

Abstract
The purpose of the study was to assess the effects of sodium citrate ingestion on the metabolic response to exercise and performance in a 1500-m competitive run in trained female middle-distance runners in field conditions. Seventeen athletes (mean (± SD) aged 18.6 ± 2.5 years, VO2max 55.2 ± 7.6 ml·kg-1·min-1) competed in two 1500-m races following ingestion of 0.4 g·kg-1 body mass of sodium citrate (CIT) and placebo (PLC - 1.0% solution of NaCl). The two substances, CIT and PLC were administered in 800 ml of solution in a randomly assigned double-blind crossover manner. Capillary blood samples were analysed for lactate, glucose, haemoglobin and haematocrit before administering the solutions (baseline) as well as before and after both 1500-m races. The athletes’ times for trials CIT and PLC were 321.4 ± 26.4 and 317.4 ± 22.5 s, respectively (p > 0.05). A greater relative increase in plasma volume after administering the experimental solution, an increased body mass (by 0.4 kg; p = 0.006) immediately before the race and a restrained increase in blood glucose concentration (by 2.5 ± 1.2 mmol·l-1 vs 3.4 ± 0.8 mmol·l-1; p = 0.002) during the race were observed in the CIT trial compared to the PLC. A significant relationship was observed between body mass of the subjects immediately before the race and performance time (r = 0.374; p = 0.029). There were no between-treatment differences in heart rate in any stage of the run or in blood lactate accumulation during the race (final concentration of lactate was 14.4 ± 3.0 mmol·l-1 and 13.4 ± 2.5 mmol·l-1 (p > 0.05) in the CIT and PLC trials, respectively). The results suggest that sodium citrate induces an increase in water retention before exercise and may modify carbohydrate metabolism in high intensity running, but does not improve performance in 1500-m competitive run in female middle-distance runners.
Key points.
Previous studies have found that sodium bicarbonate administration may enhance performance in male athletes in running distances of 400-1500 m.
The use of sodium bicarbonate in competitive sports is limited because it induces gastrointestinal distress in many subjects.
The limited data on the effects of sodium citrate ingestion on the metabolic response to exercise and performance suggest that it may have all the benefits of sodium bicarbonate without the associated negative side effects.
We assessed the effects of sodium citrate ingestion on the metabolic response to exercise and performance in a 1500-m competitive run in trained young female middle-distance runners.
The results suggest that sodium citrate induces an increase in water retention before exercise and may modify carbohydrate metabolism in high intensity running, but does not improve performance in 1500-m competitive run in female middle-distance runners.
Key words: Middle-distance running, buffer ingestion, ergogenic aid
Introduction
High-intensity exercise is associated with the accumulation of lactate and hydrogen ions (H+) within active muscle and blood. Although recent findings of Pedersen and co-workers (2004) question the involvement of H+ in muscle fatigue, a decrease in pH has been shown to contribute to decrease in muscle function through inhibition of the glycolytic enzymes (Sutton et al., 1981), calcium release from the sarcoplasmic reticulum and its binding to troponin C (Fuchs et al., 1969) and interaction between myosin and actin (Chase and Kushmeric, 1988). Ingestion of sodium bicarbonate or sodium citrate has been shown to increase blood pH and HCO3- concentration (Potteiger et al., 1996). The monocarboxylate transporter, which is considered to be responsible for lactate and H+ transport across the cell membrane (Roth, 1991) is sensitive to a pH gradient (Roth and Brooks, 1990). Thus, ingestion of alkalinizing agents mentioned above by increasing the extracellular pH may create a favourable pH gradient for efflux of intracellular lactate and H+ from contracting muscle cells. This, in turn, may delay the decrease in intramuscular pH to the critical level at which detrimental effects on muscle performance occur during intense exercise.
