

Abstract
Competitive athletics is often associated with moderate left ventricular (LV) hypertrophy, and it has been hypothesized that training mode and type of exercise modulates long-term cardiac adaptation. The purpose of the study was to compare cardiac structure and function among athletes of various sports and sedentary controls. Standard transthoracic two-dimensional M-mode and Doppler echocardiography was performed at rest in Caucasian male canoe/kayak paddlers (n = 9), long distance runners (LDR, n = 18), middle distance runners (MDR, n = 17), basketball players (BP, n = 31), road cyclists (n = 8), swimmers (n = 10), strength/power athletes (n = 9) of similar age (range, 15 to 31 yrs), training experience (4 to 9 years), and age-matched healthy male sedentary controls (n = 15). Absolute interventricular septum (IVS) thickness and LV wall thickness, but not LV diameter, were greater in athletes than sedentary controls. Left ventricular mass of all athletes but relative wall thickness of only BP, swimmers, cyclists, and strength/power athletes were higher as compared with controls (p < 0.05). Among athletes, smaller IVS thickness was observed in MDR than BP, cyclists, swimmers or strength/power athletes, while LDR had higher body size-adjusted LV diameter as compared to BP, cyclists and strength/power athletes. In conclusion, relative LV diameter was increased in long distance runners as compared with basketball players, cyclists, and strength/power athletes. Basketball, road cycling, strength/power, and swimming training were associated with increased LV concentricity as compared with paddling or distance running.
Key points.
The type of cardiac hypertrophy seems to be only moderately exercise-specific.
Long-distance runners develop larger left ventricular dilation as compared with basketball players, cyclists, and strength/power athletes.
Myocardial wall thickening is triggered by different sporting activities that involve large muscle groups.
Key words: Myocardial hypertrophy, left ventricle, echocardiography, athlete
Introduction
Regular participation in competitive sports frequently causes moderate left ventricular (LV) hypertrophy, the type and extent of which depend on the amount and intensity of the training (Fagard, 2003; Pluim et al., 2000). It has been suggested that intense isometric (anaerobic, strength/power) exercise training results in a more concentric LV hypertrophy, which is characterized by an increase in LV mass with also an augmented ratio of wall thickness to the LV diameter (Haykowsky et al., 2002), whereas extensive isotonic (aerobic, endurance) exercise training results in a more prominent enlargement of LV diameter (George et al., 1991; Morganroth et al., 1975; Pluim et al., 2000; Snoeckx et al., 1982).
Some (Csanady and Gruber, 1984; Gates et al., 2004) but not the other (Haykowsky et al., 2000; 2002; Wernstedt et al., 2002; Whyte et al., 2004) groups have found the evidence of dichotomous cardiac adaptation to strength/power versus endurance training. However, differences in echocardiographic indices between marathon runners, cyclists and triathletes (Hoogsteen et al., 2004), as well as between handball players and canoe/kayak paddlers (Gates et al., 2004), have been reported suggesting sport-specific adaptation. Furthermore, it has been proposed that the structural cardiac adaptation to endurance exercise training depends on the group of muscles, i.e., those of lower or upper extremities, primarily involved (Csanady and Gruber, 1984; Gates et al., 2003, 2004). However, specificity of the pattern of cardiac hypertrophy in response to various training programs remains ambiguous (Baggish et al., 2007; Barbier et al., 2006; Naylor et al., 2008) as in many studies no evidence of dichotomous cardiac adaptation has been found even between the strength/power and endurance athletes (Haykowsky et al., 2000; 2002; Shapiro, 1984; Wernstedt et al., 2002; Whyte et al., 2004).
To shed more light on the specificity of cardiac hypertrophy, we compared echocardiographic indices of athletes of seven different sports disciplines and sedentary controls, with particular attention to the type of myocardial geometric pattern. In the present study we chose to investigate distance runners and road cyclists, who do minimal strength training but cover substantial mileage; basketball players, who train and compete in predominantly anaerobic bursts (Balciunas and Stonkus, 2003); swimmers, in which case horizontal position and water submersion during training is dominant; flat- water paddlers, who perform mostly upper-body training of both aerobic and anaerobic type (Shephard, 1987; Tesch, 1983); and strength/power athletes from predominantly combat sports. We hypothesized that training mode and type of exercise might differentially affect characteristics of cardiac adaptation.
