show that endurance training is associated with higher central parameters in older women, this is not the case with longitudinal (intervention) type studies (Katyal et al., 2003; Murias et al., 2010a). This discrepancy may be related to differences in training modes (cross-training between running, cycling and swimming etc.) and lifelong participation in training (years of training versus short-term training of 3-6 months) in cross-sectional analyses.
In comparisons of young and older endurance trained women, it has generally been noted that young women have a higher VO2max and Qmax (Proctor et al., 1998; Wiebe et al., 1999). Wiebe et al., 1999 compared endurance trained young (age 22.4 ± 1.4) to older women using three different age groups (age 42.7 ± 0.6, 50.8 ± 0.8, 60.3 ± 1.2) for comparison of VO2max and its components. The young group had a VO2max of 63.7 ± 2.3 ml·kg-1·min-1 compared to 51.0 3.1 and 47.0 ± 2.5 ml.kg-1.min-1 in the two middle-aged groups and 44.2 ± 1.7 ml·kg-1·min-1 in the oldest group. SVmax was highest in the younger group (125 ± 5) compared to the other three groups (109 ± 6, 107 ± 6, 104 ± 7); however, there were no differences between any of the older groups. In other words, endurance activity was associated with preserved SV from middle-age to older age. Taken together with findings of Eskurza et al., 2002 that decreases in VO2max of endurance trained women are primarily related to decreases in physical activity volume as well as findings from Katyal et al., 2003 and Murias et al., 2010a that improved VO2max from short-term training in older women is not associated with changes in central parameters, it is possible that older women might preserve their maximal Q and SV with high volumes of endurance training as was observed in the T group of the present study. It is also possible that higher maximal Q and SV among trained women are related to lifelong exercise participation. Studies have shown that older adults are unable to improve central parameters with training or have lower levels of Q when compared to master athletes and younger adults respectively (Donal et al., 2011; Fujimoto et al., 2010). Finally, differences in these central parameters, as well as exercise levels, may relate to genetic differences between groups (Bouchard and Rankinen, 2001).
We also found that SV did not increase from SM to maximal exercise in either the T or UT group. Past studies have indicated a failure to maintain SV beyond moderate-intensity aerobic exercise in older adults (McCole et al., 1999, Thomas et al., 1993). McCole et al., 1999 used a treadmill testing protocol which offers an advantage to the trained groups which were primarily composed of runners; the specificity of the mode would allow for the women to achieve a true maximum. However, this study did not find any increase in SV after 60% of VO2max. Data from endurance trained young males and females have shown that SV may continue to increase until maximal exercise, at least in some participants; primarily due to ventricular filling (related to better diastolic filling) and left ventricular ejection (Ferguson et al., 2001; Gledhill et al., 1994). It therefore seems that endurance trained individuals may have better ventricular contractility and end-diastolic pressures leading to higher SV even at higher heart rates. In the present study the T group had an increase in SV from 105.7 to 119.3 ml (12.9% increase) while SV in the UT group increased from 89.7 to 94.6 ml (5.5% increase, p > 0.05 between groups). Further, 4 T and only 2 UT had a ~20% increase from SM to maximal exercise. According to a review conducted by Rowland, 2009, this continued increase of 20% in SV from SM to maximal exercise has been observed in 8 of 21 studies. The commonality in these studies was that 6 of the 8 were conducted using acetylene rebreathe and 5 of the 8 were conducted using a supramaximal protocol (wherein a supramaximal bout of exercise is conducted after a short rest period). The conclusion drawn from the review of the 21 papers was that current evidence pertaining to increasing SV in endurance trained is inconclusive. There is evidence of a central limitation to VO2max (González-Alonso, 2008), however, Warburton and Gledhill, 2008 pointed out that this is not generally the case in endurance trained as they are able to increase SV throughout exercise to maximal levels. Our study did not find statistical increases from SM to maximal exercise in either group; however, there is some support for the notion that SV does not plateau at SM exercise in all endurance trained older adults, even among women over the age of 60. We too used a protocol in which the participants had a rest following maximal exercise prior to a workrate (although not supramaximal) designed to rapidly elicit maximal responses. Our study used acetylene, but was a wash-in method not a rebreathe, as were the bulk of previous studies. Nevertheless, as alluded to earlier, in our study the maximal Q seemed higher than one would predict (whereas the submaximal values were not) and thus this trend toward increases of SV with maximal exercise in the older trained group is questioned. Indeed, current evidence pertaining to whether endurance trained older adults might increase SV throughout exercise remains inconclusive.