Numerous studies have assessed the effect of pre-exercise administration of alkalinizing agents on performance in different types of exercise (Burke et al., 2006; Requena et al., 2005). The general conclusion of the reviewers is that the ingestion of sodium bicarbonate or sodium citrate appears to enhance performance in a single bout of maximal intensity exercise of approximately 1-7 min duration. However, this conclusion is mainly based on the results of studies in which sodium bicarbonate has been used. Although ingestion of sodium bicarbonate has potential to enhance performance in high intensity exercise, its use in competitive sports is limited because it induces gastrointestinal distress in many subjects (Requena et al., 2005). The limited data on the effects of sodium citrate ingestion on the metabolic response to exercise and performance suggest that it may have all the benefits of sodium bicarbonate without the associated negative side effects (McNaughton, 1990). On the other hand, research conducted in male runners has shown that a dose of sodium citrate that is sufficient for inducing an alkalotic state and that is ingested with water also induces an increase in both plasma volume and body mass (Ööpik et al., 2003; 2004). Additional workload caused by increased body mass may counterbalance the positive effect of sodium citrate on running performance.
Both intra- and extracellular buffer systems are involved in the regulation of intracellular pH. Available data suggest that muscle buffer capacity is about 20% lower in females than in males (Edge et al., 2006). Consequently, female athletes increasing the limited buffer capacity of their body through pre-exercise ingestion of alkalinizers could be expected to benefit in respect of performance in high-intensity exercise even more than males. However, the possible acute effect of sodium citrate ingestion on plasma volume or body mass has not been assessed in females.
Female subjects have been studied on very few occasions so far (Bishop and Claudius, 2005; Kozak-Collins et al., 1994; McNaughton et al., 1997; Tiryaki and Atterbom, 1995) and the data concerning the effect of ingestion of alkalinizers on performance in female athletes are inconsistent. To the best of our knowledge the study conducted by Tiryaki and Atterbom, 1995 is the only one where female middle-distance runners administering sodium citrate have been investigated in field conditions. Pre-exercise ingestion of sodium bicarbonate or sodium citrate failed to affect 600-m running performance. The results of other studies have revealed that sodium bicarbonate administration may enhance performance in male athletes in running distances of 400-1500 m (Bird et al., 1995; Goldfinch et al., 1988; Wilkes et al., 1983).
Hence, the true effect of sodium citrate on the metabolic response to exercise and performance in female middle-distance runners in competitive situation remains unclear. Therefore, the purpose of the present study was to assess the effects of sodium citrate ingestion on the metabolic response to exercise and performance in a 1500-m competitive run in trained young female middle-distance runners.
Methods
Subjects
Seventeen female middle-distance runners gave their written informed consent for participation in the study, the protocol of which was approved by the university’s Ethics Committee. Where subjects were under 18 years of age, the written informed consent was also obtained from the parents. At the beginning of the study the mean (± SD) age, body mass, height, and maximal oxygen uptake (VO2max) of the subjects were 18.6 ± 2.5 years, 56.2 ± 5.3 kg, 1.68 ± 0.04 m and 55.2 ± 7.6 ml·kg-1·min-1, respectively. They had been involved in running training for 5.5 ± 2.0 years. They trained regularly 5-6 times a week 1.5-2 hours each time. All subjects competed regularly in middle-distance races at club to national level competitions.
Study protocol
All subjects were tested four times in a 3-hour postabsorptive state. The first occasion was to determine VO2max in laboratory conditions, and the other three were to undertake a 1500-m run in an indoor banked 150-m oval running track. The runners were instructed to abstain from vigorous exercise the day before each test, and were requested to follow their habitual eating pattern throughout the study period. On each test day and the day preceding the visit to the laboratory, the subjects kept detailed physical activity and food diaries, in which they recorded all food and drink intake. In order to ensure the weight of food consumed was recorded correctly, each participant was provided with a weighing scale and a questionnaire to record the type and quantity of food eaten. A dietary analysis was performed using the Micro-Nutrica 2.0 software. The information obtained from the diaries completed before the first visit to the laboratory was used to remind the athletes of the pattern of physical activity and eating to follow before each subsequent test day. These measures were undertaken in order to ensure stable nutritional and training status of the subjects throughout the study period.