Methods
Subjects
A total of 117 Caucasian males aged 20.3 (3.0) (range, 15-31) years volunteered to participate in the study. Experimental procedures were approved by regional bioethics committee, and all subjects gave written informed consent to participate in the study, which conformed to the policy statement with respect to the Declaration of Helsinki. Long-distance runners (n = 18) specialized in races of 5000 m to marathon, while middle-distance runners (n = 17) were specialists of 800 to 3000 m. The cyclists were engaged in road racing, i.e. predominantly endurance (aerobic) activity, whereas swimmers (n = 10) were sprinters to middle-distance performers. The paddlers were training for the Olympic flat-water disciplines; three of them specialized in canoeing. Strength/power group (n = 9) consisted of athletes from combat sports (n = 5), and weight-lifting, shot-put, rugby, and figure skating (n = 1 for each), where the substantial proportion of athletic activity is devoted to explosive movements and bursts of maximal or near maximal intensity rather than static loads.
All athletes were of a similar level, having achieved national or international recognition. They had been regularly engaged in their selected sport for at least three years, and were in their active training season, training six (runners, cyclists, and strength/power athletes) to ten (paddlers, swimmers, BP) times per week on the average at the time of examination.
Sedentary (sport-training for not more than 2 hours a week) but otherwise healthy men (n = 15) of similar age served as controls. The age and anthropometric characteristics of all groups of subjects are presented in Table 1.
Table 1.
Age and anthropometric characteristics of subjects. Data are means (±SD).
| Group | n | Age * (yrs) | Height * (m) | Body mass * (kg) | BMI * (kg•m-2) | BSA * (m2) |
|---|---|---|---|---|---|---|
| 1. LDR | 18 | 21.2 (3.7) | 1.79 (.05) | 67.8 (6.0) | 21.1 (1.8) | 1.85 (.09) |
| 2. MDR | 17 | 20.4 (1.8) | 1.82 (.05) | 69.0 (5.7) | 20.9 (1.6) | 1.89 (.09) |
| 3. Basketball players | 31 | 19.0 (2.5) | 1.94 (.08)1,2,4—8 | 86.3 (10.8) 1,2,4,8 | 22.8 (2.0) 1,2 | 2.18 (.17) 1,2,4,5,8 |
| 4. Cyclists | 8 | 20.1 (3.7) | 1.81 (.06) | 72.0 (7.3) | 21.9 (1.6) | 1.92 (.12) |
| 5. Swimmers | 10 | 20.0 (3.7) | 1.84 (.11) | 76.1 (10.2) | 22.3 (1.4) | 1.99 (.2) |
| 6. Paddlers | 9 | 18.4 (1.3) | 1.85 (.06) | 82.4 (6.8) 1,2 | 24.1 (1.1) 1,2,4,5 | 2.07 (.12) 1,2 |
| 7. Strength/power | 9 | 21.8 (2.9) 3,6 | 1.83 (.06) | 84.2 (11.9) 1,2 | 25.1 (2.3) 1—5 | 2.06 (.17) 1,2 |
| 8. Controls | 15 | 22.5 (1.8) 2,3,6 | 1.81 (.05) | 74.6 (9.9) | 22.7 (2.5) | 1.94 (.14) |
LDR, long-distance runners; n, sample size; SD, standard deviation; MDR, middle-distance runners; BMI, body mass index; BSA, body surface area.
* 1-way ANOVA indicated significant effect of Group on this variable (p < 0.001).
1,2,3,4,5,6,7,8 — post hoc test (T-test adjusted for multiple comparisons) located significant difference (p < 0.05) as compared to those groups.
Echocardiography
Standard transthoracic echocardiographic examinations to measure end-diastolic LV dimensions were performed as recommended by the American Society of Echocardiography (Sahn et al., 1978). Experimental procedures were described in detail elsewhere (Venckunas et al., 2006). Briefly, the same investigator, professional cardiologist, who was blind to the subject’s training group, took three measurements of each parameter, and the average was calculated. Intraobserver variability was tested from the blind measurements taken on 35 tracings, 10 days apart, before to the actual investigation. Coefficients of variation were less than 5% for all of the echocardiographic measures (Vasiliauskas et al., 2006).