The absence of between-group differences observed in maximal and SM (a-v)O2diff is similar to findings of other studies (Fujimoto et al., 2010; Wiebe et al., 1999). Nevertheless, based on data from Ogawa et al., 1992 and Murias et al., 2010a, increases in (a-v)O2diff would be expected. This discrepancy may be related to different training volumes or length of participation in training programs or perhaps to the diminished ability for older women to increase muscle mass and thus (a-v)O2diff .
Limitations
The T group was significantly younger than the UT group, although the mean difference was only 6 years and all women were postmenopausal. To ensure that the differences observed in SVmax were not related to age, a post-hoc linear regression analysis using SVmax as the outcome and age and the main exposure was conducted. When controlling for VO2max (p = 0. 98) or group (p = 0.76), there was no significant association between age and SVmax. Further, we did not collect data on lean muscle mass or body fat %. This would have allowed for further speculation on the lack of differences for (a-v)O2diff between groups. Another limitation of the study is the small number of older trained women. While there was sufficient power to detect differences for the main research question, a larger sample would have allowed for more robust results pertaining to the SV plateau. Finally, our (a-v)O2diff values were lower than expected in both groups. As these were calculated using Q and VO2, the (a-v)O2diff is only as reliable as these values. Both VO2 and Q were collected using highly reliable and validated techniques, and all data were collected by competent and trained researchers.
Conclusion
In conclusion, older women who are endurance trained have a higher Q and SV at both SM and maximal exercise; therefore, it seems that older T women are able to preserve central parameters of VO2max. Further, in the T, SV did not rise significantly between submaximal and maximal exercise, in contrast to trained groups of younger adults wherein a continued increase in SV from moderate through heavy exercise has been witnessed; however there was a trend toward a SM to maximum SV increase and perhaps a characteristic of some of the T participants. Future research using large samples of older endurance trained women should be conducted to determine if there are specific characteristics that are associated with continued increases in SV from submaximal to maximal intensity aerobic exercise.
Acknowledgements
This study was supported by Natural Sciences and Engineering Research Council of Canada (NSERC).
Biographies

Shilpa Dogra
Employment
Assistant Professor, Acadia University.
Degree
PhD
Research interests
Exercise and aging, chronic disease epidemiology
E-mail: shilpa.dogra@acadiau.ca

Matthew D. Spencer
Employment
Post-Doctoral Research Fellow, Canadian Centre for Activity and Aging, School of Kinesiology, University of Western Ontario
Degree
PhD
Research interests
Cardiovascular and pulmonary responses to exercise.
E-mail: mspenc25@uwo.ca

Donald H. Paterson
Employment
Professor, Canadian Centre for Activity and Aging, School of Kinesiology, University of Western Ontario
Degree
PhD
Research interests
Exercise physiology, cardiovascular; exercise and aging.