The maximal oxygen uptake of the subjects was measured during a progressive exercise test performed on a treadmill (Runrace HC 1400, Technogym, Gambettola, Italy). After a 5-min warm-up at a speed of 8 km·h-1, the starting speed was set at 10 km·h-1. The speed of movement was increased every 3 min by 2 km·h-1 until reaching 14 km·h-1, after which it was raised by 1 km·h-1 every 3 min until the runners could no longer maintain the pace. Expired gas was sampled and analyzed continuously using an online system (True Max 2400, Parvo Medics, East Sandy, Utah, USA). The analyzer was calibrated with standard gas mixture containing 16.0% of O2 and 4.0% of CO2 before each subject was tested. The main criteria used to confirm that VO2max had been reached was the achievement of plateau in O2 uptake with an increase in workrate (Davis, 2006). In case of difficulties in identifying a true plateau in VO2 before cessation of the test the achievement of VO2max was accepted if the respiratory exchange ratio at test termination exceeded 1.00 and the heart rate was over 90% of age-predicted maximum (Davis, 2006).
Each athlete participated in three 1500-m races. The races took place over three consecutive weeks. The first race was performed in order to accustom the subjects to the research procedures and to assess their current performance capacity in the distance of 1500 m. The two conditions, sodium citrate (CIT) and placebo (PLC) were administered thereafter in a randomly assigned double-blind crossover manner.
In the CIT trial, the subjects ingested 400 ml of fluid containing sodium citrate (0.4 g·kg-1 body mass). The latter was dissolved in 200 ml of mineral water with low mineral content and mixed with 200 ml of orange juice. In the PLC trial, 400 ml of solution containing 1.0% of sodium chloride was used in the same mineral water and orange juice mix. The procedure of administration the solutions in the CIT and PLC trials was the same: half of the volume (200 ml) was consumed two hours and the other half 1.5 hours before the test run. Immediately following ingestion of each portion of the solution, the subjects were encouraged to drink 200 ml of mineral water, in order to wash the taste of the solution from their mouths and minimize the likelihood of gastrointestinal disorders. The total amount of fluid ingested before the race was 800 ml. The subjects were asked to report to the researchers about any gastrointestinal distress experienced during the trials. Body mass was measured just before administering the solution, immediately before starting the run, and after finishing. The subjects were allowed to use the toilet between the first and the second body mass measurement. They did not consume any food or beverages after drinking the treatment solution throughout the testing procedure in each trial. They performed their customary prerace warm-up before the race.
In order to create a real competitive situation during the run, the subjects were pair-matched according to their results in the control trial. During the race they were continuously encouraged to run as fast as they could. Heart rate was recorded during the race using cardiotester Polar PE 3000 (Polar Electro OY, Finland). All races took place in the late afternoon (18:00 - 20:00).
Biochemical analyses
Capillary blood samples were taken from the fingertip of the subjects. Participants were seated for at least 5 min prior to the procedure. The first sample was taken before administering the solutions (baseline), the second before each test run (after the standardized warm-up), and the third sample was obtained five minutes after the end of the 1500-m run.
The concentrations of lactate and glucose in blood samples were measured enzymatically (Dr Lange Cuvette Test LKM 140 and LKM 141, respectively) using miniphotometer LP 20 Plus (Dr Lange, Germany). The capillary blood samples were also used for the measurement of haemoglobin concentration (cyanmethemoglobin method, Dr Lange Cuvette Test LKM 143) and packed cell volume (by spun haematocrit). The values obtained were used to calculate changes in plasma and blood volume (Dill and Costill, 1974).