Relative wall thickness (RWT) was obtained by dividing the sum of end diastolic LV posterior wall thickness (PWT) and interventricular septum thickness (IVS) by LV diameter. LV mass (in g) was calculated using the following formula (Devereux et al., 1986): LV mass = 0.8 {1.04 × [(IVS + PWT + LVD)3 - (LVD)3]} + 0.6, where LVD is internal LV diameter (all in cm at end diastole). The early (E) and late (A) diastolic peak filling velocities (in m/s) were measured using pulsed Doppler, and the E/A ratio was calculated.
Subjects were asked to fill in a questionnaire indicating their training experience (athletes) and age. Body mass and height of the subjects were measured and body surface area (BSA) was calculated applying the standard equation (Du Bois and Du Bois, 1916).
Statistical analysis
Statistical analyses were carried out using SPSS 11.0 statistical software package. The Kolmogorov-Smirnov test was employed to assess normality of data distribution. BMI, LV diameter, PWT, LV mass, RWT, E and A did not deviate from normality (Kolmogorov-Smirnov test p>0.05). Body mass, height, BSA, and IVS approximated normality, i.e., skewness and kurtosis ranged between -1 and 1 (these variables were not transformed, as transformation would not improve their distribution). The E/A variable did not deviate from normality following square root transformation, whereas age approximated normality after log transformation. To test the effect of group (8 levels) a 1-way ANOVA was carried out. A t-test for independent samples with appropriate adjustment for multiple comparisons (Bonferroni correction) was used to locate the differences between groups. Values of mean and standard deviation are presented. Associations between variables were determined by Pearson correlation analysis.
Results
Anthropometric characteristics of the subjects were significantly influenced by the grouping variable (Table 1). As expected, basketball players were the tallest of all groups, and heavier than runners, cyclists or controls (p < 0.05). Distance runners had lower body mass, body mass index, and BSA than paddlers and strength/power-trained athletes.
No pathological changes either in the structure or function of the myocardium were evident during the echocardiographic examination in any of the subjects. The analysis of raw data indicated that most of the structural and all functional echocardiographic LV parameters were significantly affected by the grouping variable. However, no effect of group was evident on absolute LV diameter. Indices of LV morphology and measured diastolic function parameters of all groups of subjects are presented in Table 2.
Table 2.
Cardiac characteristics in athletic and sedentary males. Data are means (±SD).
| Group | n | LV diam (mm) | IVS ‡(mm) | PWT ‡(mm) | LV mass ‡(g) | LV diam -res † a(mm) | E * (m/s) | A †(m/s) |
|---|---|---|---|---|---|---|---|---|
| 1. LDR | 18 | 55.9(2.4) | 10.7(1.5) | 10.7(1.3) | 241(44) | 56.9 (2.1) 3,4,7,8 | .771(.078) | .461(.058) |
| 2. MDR | 17 | 54.4(3.2) | 10.1(1.1)3,4,5,7 | 10.5(.9) | 219(32) | 55.2 (2.9) | .817(.081) | .441(.059) |
| 3. BP | 31 | 54.8(3.5) | 11.4(.8) | 11.2(1.1) | 252(42) | 53.6 (3.3) | .838(.171)(n=23) | .436(.094)(n=23) |
| 4. Cyclists | 8 | 53.2(3.1) | 11.7(.9) | 11.2(.3) 2 | 244(29) | 53.8 (2.8) | .868(.148) | .505(.085) |
| 5. Swimmers | 10 | 54.7(4.1) | 11.4(.8) | 11.1(.8) | 249(33) | 54.8 (3.5) | .861(.125) | .483(.086) |
| 6. Paddlers | 9 | 56.6(2.9) | 11.0(1.2) | 10.8(1.1) | 252(40) | 56.2 (2.9) | .788(.086) | .403(.065) |
| 7. Strength/power | 9 | 54.0(3.6) | 11.5(.6) | 11.0(.4) | 243(33) | 53.6 (2.6) | .833(.091) | .553(.100)1,2,3,6,8 |
| 8. Controls | 15 | 52.8(3.1) | 9.1(.6)1—7 | 9.7(.8)3,4,5,7 | 184(32)1—7 | 53.2 (2.8) | .714(.095)2,3,4,5,7 | .430(.072) |
LV: left ventricular; diam: diameter, IVS: end-diastolic interventricular septum thickness, PWT: end-diastolic left ventricular posterior wall thickness, E: early diastolic peak filling velocity, A: late diastolic peak filling velocity, LDR: long-distance runners, n: sample size (if sub-sample was used for some variables, n is indicated in parenthesis). BP: Basketball players, MDR: middle-distance runners.