E-mail: dpaterso@uwo.ca
References
- Babcock M.A., Paterson D.H., Cunningham D.A.(1994) Effects of aerobic endurance training on gas exchange kinetics of older men. Medicine and Science in Sports and Exercise 26, 447-452 [PubMed] [Google Scholar]
- Barker R.C, Hopkins S.R., Kellogg N., Olfert I.M., Brutsaert T.D., Gavin T.P., Entin P.L., Rice A.J., Wagner P.D.(1999) Measurement of cardiac output during exercise by open-circuit acetylene uptake. Journal of Applied Physiology 887, 1506-1512 [DOI] [PubMed] [Google Scholar]
- Beaver W.L., Lamarra N., Wasserman K.(1981) Breath-by-breath measurement of true alveolar gas exchange. Journal of Applied Physiology 51, 1662-1675 [DOI] [PubMed] [Google Scholar]
- Beaver W.L., Wasserman K., Whipp B.J.(1986) A new method for detecting anaerobic threshold by gas exchange. Journal of Applied Physiology 60, 2020-2027 [DOI] [PubMed] [Google Scholar]
- Bouchard C., Rankinen T.(2001) Individual differences in response to regular physical activity. Medicine and Science in Sports and Exercise 33, S446-541 [DOI] [PubMed] [Google Scholar]
- Dibski D.W., Smith D.J., Jensen R., Norris S.R., Ford G.T.(2005) Comparison and reliability of two non-invasive acetylene uptake techniques for the measurement of cardiac output. European Journal of Applied Physiology 994, 670-680 [DOI] [PubMed] [Google Scholar]
- Donal E., Rozoy T., Kervio G., Schnell F., Mabo P., Carré F.(2011) Comparison of the heart function adaptation in trained and sedentary men after 50 and before 35 years of age. American Journal of Cardiology 1108, 1029-1037 [DOI] [PubMed] [Google Scholar]
- Eskurza I., Donato A.J., Moreau K., Seals D.R., Tanaka H.(2002) Changes in maximal aerobic capacity with age in endurance-trained women: 7-yr follow-up. Journal of Applied Physiology 92, 2303-2308 [DOI] [PubMed] [Google Scholar]
- Fujimoto N., Prasad A., Hastings J.L., Arbab-Zadeh A., Bhella P.S., Shibata S., Palmer D., Levine B.D.(2010) Cardiovascular effects of 1 year of progressive and vigorous exercise training in previously sedentary individuals older than 65 years of age. Circulation 1122, 1797-1805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gledhill N., Cox D., Jamnik R.(1994) Endurance athletes’ stroke volume does not plateau: major advantage is diastolic function. Medicine and Science in Sports and Exercise 26, 1116-1121 [PubMed] [Google Scholar]
- González-Alonso J.(2008) Point: Stroke volume does/does not decline during exercise at maximal effort in healthy individuals. Journal of Applied Physiology 104, 275-276 [DOI] [PubMed] [Google Scholar]
- Johnson B.D., Beck K.C., Proctor D.N., Miller J., Dietz N.M., Joyner M.J.(2000) Cardiac output during exercise by the open circuit acetylene washin method: comparison with direct Fick. Journal of Applied Physiology 88, 1650-1658 [DOI] [PubMed] [Google Scholar]
- Katyal S., Freeman M., Miller J.A., Thomas S.G.(2003) Short-term aerobic training and circulatory function in women: age and hormone-replacement therapy. Clinical Science (Lond) 104, 267-273 [DOI] [PubMed] [Google Scholar]
- Kemi O.J., Haram P.M., Loennechen J.P., Osnes J.B., Skomedal T., Wisl⊘ff U., Ellingsen Ø.(2005) Moderate vs. high exercise intensity: differential effects on aerobic fitness, cardiomyocyte contractility, and endothelial function. Cardiovascular Research 67, 161-172 [DOI] [PubMed] [Google Scholar]
- McCole S.D., Brown M.D., Moore G.E., Zmuda J.M., Cwynar J.D., Hagberg J.M.(2000) Enhanced cardiovascular hemodynamics in endurance-trained postmenopausal women athletes. Medicine and Science in Sports and Exercise 32, 1073-1079 [DOI] [PubMed] [Google Scholar]
- McCole S.D., Brown M.D., Moore G.E., Zmuda J.M., Cwynar J.D., Hagberg J.M.(1999) Cardiovascular hemodynamics with increasing exercise intensities in postmenopausal women. Journal of Applied Physiology 887, 2334-40 [DOI] [PubMed] [Google Scholar]
