

Abstract
Background Wrist arthroscopy plays a role in both the diagnosis and the treatment of wrist pathology. It has evolved in the last three decades.
Questions The present status of wrist arthroscopy was investigated by answering the following questions:
-What is its current position in the treatment wrist pathologies according to the literature?
-What is its current position according to hand surgeons?
Methods Analysis of the number of publications on wrist arthroscopy was performed and compared with the number of publications on other arthroscopy topics to assess the current position of wrist arthroscopy. The members of the EWAS (European Wrist Arthroscopy Society) and the members of eight national hand surgery societies were questioned on wrist arthroscopy in daily practice.
Results From 1975 till now, 925 papers on wrist arthroscopy were found. The publications on wrist arthroscopy increased from an average of 8/year (1986) to 26/year (2012). More than half (56.9%) of the respondents of the EWAS perform fewer than 5 wrist arthroscopies per month, and only 7 (10.8%) indicate the performance of more than 10 wrist arthroscopies per month. Seventy-four percent of the orthopedic hand surgeons perform wrist arthroscopy (in 48.5% for therapeutic indications) against 36.8% of plastic surgery hand surgeons (in 23.1% for therapeutic indications).
Conclusion Wrist arthroscopy has taken up a place in the armamentarium of the hand surgeon. The place of wrist arthroscopy in daily practice is related to the background of the hand surgeon.
Keywords: indications, survey, wrist arthroscopy, hand surgeons
Wrist arthroscopy plays an important role in the diagnosis and treatment of many wrist pathologies. On the timeline of medical interventions, wrist arthroscopy has earned its place only in the last three decades. It followed the developments of laparoscopic techniques, starting out of curiosity to inspect the inside of the human body, and trying to find explanations for different ailments.1 The instruments developed for cystoscopy and laparoscopy were subsequently used to inspect joints. With the development of smaller instruments and better visualization techniques, this minimally invasive surgery has become more accepted as a way to diagnose ailments of the joint.
Takagi started with arthroscopy in the knee because of the important clinical problem he was faced with: tuberculosis of the knee, which prevented patients from sitting on their knees, causing an important social handicap.2
Arthroscopic examination of the wrist had been first attempted on cadavers in 1932.3 The challenges in the beginning were the small joint space, the extravasation of fluid when high-pressure fluid infiltration was used for distension of the wrist, and instruments that were too big for this small joint. Improvements in the technique included the use of traction instead of distension with fluid to create space, thus avoiding the complication of fluid extravasation, and the development of specific instruments for the wrist. Furthermore, the description of the entry portals to the wrist in 1986 by Whipple enabled a safe entry to the wrist. In the same year, the first wrist arthroscopy workshop was organized.4
The present article summarizes numerous publications on wrist arthroscopy since 1970 and provides a sampling of the use of wrist arthroscopy by hand surgeons in eight countries.
Materials Section
To assess the current position of wrist arthroscopy, we started by looking at the number of publications in this field. We searched the Medline database for English-only papers using the search terms “wrist' AND 'arthroscopy.” The total number of papers per five-year period was noted from 1970 to 2010. Furthermore, we looked for the current indications for and limitations of wrist arthroscopy in the field of wrist surgery. A second Medline search was performed to retrieve papers using the search terms “Wrist AND Arthroscopy.” This yielded 925 papers. Of these, 214 were review papers. The search was repeated using “Wrist AND Arthroscopy AND Complications,” yielding 226 papers, of which 50 were review papers. “Wrist AND Arthroscopy AND Indications” yielded 76 papers, of which 37 were review papers. “Wrist AND Arthroscopy AND MRI” yielded 172 papers of which 37 were review papers, whereas “Wrist AND Arthroscopy AND CT” yielded 49 papers with 24 review papers.
Only general articles and reviews were included; reports on specific techniques were excluded.
A questionnaire survey was conducted among the members of the EWAS (European Wrist Arthroscopy Society) and the members of eight different national hand surgery societies (the Netherlands, France, Belgium, Germany, Spain, Italy, Japan and Australia).
The first survey, which was conducted among the members of the EWAS, consisted of two sets of questions. The first set related to the surgeons' background and experience in wrist arthroscopy, and the second set aimed at assessing the place of wrist arthroscopy in their clinical practice (Table 1). The survey was undertaken as an electronic survey (Google Doc) composed of open and multiple-choice questions. A reminder was sent to all participants twice to complete the questionnaire.
Table 1. Questions of the survey sent to the EWAS members.
| What is your background in hand surgery? |
|
| How many years of experience in hand surgery do you have? |
Open question Please give answer in years |
| How many years of experience in wrist arthroscopy do you have? |
Open question Please give answer in years |
| How many wrist arthroscopies do you perform a month? | Open question |
| How many of those are diagnostic wrist arthroscopies? |
Open question Diagnostic arthroscopies = inspection of cartilage and ligaments (only introduction of scope and hook) |
| How many of those are interventions? |
Open question Intervention = every intervention, such as biopsy, shaving, VAP, TFCC reinsertion |
| What do you consider to be the place of wrist arthroscopy in the diagnostics of wrist pathology? |
|
| What do you consider to be the place of wrist arthroscopy in the treatment of wrist pathology? |
|
| How many wrist arthroscopies do you think a hand surgeon should have performed to qualify him/her as expert in wrist arthroscopy? | Open question |
| How many wrist arthroscopies do you think a hand surgeon should perform each year to keep his/her expert level? | Open question |
To retrieve more general information, a second questionnaire survey was conducted relating to the background of hand surgeons and their use of wrist arthroscopy in daily practice (Table 2). This survey involved members of nine different national hand surgery societies.