a Unstandardized residuals on BSA were added to the mean of LV diameter across all groups.
* 1-way ANOVA indicated significant effect of Group on this variable (p < 0.05).
† 1-way ANOVA indicated significant effect of Group on this variable (p < 0.01).
‡ 1-way ANOVA indicated significant effect of Group on this variable (p < 0.001).
1,2,3,4,5,6,7,8 — post hoc test located significant difference (p<0.05) as compared to those groups.
All structural (with exception of unadjusted LV diameter) and functional (except E/A ratio) parameters of sedentary controls differed from one or more groups of athletes. Sedentary males had lower IVS and LV mass than any of the tested groups of athletes, and thinner posterior wall than basketball players, cyclists, swimmers, and strength/power athletes. In addition, statistically significant differences were observed between groups of athletes for IVS (Table 2). Middle-distance runners had lower IVS thickness (p < 0.05) as compared to basketball players, road cyclists, swimmers, and strength/power athletes, and thinner posterior wall than cyclists (p < 0.05).
A significant (p < 0.001) effect of group on RWT was detected. As compared with controls, RWT was higher in all groups of athletes except distance runners and paddlers, while no significant differences in RWT were detected between groups of athletes (Figure 1).
Figure 1.
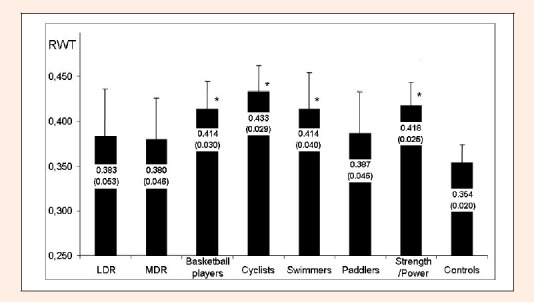
Relative wall thickness (RWT) of athletes and sedentary males. LDR: long-distance runners, MDR: middle-distance runners. Mean and standard deviation are presented. * Significantly higher than in controls (p < 0.05).
Analysis of lusitropic indices (A, E, or E/A) indicated that the E/A ratio was higher in BP as compared with that of strength/power athletes (p < 0.05). Strength/power athletes also exhibited higher late diastolic peak filling velocity (A) than the majority of other groups (Table 2). To test whether these differences were influenced by age (Table 1), it was included as a covariate in a separate 1-way ANOVA. The effect of group on E/A and A, but not E, retained significance, meaning that the effects on the former variables were not just an age-related influence.
Correlation analysis also indicated that IVS, LV diameter, PWT and LV mass correlated with BSA (r of 0.325, 0.368, 0.263 and 0.445, respectively; all p < 0.05). This finding suggests that cardiac size variables are affected by body size. To adjust for confounding body size influence, two different analyses were carried out: (1) residuals were generated for IVS, LV diameter, PWT and LV mass on BSA and, (2) IVS, LV diameter, and PWT were divided by square root of BSA, and LV mass by BSA. Then the derived variables were subjected to 1-way ANOVA.
Both procedures of adjustment gave similar results; the effect of group was retained in IVS, PWT and LV mass variables, with sedentary males exhibiting lower values of traits than athletes (not shown). Left ventricular mass remained similar between the groups of athletes, but the effect of group emerged (p < 0.01) on LV diameter, revealing more voluminous LV chamber in LDR - their indexed LV diameter was larger as compared with basketball players, cyclists, strength/power-trained athletes, and sedentary controls (Table 2, Figure 2). Additionally, PWT was found to be significantly higher in distance runners as compared with controls (p<0.05), and thicker myocardial wall emerged in cyclists as compared with BP (p < 0.05; not shown).