- Murias J.M., Kowalchuk J.M., Paterson D.H.(2010a) Mechanisms for increases in VO2max with endurance training in older and young women. Medicine and Science in Sports and Exercise 42, 1891-1898 [DOI] [PubMed] [Google Scholar]
- Murias J.M., Kowalchuk J.M., Paterson D.H.(2010b) Time course and mechanisms of adaptations in cardiorespiratory fitness with endurance training in older and young men. Journal of Applied Physiology 1108, 621-627 [DOI] [PubMed] [Google Scholar]
- Ogawa T., Spina R.J., Martin W.H., 3rd, Kohrt W.M., Schechtman K.B., Holloszy J.O., Ehsani A.A.(1992) Effects of aging, sex, and physical training on cardiovascular responses to exercise. Circulation 86, 494-503 [DOI] [PubMed] [Google Scholar]
- Paterson D.H., Cunningham D.A.(1999) The gas transporting systems: limits and modifications with age and training. Canadian Journal of Applied Physiology 24, 28-40 [DOI] [PubMed] [Google Scholar]
- Paterson D.H., Warburton D.E.(2010) Physical activity and functional limitations in older adults: a systematic review related to Canada’s Physical Activity Guidelines. International Journal of Behavioral Nutrition and Physical Activity 11, 7-38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferguson S., Gledhill N., Jamnik V.K., Wiebe C., Payne N.(2001) Cardiac performance in endurance-trained and moderately active young women. Medicine and Science in Sports and Exercise 333, 1114-1119 [DOI] [PubMed] [Google Scholar]
- Proctor D.N., Beck K.C., Shen P.H., Eickhoff T.J., Halliwill J.R., Joyner M.J.(1998) Influence of age and gender on cardiac output-VO2 relationships during submaximal cycle ergometry. Journal of Applied Physiology 84, 599-605 [DOI] [PubMed] [Google Scholar]
- Rossiter H.B., Kowalchuk J.M., Whipp B.J.(2006) A test to establish maximum O2 uptake despite no plateau in the O2 uptake response to ramp incremental exercise. Journal of Applied Physiology 100, 764-770 [DOI] [PubMed] [Google Scholar]
- Rowland T.(2009) Endurance athletes’ stroke volume response to progressive exercise: a critical review. Sports Medicine 39, 687-695 [DOI] [PubMed] [Google Scholar]
- Spina R.J.(1999) Cardiovascular adaptations to endurance exercise training in older men and women. Exercise and Sport Science Reviews 27, 317-332 [PubMed] [Google Scholar]
- Stachenfeld N.S., Mack G.W., DiPietro L., Morocco T.S., Jozsi A.C., Nadel E.R.(1998) Regulation of blood volume during training in post-menopausal women. Medicine and Science in Sports and Exercise 30, 92-98 [DOI] [PubMed] [Google Scholar]
- Stevenson E.T., Davy K.P., Seals D.R.(1994) Maximal aerobic capacity and total blood volume in highly trained middle-aged and older female endurance athletes. Journal of Applied Physiology 777, 1691-1696 [DOI] [PubMed] [Google Scholar]
- Swain D.P., Franklin B.A.(2006) Comparison of cardioprotective benefits of vigorous versus moderate intensity aerobic exercise. American Journal of Cardiology 997, 141-147 [DOI] [PubMed] [Google Scholar]
- Thomas S.G., Paterson D.H., Cunningham D.A., McLellan D.G., Kostuk W.J.(1993) Cardiac output and left ventricular function in response to exercise in older men. Canadian Journal of Physiology and Pharmacology 71, 136-144 [DOI] [PubMed] [Google Scholar]
- Warburton D.E., Gledhill N.(2008) Counterpoint: Stroke volume does not decline during exercise at maximal effort in healthy individuals. Journal of Applied Physiology 104, 276-278 [DOI] [PubMed] [Google Scholar]
- Whipp B.J., Ward S.A., Wasserman K.(1986) Respiratory markers of the anaerobic threshold. Advances in Cardiology 35, 47-64 [DOI] [PubMed] [Google Scholar]
- Wiebe C.G., Gledhill N., Jamnik V.K., Ferguson S.(1999) Exercise cardiac function in young through elderly endurance trained women. Medicine and Science in Sports and Exercise 31, 684-691 [DOI] [PubMed] [Google Scholar]