Statistical analysis
The distribution pattern of the data was tested using the one-sample Kolmogorov-Smirnov test. A one-way analysis of variance for repeated measures was applied to identify differences between CIT and PLC treatments. The dependent t-test was used to locate differences between the means. Significance was set at p < 0.05. The Pearson product- moment correlation coefficients were computed to determine the relationship between variables. The SPSS 10.0 for Windows software was used for performing statistical analysis.
Results
There were no differences in energy and nutrient intake by the subjects during the day preceding the test or in the test day in any treatment conditions (Table 1).
Table 1.
Quantities of protein, fat, carbohydrate and water consumed by the subjects during the preceding and the test day. Data are means (SD).
| Day | Control | Treatment Placebo | Sodium citrate | |
|---|---|---|---|---|
| The preceding day | Energy (kcal·day−1) | 1966 (535) | 1685 (584) | 1869 (560) |
| Protein (g·day−1) | 69.9 (19.8) | 57.1 (28.5) | 72.1 (25.3) | |
| Fat (g·day−1) | 65.5 (37.4) | 51.7 (21.8) | 61.8 (28.9) | |
| Carbohydrate (g·day−1) | 267.6 (125.3) | 242.2 (106.9) | 249.9 (86.8) | |
| Water (g·day−1) | 1829 (899) | 1866 (1235) | 1729 (742) | |
| Test day | Energy (kcal·day−1) | 1403 (695) | 1124 (504) | 1318 (662) |
| Protein (g·day−1) | 44.4 (25.4) | 40.8 (23.1) | 42.1 (25.8) | |
| Fat (g·day−1) | 44.3 (28.3) | 35.2 (24.2) | 39.3 (20.5) | |
| Carbohydrate (g·day−1) | 201.8 (118.0) | 157.2 (80.8) | 194.5 (107.0) | |
| Water (g·day−1) | 1053 (630) | 1066 (482) | 1071 (525) |
There was no significant effect of CIT administration on 1500-m running time. It took 321. 4 ± 26.4 s in the CIT trial and 317.4 ± 22.5 s in the PLC trial to complete the run. No difference between treatments was observed in any stage of the run where the split times were measured (Table 2). Seven of the 17 subjects achieved their better result after CIT ingestion, whereas ten were faster in the PLC trial.
Table 2.
Split times (s) and time taken to complete the 1500-m run. Data are means (SD).
| Stage | ||||
|---|---|---|---|---|
| Treatment | 450 m | 900 m | 1200 m | Finish |
| PLC | 92.6 (8.9) | 190.3 (15.3) | 255.9 (19.0) | 317.4 (22.5) |
| CIT | 93.1 (7.7) | 192.5 (16.1) | 258.8 (21.4) | 321.4 (26.4) |
There were no between- treatment differences in heart rate values in any stage of the run. The highest heart rate observed at the finish of the race was 192 ± 9 beats·min-1 in both trials.
There was no between-trial difference in baseline body mass of the subjects (Table 3). Before the start of the test run the runners were heavier in the CIT trial in comparison with the PLC by 0.4 kg (p = 0.006). The difference in body mass was also maintained after the race (by 0.3 kg; p = 0.009). Correlation analysis of the pooled data revealed a significant relationship between body mass of the subjects immediately before the race and performance time (n = 34; r = 0.374; p = 0.029).
Table 3.
Body mass of the subjects. Data are means (SD).
| Treatment | Baseline | Before run | After run |
|---|---|---|---|
| PLC | 56.1 (5.4) | 56.1 (5.4) | 56.0 (5.4) † |
| CIT | 56.1 (5.4) | 56.5 (5.4) * ‡ | 56.3 (5.3) * † ‡ |
Significantly different (p < 0.05):
* from baseline value
† from before run value
‡from PLC treatment.
The calculated relative increase in plasma volume during the period between administering the solution and starting the run in the CIT trial (3.96 ± 4.44%) exceeded the change observed in the PLC trial (-0.55 ± 5.57%; p = 0. 006). The relative decrease in plasma volume during the race did not differ in the two trials (Table 4).
Table 4.