Figure 2.
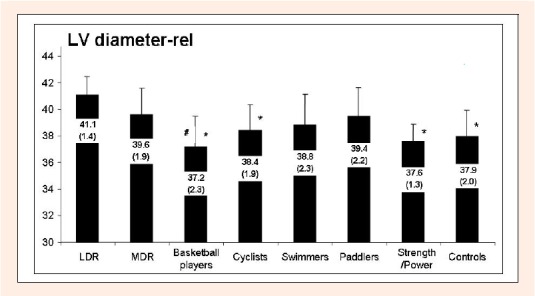
Relative left ventricular diameter (i.e., absolute left ventricular diameter divided by the square root of body surface area) of athletes and sedentary males. LDR: long-distance runners, MDR: middle-distance runners. Mean and standard deviation are presented. * Significantly lower than in long-distance runners (p < 0.05). # Significantly lower than in middle-distance runners (p < 0.05).
Discussion
The results of this study support the notion that regular exercise training induces cardiac hypertrophy that may be manifested by the LV wall thickening and cavity dilation in young athletes. The former aspect of adaptation was observed in all athletes, whereas the latter was specific to the distance runners.
Early echocardiographic studies suggested that the type of myocardial hypertrophy depends on the athletic training program, e.g. preferentially increased LV diameter was found in endurance athletes whereas preferentially increased LV thickness in strength athletes (Morganroth et al., 1975; Snoeckx et al., 1982). Subsequent studies, however, were frequently in discord with that dichotomy of the cardiac structural patterns in athletes. For instance, even very intense strength training aimed at increasing skeletal muscle power/strength/mass would not necessarily result in cardiac wall thickening (Bertovic et al., 1999; Haykowsky et al., 2002; Pelliccia et al., 1993; Wernstedt et al., 2002; Whyte et al., 2004) or the resultant myocardial structure in strength/power athletes would not differ from that of endurance athletes (Legaz Arrese et al., 2005; Pelliccia et al., 1999; Urhausen and Kindermann, 1999; Wernstedt et al., 2002; Whyte et al., 2004). Similarly increased LV mass in all of our athlete groups but some sports-specific differences in echocardiographic parameters suggest the possibility that there is a generic response to exercise (an increased cardiac mass) (Barbier et al., 2006; George et al., 1991; Shapiro, 1984), with (only) some specific effects on various cardiac structural or functional characteristics (Barbier et al., 2006). While the increase in myocardial mass might be influenced by the exercise-related rise in concentration of anabolic hormones (Cumming et al., 1986; Vogel et al., 1985), mechanisms underlying sports-specific influences remain unknown.
Increased myocardial mass due to both cavity dilation and wall thickening is a usual finding in endurance runners (Fagard, 2003; Pluim et al., 2000). It is believed that the increased volume loading during exercise triggers cardiac adaptation in endurance athletes. Additionally, it has also been proposed that the increase in diameter of the LV may be due to stretch of myocardium at rest because of the prolonged filling time associated with bradycardia (Rowell, 1986). The dilation of ventricle is believed to occur via elongation of cardiac myocytes (George et al., 1991). In the present study, long distance runners (but not middle distance runners) had a larger relative LV diameter than basketball players, cyclists, strength/power athletes, or controls (Table 2). The fact that middle distance runners did not differ significantly might be related to the difference in duration of the training stimulus between the long and middle distance runners, as it has been shown that marathoners spend more time for their training than middle distance runners of similar competitive level (Venckunas et al., 2005). Thus, our observation is consistent with the hypothesis that increased exercise-induced volume overload triggers myocardial dilation and indicates that duration of the stimulus is an important factor for the left ventricular chamber enlargement.
Due to the specific technique in flat-water paddling this discipline is particularly demanding for both aerobic and anaerobic capacity of upper body musculature (Shephard, 1987; Tesch, 1983) while lower body is much less involved. This upper-to-lower body imbalance contrasts paddling from other sports disciplines of the present study, providing a model to explore if preferential involvement of different muscle groups plays a role in cardiac adaptation. Several studies reported thicker myocardial walls in individual elite paddlers than athletes from majority of other sports (Csanady and Gruber, 1984; Pelliccia et al., 1991; Pluim et al., 2000). In our study, however, neither high-performance paddlers had exceptionally thick LV walls nor the group of paddlers differed from the other groups of athletes in any parameters of cardiac morphology. Similar absence of difference in myocardial wall thickness between paddlers and endurance athletes was also documented by other echocardiographic studies (Iglesias Cubero et al., 2000; Pelliccia et al., 1999; Whyte et al., 2004). Thus these findings argue against marked differences in LV adaptation to upper versus lower body training, although it has to be acknowledged that detection of possible subtle variations might have been precluded by modest sample size. Possible explanation for the discrepancy between the results of different studies might be related to variation in training regimen (season, specificity) and usually limited statistical power to detect subtle differences.
Conclusion
The majority of echocardiographic parameters were similar between athletes from various sports. Athletes had thicker left ventricular wall, but not absolute cavity diameter than sedentary controls. Body size-adjusted left ventricular diameter was, however, higher in long distance runners as compared with controls, basketball players, cyclists, and strength/power athletes. Relative wall thickness was not increased in distance runners and paddlers but was higher in basketball players, swimmers, cyclists, and strength/power athletes as compared with controls. The results of the present study thus suggest that ventricular chamber dilation is limited to athletes engaged in mainly dynamic endurance sports such as long distance running, while myocardial wall thickening is triggered by different sporting activities that involve large muscle groups. To understand mechanisms underlying enlarged myocardium of athletes, further studies should aim at the revealing peculiarities of the diastolic and systolic as well as coronary circulation parameters during acute exercise of different types (e.g. strength versus endurance activity), as well as to study and compare the response of cardiac morphofunction to actual exercise in athletes of different sports.
Biographies
Tomas Venckunas
Employment
Department of Applied Physiology and Sports Medicine, Lithuanian Academy of Physical Education.
Degree
PhD (Biology)
Research interests
Cardiovascular adaptation to exercise training.
E-mail: t.venckunas@gmail.com
Arimantas Lionikas
Employment
Center for Developmental and Health Genetics, Pennsylvania State University.
Degree
PhD (Biology)
Research interests
Muscle biology and genetic influences.
E-mail: aul104@psu.edu

Jolanta E. Marcinkeviciene
Employment
Institute of Cardiology, Kaunas University of Medicine.
Degree
PhD, MD
Research interests
Cardiovascular alterations in response to pathological and physiologic overload.
E-mail: jolantamar@yahoo.com

Rasa Raugaliene
Employment
Department of Applied Physiology and Sports Medicine, Lithuanian Academy of Physical Education; Institute of Cardiology, Kaunas University of Medicine.
Degree
PhD, MD
Research interests
Changes in cardiac function in patients and athletes.
E-mail: rasara@takas.lt

Aleksandras Alekrinskis
Employment
Depart. of Applied Physiology and Sports Medicine, Lithuanian Academy of PE.
Degree
PhD
Research interests
Short- and long-term adaptation to paddling training.
E-mail: a.stasiulis@lkka.lt

Arvydas Stasiulis
Employment
Professor, Department of Applied Physiology and Sports Medicine, Lithuanian Academy of Physical Education.
Degree
PhD
Research interests
Aerobic capacity and its changes under different conditions including neuromus-cular fatigue.