Packed cell volume, haemoglobin concentration, and relative changes in plasma volume. Data are means (SD).
| PLC | CIT | ||
|---|---|---|---|
| Packed cell volume (%) | |||
| Baseline | 38.1 (3.0) | 37.7 (2.6) | |
| Before run | 38.1 (2.9) | 36.8 (2.5) * ‡ | |
| After run | 40.5 (2.6) *† | 39.2 (2.4) * † ‡ | |
| Haemoglobin (g·100 ml−1) | |||
| Baseline | 12.6 (1.3) | 12.8 (1.1) | |
| Before run | 12.7 (1.1) | 12.5 (1.2) * | |
| After run | 13.2 (1.2) *† | 13.0 (1.2) * † | |
| Changes in plasma volume (%) | |||
| Baseline → before run | − 0.55 (5.57) | 3.96 (4.44) ‡ | |
| Before run → after run | −7.73 (3.90) | −7.58 (4.78) |
Significantly different (p < 0.05):
* from baseline value
† from before-run value
‡ from PLC treatment.
There were no differences in blood lactate concentration between the trials prior to administering the solutions or before the race (Figure 1). An increase in the blood lactate level was observed as a result of the 1500-m run in both trials The concentration of lactate in blood measured 5 min after finishing the race was 14.4 ± 3.0 mmol·l-1 and 13.4 ± 2.5 mmol·l-1 (p > 0.05) in the CIT and PLC trials, respectively.
Figure 1.
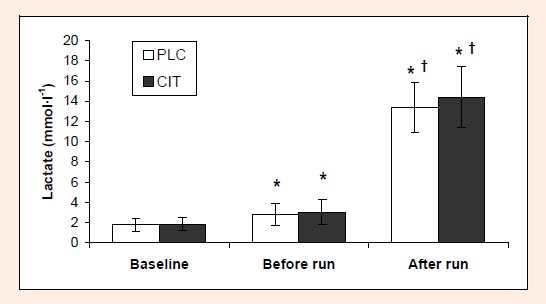
Blood lactate concentration under different treatments (mean ± SD). Significantly different (p < 0.05): * from baseline value; † from before-run value.
Blood glucose concentrations were similar in baseline and before run conditions in both trials (Figure 2). The race resulted in an increase in blood glucose concentration in both trials. The extent of the increase was lower in the CIT trial (2.5 ± 1.2 mmol·l-1) in comparison with the PLC trial (3.4 ± 0.8 mmol·l-1; p = 0.002). The values of blood lactate and glucose concentrations measured before and after the run are presented as adjusted for the individual changes in blood volume.
Figure 2.
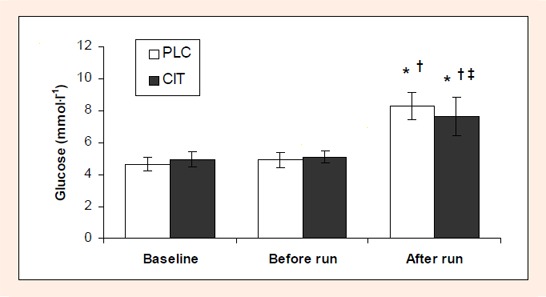
Blood glucose concentration under different treatments (mean ± SD). Significantly different (p 0.05): * from baseline value; † from before-run value; ‡ from the PLC treatment.
Fifteen athletes of seventeen reported mild nausea, stomach cramps, cold shivers or diarrhoea following ingestion of sodium citrate, whereas there were no such complaints in the PLC trial.
Discussion
The main finding of the study was that administration of CIT in comparison with PLC ingestion did not improve performance in 1500-m run in trained young female middle-distance runners. This finding is in agreement with the results of the study conducted by Tiryaki and Atterbom, 1995 who reported no effect of sodium citrate or sodium bicarbonate ingestion in comparison with placebo administration on performance in 600-m run in young female track athletes. Contrary to this, Bird et al., 1995 demonstrated improvement in performance in 1500-m run in male distance runners as a result of sodium bicarbonate ingestion. Similarly, two other placebo-controlled studies have shown that sodium bicarbonate ingestion enhances performance in 400-m (Goldfinch et al., 1988) and 800-m (Wilkes et al., 1983) run in male runners.