E-mail: a.alekrinskis@lkka.lt
References
- Baggish A.L., Wang F., Weiner R.B., Elinoff J.M., Tournoux F., Boland A., Picard M.H., Hutter A.M., Wood M.J. (2007) Training-specific changes in cardiac structure and function: a prospective and longitudinal assessment of competitive athletes. Journal of Applied Physiology Dec 20 (Epub ahead of print) [DOI] [PubMed] [Google Scholar]
- Balciunas M., Stonkus S. (2003) Analysis of predominant intensity of physical load in basketball players of different ages during competition and training. Human Movement 2, 17-21 [Google Scholar]
- Barbier J., Ville N., Kervio G., Walther G., Carre F. (2006) Sports-specific features of athlete’s heart and their relation to echocardiographic parameters. Herz 31, 531-543 [DOI] [PubMed] [Google Scholar]
- Bertovic D.A., Waddell T.K., Gatzka C.D., Cameron J.D., Dart A.M., Kingwell B.A. (1999) Muscular strength training is associated with low arterial compliance and high pulse pressure. Hypertension 33, 1385-1391 [DOI] [PubMed] [Google Scholar]
- Csanady M., Gruber N. (1984) Comparative echocardiographic study in leading canoe-kayak and handball sportsmen. Cor et Vasa 26, 32-37 [PubMed] [Google Scholar]
- Cumming D.C., Bunsting L.A., 3rd, Srich G, Ries A.L., Rbar R.W.. (1986) Reproductive hormone increases in response to acute exercise in men. Medicine and Science in Sports and Exercise 18, 369-373 [PubMed] [Google Scholar]
- Devereux R.B., Alonso D.R., Lutas E.M., Gottlieb G.J., Campo E., Sachs I., Reichek N. (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. The American Journal of Cardiology, 57, 450-458 [DOI] [PubMed] [Google Scholar]
- Du Bois D., Du Bois E.F. (1916) A formula to estimate approximate surface area if height and weight be known. Archives of Internal Medicine 17, 129-171 [PubMed] [Google Scholar]
- Fagard R.H. (2003) Athlete’s heart. Heart, 89, 1455-1461 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gates P.E., Campbell I.G., George K.P. (2004) Concentric left ventricular morphology in aerobically trained kayak canoeists. Journal of Sports Sciences 22, 859-865 [DOI] [PubMed] [Google Scholar]
- Gates P.E., George K.P., Campbell I.G. (2003) Concentric adaptation of the left ventricle in response to upper body exercise training. Journal of Applied Physiology 94, 549-554 [DOI] [PubMed] [Google Scholar]
- George K.P., Wolfe L.A., Burggraf G.W. (1991) The ‘athletic heart syndrome’. A critical review. Sports Medicine, 11, 300-330 [DOI] [PubMed] [Google Scholar]
- Haykowsky M.J., Dressendorfer R., Taylor D., Mandic S., Humen D. (2002) Resistance training and cardiac hypertrophy: unravelling the training effect. Sports Medicine, 32, 837-849 [DOI] [PubMed] [Google Scholar]
- Haykowsky M.J., Teo K.K., Quinney A.H., Humen D.P., Taylor D.A. (2000) Effects of long term resistance training on left ventricular morphology. The Canadian Journal of Cardiology 16, 35-38 [PubMed] [Google Scholar]
- Hoogsteen J., Hoogeveen A., Schaffers H., Wijn P.F., van Hemel N.M., van der Wall E.E. (2004) Myocardial adaptation in different endurance sports: an echocardiographic study. The International Journal of Cardiovascular Imaging, 20, 19-26 [DOI] [PubMed] [Google Scholar]
- Iglesias Cubero G., Batalla A., Rodriguez Reguero J.J., Barriales R., Gonzalez V., de la Iglesia J.L., Terrados N. (2000) Left ventricular mass index and sports: the influence of different sports activities and arterial blood pressure. International Journal of Cardiology, 75, 261-265 [DOI] [PubMed] [Google Scholar]
- Legaz Arrese A., Serrano Ostariz E., Gonzalez Carretero M., Lacambra Blasco I. (2005) Echocardiography to measure fitness of elite runners. Journal of the American Society of Echocardiography 18, 419-426 [DOI] [PubMed] [Google Scholar]
- Morganroth J., Maron B.J., Henry W.L., Epstein S.E. (1975) Comparative left ventricular dimensions in trained athletes. Annals of Internal Medicine, 82, 521-524 [DOI] [PubMed] [Google Scholar]
- Pelliccia A., Maron B.J., De Luca R., Di Paolo F.M., Spataro A., Culasso F. (1999) Physiological left ventricular cavity dilatation in elite athletes. Annals of Internal Medicine, 130, 23-31 [DOI] [PubMed] [Google Scholar]
- Naylor L.H., George K., O’Driscoll G., Green D.J. (2008) The athlete’s heart: A contemporary appraisal of the ‘Morganroth Hypothesis’. Sports Medicine, 38, 69-90 [DOI] [PubMed] [Google Scholar]
- Pelliccia A., Maron B.J., Spataro A., Proschan M.A., Spirito P. (1991) The upper limit of physiologic cardiac hypertrophy in highly trained elite athletes. The New England Journal of Medicine 324, 295-301 [DOI] [PubMed] [Google Scholar]
- Pelliccia A., Spataro A., Caselli G., Maron B.J. (1993) Absence of left ventricular wall thickening in athletes engaged in intense power training. The American Journal of Cardiology, 72, 1048-1054 [DOI] [PubMed] [Google Scholar]
- Pluim B.M., Zwinderman A.H., van der Laarse A., van der Wall E.E. (2000) The athlete’s heart. A meta-analysis of cardiac structure and function. Circulation 101, 336-344 [DOI] [PubMed] [Google Scholar]
- Rowell L.B. (1986) Cardiovascular adaptations to chronic physical activity and inactivity. Human circulation: regulation during physical stress. New York: Oxford University Press; 257-286 [Google Scholar]
- Sahn D.J., DeMaria A., Kisslo J., Weyman A. (1978) Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation, 58, 1072-1083 [DOI] [PubMed] [Google Scholar]
- Shapiro L.M. (1984) Physiological left ventricular hypertrophy. British Heart Journal, 52, 130-135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shephard R. (1987) Science and medicine of canoeing and kayaking. SSports Medicine, 4, 19-33 [DOI] [PubMed] [Google Scholar]
- Snoeckx L.H., Abeling H.F., Lambregts J.A., Schmitz J.J., Verstappen F.T., Reneman R.S. (1982) Echocardiographic dimensions in athletes in relation to their training programs. Medicine and Science in Sports and Exercise 14, 428-434 [DOI] [PubMed] [Google Scholar]
- Tesch P.A. (1983) Physiological characteristics of elite kayak paddlers. Canadian Journal of Applied Sport Sciences, 8, 87-91 [PubMed] [Google Scholar]
- Urhausen A., Kindermann W. (1999) Sports-specific adaptations and differentiation of the athlete’s heart. Sports Medicine, 28, 237-244 [DOI] [PubMed] [Google Scholar]
- Vasiliauskas D., Venckūnas T., Marcinkeviciene J., Bartkeviciene A. (2006) Development of structural cardiac adaptation in basketball players. European Journal of Cardiovascular Prevention and Rehabilitation, 13, 985-989 [DOI] [PubMed] [Google Scholar]
- Venckunas T., Raugaliene R., Jankauskiene E. (2005) Structure and function of distance runners’ heart. Medicina (Kaunas) 41, 685-692 [PubMed] [Google Scholar]
- Venckunas T., Stasiulis A., Raugaliene R. (2006) Concentric myocardial hypertrophy after one year of increased training volume in experienced distance runners. British Journal of Sports Medicine, 40, 706-709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vogel R.B., Books C.A., Ketchum C., Zauner C.W., Murray F.T. (1985) Increase of free and total testosterone during submaximal exercise in normal males. Medicine and Science in Sports and Exercise 17, 119-123 [PubMed] [Google Scholar]
- Wernstedt P., Sjostedt C., Ekman I., Du H., Thuomas K.A., Areskog N.H., Nylander E. (2002) Adaptation of cardiac morphology and function to endurance and strength training. A comparative study using MR imaging and echocardiography in males and females. Scandinavian Journal of Medicine & Science in Sports, 12, 17-25 [DOI] [PubMed] [Google Scholar]
- Whyte G.P., George K., Sharma S., Firoozi S., Stephens N., Senior R., McKenna W.J. (2004) The upper limit of physiological cardiac hypertrophy in elite male and female athletes: the British experience. European Journal of Applied Physiology 92, 592-597 [DOI] [PubMed] [Google Scholar]