Although both sodium bicarbonate and sodium citrate administration resulted in significant shifts in the blood acid-base balance, there was no effect of alkalinizers on blood lactate accumulation and performance in 600-m run in female runners (Tiryaki and Atterbom, 1995). Similarly, there were no differences in blood lactate accumulation and in performance between the CIT and PLC trials in 1500-m run in our female athletes. Since we did not measure the pH or the concentration of bicarbonate in blood, we have no direct evidence that sodium citrate administration induced an alkalotic state in our subjects. On the other hand, Tiryaki and Atterbom, 1995 administered 300 mg·kg-1 of sodium citrate to their subjects and observed significant shifts in blood acid-base balance towards alkalosis. Hence, the dose of sodium citrate used in the present study (400 mg·kg-1) was most likely sufficient for inducing alkalosis.
Tiryaki and Atterbom, 1995 speculated that the apparent lack of the effect of alkalinizers on muscle lactate and H+ kinetics might be explained by the short duration (approximately 120 s) of the effort performed by their subjects. However, on average our subjects ran 2.7 times longer (ca 317-321 s) and still had similar post-exercise blood lactate concentrations in the CIT and PLC trials. Moreover, following sodium bicarbonate ingestion both higher blood lactate concentration as well as improved performance have been observed in female subjects in cycle exercise of only 60 s of duration (McNaughton et al., 1997).
Van Montfoort et al., 2004 found that sodium citrate in comparison with sodium bicarbonate and sodium lactate produced the highest blood pH and bicarbonate concentration but was less effective than the other substances in respect of sprint performance. The lower efficiency of sodium citrate in comparison with sodium bicarbonate in respect of performance would explain the discrepancy between our results and those of Bird et al., 1995. It has been speculated that an increase in intracellular citrate concentration after ingestion of sodium citrate could reduce the generation of ATP through glyco(geno)lysis via inhibition of the enzyme phosphofructokinase (Horswill, 1995). Hence, the positive effect of alkalinization on anaerobic energy production, which is based on the facilitated H+ efflux from intensively contracting muscle cells, may be counterbalanced by an increase in intracellular citrate concentration.
A significantly smaller extent of an increase in blood glucose level during the race in the CIT trial compared with the PLC treatment (Figure 2) confirms previous findings (Ööpik et al., 2004). These differences can not be induced by nutritional factors because the intake of energy and nutrients by the subjects did not differ in the trials (Table 1). Whether the restrained elevation in blood glucose concentration reflects an increase in glucose utilization or a reduction in hepatic glucose release during high intensity exercise after sodium citrate ingestion, remains to be assessed in further studies.
A greater relative increase in plasma volume after administering the experimental solution (Table 4) as well as increased body mass measured immediately before the run (Table 3) reveal greater fluid retention in the pre-exercise period in the CIT trial compared to the PLC. This finding fits well with previous observations in male runners (Ööpik et al., 2004). An increase in body mass as a result of sodium citrate and water co-administration should be considered a factor which may reduce any positive effect that sodium citrate ingestion may have on performance in middle-distance runners.
The potential of sodium citrate to induce gastrointestinal distress should not be underestimated. Although sodium citrate is generally considered as a better tolerable substance compared with sodium bicarbonate (Requena et al., 2005), the data in many studies (Schabort et al., 2000; Shave et al., 2001; Ööpik et al., 2004) reveal that it may cause remarkable negative side effects. In the present study there were only two of 17 athletes who did not feel any discomfort following ingestion of sodium citrate.
Conclusion
In conclusion, the results of the present study suggest that sodium citrate administered in 800 ml of solution in the amount of 400 mg·kg-1 body mass induces an increase in water retention, plasma volume and body mass, restrains an increase in blood glucose concentration during exercise, but does not improve performance in 1500-m competitive run in field conditions in trained female middle-distance runners.
Biographies
Vahur Ööpik
Employment
Professor of Exercise Physiology at the Institute of Exercise Biology and Physiotherapy at the University of Tartu, Estonia.
Degree
PhD
Research interests
Physiology and biochemistry of exercise and sports nutrition.
E-mail: vahur.oopik@ut.ee
Saima Timpmann
Employment
Researcher at the Institute of Exercise Biology and Physiotherapy at the University of Tartu, Estonia.
Degree
MSc
Research interests
Physiology and biochemistry of exercise and sports nutrition.
E-mail: saima.timpmann@ut.ee
Kadri Kadak
Employment
Physiotherapist.
Degree
MSc
Research interests
Sports nutrition.
E-mail: kadrikadak13@hot.ee
Luule Medijainen
Employment
Lecturer at the Institute of Exercise Biology and Physiotherapy at the University of Tartu, Estonia.
Degree
MSc
Research interests
Physiology and biochemistry of exercise and sports nutrition.
E-mail: luule.medijainen@ut.ee
Kalle Karelson
Employment
Senior researcher at the Institute of Exercise Biology and Physiotherapy at the University of Tartu, Estonia.
Degree
PhD
Research interests
Physiology of exercise.
E-mail: kalle.karelson@ut.ee
References
- Armstrong L.E., Costill D.L., Fink W.J. (1985) Influence of diuretic-induced dehydration on competitive running performance. Medicine and Science in Sports and Exercise, 17, 456-461 [DOI] [PubMed] [Google Scholar]
- Bird S.R., Wiles J., Robbins J. (1995) The effect of sodium bicarbonate ingestion on 1500-m racing time. Journal of Sports Sciences 13, 399-403 [DOI] [PubMed] [Google Scholar]
- Bishop D., Claudius B. (2005) Effects of induced metabolic alkalosis on prolonged intermittent-sprint performance. Medicine and Science in Sports and Exercise, 37, 759-767 [DOI] [PubMed] [Google Scholar]
- Burke L., Cort M., Cox G., Crawford R., Desbrow B., Farthing L., Minehan M., Shaw N., Warnes O. (2006) Supplements and sports foods. In: Clinical sports nutrition. Eds: Burke L., Deakin V.3rdeditionSydney: McGraw-Hill; 485-579 [Google Scholar]
- Chase P.B., Kushmerick M. (1988) Effect of pH on the contraction of rabbit fast and slow skeletal muscle fibres. Biophysical Journal, 53, 935-946 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis J.A. (2006) Direct determination of aerobic power. In: Physiological assessment of human fitness. Eds: Maud P.J., Foster C.Champaign, IL: Human Kinetics; 9-18 [Google Scholar]
- Dill D.B., Costill D.L. (1974) Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. Journal of Applied Physiology 37, 247-248 [DOI] [PubMed] [Google Scholar]
- Edge J., Bishop D., Goodman C. (2006) The effects of training intensity on muscle buffer capacity in females. European Journal of Applied Physiology 96, 97-105 [DOI] [PubMed] [Google Scholar]
- Fuchs F., Reddy Y., Briggs F.N. (1969) The interaction of cations with the binding site of troponin. Biochimica et Biophysica Acta 221, 407-409 [DOI] [PubMed] [Google Scholar]
- Goldfinch J., McNaughton L., Davies P. (1988) Induced metabolic alkalosis and its effects on 400 m racing time. European Journal of Applied Physiology 57, 45-48 [DOI] [PubMed] [Google Scholar]
- Horswill C.A. (1995) Effects of bicarbonate, citrate, and phosphate loading on performance. International Journal of Sport Nutrition 5, S111-S119 [DOI] [PubMed] [Google Scholar]
- Kozak-Collins K., Burke E.R., Schoene R.B. (1994) Sodium bicarbonate ingestion does not improve performance in women cyclists. Medicine and Science in Sports and Exercise, 26, 1510-1515 [PubMed] [Google Scholar]
- McNaughton L.R. (1990) Sodium citrate and anaerobic performance: implications of dosage. European Journal of Applied Physiology 61, 392-397 [DOI] [PubMed] [Google Scholar]
- McNaughton L.R., Ford S., Newbold C. (1997) Effect of sodium bicarbonate ingestion on high intensity exercise in moderately trained women. Journal of Strength and Conditioning Research 11, 98-102 [Google Scholar]
- Ööpik V., Saaremets I., Medijainen L., Karelson K., Janson T., Timpmann S. (2003) Effects of sodium citrate ingestion before exercise on endurance performance in well trained college runners. British Journal of Sports Medicine 37, 485-489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ööpik V., Saaremets I., Timpmann S., Medijainen L., Karelson K. (2004) Effects of acute ingestion of sodium citrate on metabolism and 5-km running performance: a field study. Canadian Journal of Applied Physiology 29, 691-703 [DOI] [PubMed] [Google Scholar]
- Pedersen T.H., Nielsen O.B., Lamb G.D., Stephenson D.G. (2004) Intracellular acidosis enhances the excitability of working muscle. Science 305, 1144-1147 [DOI] [PubMed] [Google Scholar]
- Potteiger J.A., Webster M.J., Nickel G.L., Haub M.D., Palmer R.J. (1996) The effects of buffer ingestion on metabolic factors related to distance running performance. European Journal of Applied Physiology 72, 365-371 [DOI] [PubMed] [Google Scholar]
- Requena B., Zabala M., Padial P., Feriche B. (2005) Sodium bicarbonate and sodium citrate: ergogenic aids?. Journal of Strength and Conditioning Research 19, 213-224 [DOI] [PubMed] [Google Scholar]
- Roth D.A. (1991) The sarcolemmal lactate transporter: transmembrane determinants of lactate flux. Medicine and Science in Sports and Exercise, 23, 925-934 [PubMed] [Google Scholar]
- Roth D.A., Brooks G.A. (1990) Lactate and pyruvate transport is dominated by a pH gradient-sensitive carrier in rat skeletal muscle sarcolemmal vesicles. Archives of Biochemistry and Biophysics 279, 386-394 [DOI] [PubMed] [Google Scholar]
- Schabort E.J., Wilson G., Noakes T.D. (2000) Dose-related elevation in venous pH with citrate ingestion do not alter 40-km cycling time-trial performance. European Journal of Applied Physiology 83, 320-327 [DOI] [PubMed] [Google Scholar]
- Shave R., Whyte G., Siemann A., Doggart L. (2001) The effects of sodium citrate ingestion on 3,000-meter time-trial performance. Journal of Strength and Conditioning Research 15, 230-234 [PubMed] [Google Scholar]
- Sutton J.R., Jones N.L., Toews C.J. (1981) Effect of pH on muscle glycolysis during exercise. Clinical Science 61, 331-338 [DOI] [PubMed] [Google Scholar]
- Tiryaki G.R., Atterbom H.A. (1995) The effects of sodium bicarbonate and sodium citrate on 600 m running time of trained females. The Journal of Sports Medicine and Physical Fitness 35, 194-198 [PubMed] [Google Scholar]
- Van Montfoort M.C., Van Dieren L., Hopkins W.G., Shearman J.P. (2004) Effects of ingestion of bicarbonate, citrate, lactate, and chloride on sprint running. Medicine and Science in Sports and Exercise, 36, 1239-1243 [DOI] [PubMed] [Google Scholar]
- Wilkes D., Gledhill N., Smyth R. (1983) Effect of acute induced metabolic alkalosis on 800 m racing time. Medicine and Science in Sports and Exercise, 15, 277-280 [DOI] [PubMed] [Google Scholar]