Table 2. Questions of the survey to the members of the national hand surgery societies.
| What is your background for hand surgery? |
|
| Do you perform wrist arthroscopies? |
|
| If you perform wrist arthroscopies, how many wrist arthroscopies do you perform a month? |
|
| If you perform wrist arthroscopies, what is the main objective of the wrist arthroscopy? |
|
Results
Before 1975 there are no references in the Medline database that can be identified using the search terms “wrist AND arthroscopy.” In total there were 925 papers to be found in the Medline database on wrist arthroscopy, with a steady increase in numbers from 1986 to 2013 (Fig. 1).
Fig. 1.

Papers on wrist arthroscopy found in Pubmed with search terms (Wrist AND Arthroscopy) per period of 5 years.
The results of the second search, looking for the indications for and limitations of wrist arthroscopy, are presented in Fig. 2, showing the total number of papers and the number of reviews (in brackets) on the subject. The base-line search was with the terms “wrist AND arthroscopy.” In the subsequent searches these two terms were combined with a new term. As these are new searches, the addition of the number of papers found in each search does not add up to the original 894.
Fig. 2.
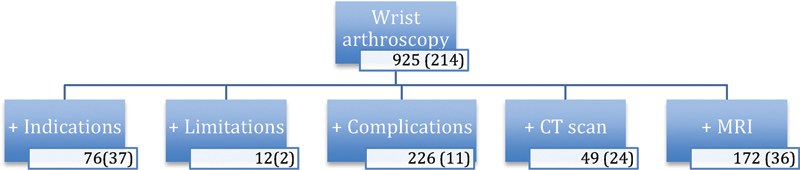
Number of publications in Medline on wrist arthroscopy, categorised by various search terms. Number of reviews between parentheses.
The literature clearly shows that there are two major uses of wrist arthroscopy: as a diagnostic tool and as a therapeutic tool.
As a diagnostic tool, wrist arthroscopy has its place next to magnetic resonance imaging (MRI) and computed tomography (CT) scans. With the improvement of radiologic techniques, numerous papers have compared the diagnostic results of arthroscopy with those of CT and MRI scanning. The results for papers comparing the efficacy of MRI, MR arthrograms, and CT scans for the diagnosis of triangular fibrocartilage complex (TFCC) tears or intrinsic ligament tears can be found in Table 3.5,6,7,8,9,10,11,12 All authors compared the MRI results with the findings during wrist arthroscopy, which they consider to be the gold standard. Mahmood et al conclude that, although the sensitivity and specificity of the MR arthrogram is high, wrist arthroscopy offers the advantage of being both diagnostic and therapeutic.5 Bille et al state that wrist arthroscopy is the accepted reference standard for evaluating ligamentous and cartilaginous injuries of the wrist, but that it entails all the risks of surgery.6
Table 3. Papers on the sensitivity and specificity of MRI and CT scan for the diagnosis of wrist pathology.
| Authors | Modality | Tissue | Sensitivity | Specificity |
|---|---|---|---|---|
| Magee et al8 | MRI (3 T) | TFCC SL |
86 89 |
100 |
| Haims et al9 | MRI (conv) | TFCC peripheral | 17 | |
| Smith10 | MRI (3 T) | SL | 86 | 100 |
| Zlatkin11 | MRI (3 T) | TFCC | 89a | |
| Potter12 | MRI (3 T) | TFCC | 100 | 75 |
| Mahmood et al5 | MR arthro | TFCC SL LT |
90 91 100 |
75 88 100 |
| Bille et al6 | CT arthro | TFCC central TFCC peripheral |
88 30 |
95 94 |
Abbreviations: Arthro: MRI or CT scan with intra-articular contrast; Conv: conventional MRI.
Accuracy instead of sensitivity.
Besides the diagnostic indications for wrist arthroscopy, there are many procedures that can be performed arthroscopically in the wrist. In 2006 Mathoulin and Massarella described the therapeutic indications for 1,000 wrist arthroscopies (Table 4).13 In this series only 4% of the arthroscopies were purely diagnostic.
Table 4. Indications for wrist arthroscopy.
| Arthroscopic assistance for fracture treatment |
| TFCC tears |
| Resection of wrist ganglia |
| Treatment if intrinsic ligament tears |
| Ectomy (radial styloid, wafer, carpal boss) |
| Partial prosthesis |
| Other techniques |
Source: Mathoulin and Massarella.13
Leclercq surveyed the members of the EWAS in 2008 concerning complications they experienced in wrist arthroscopies, and there were 36 respondents who submitted series. (Leclercq C. Complications of wrist arthroscopy, a survey of 10,107 cases. http://www.websurg.com). Eight surgeons had each performed more than 600 wrist arthroscopies, and 13% of their arthroscopies were diagnostic and 87% therapeutic, whereas among the surgeons who had performed fewer than 100 wrist arthroscopies, the rate was 35% diagnostic and 65% therapeutic, indicating that surgeons with less arthroscopic experience tended more to perform diagnostic procedures.
Background of the Surgeons
The rate of response to our first survey sent to the members of the EWAS was 35% after two reminders (65 out of 185 members as of 2009). Approximately half of the respondents (30 out of 65) had a background in orthopedic surgery. A smaller group (23 out of 65) were plastic surgeons, and only a minority (11 out of 65) had a background solely in hand surgery. The majority (51 out of 65) had between 5 and 15 years of experience in hand surgery, but most of these (49 out of 65) had less than 10 years' experience in wrist arthroscopy, indicating that this expertise is often acquired later in the surgical experience (Table 5).
Table 5. Summary of EWAS member survey results.
| Question | Answer | Number | Percentage |
|---|---|---|---|
| Background in hand surgery | Orthopaedic | 30 | 46.9% |
| Plastic | 23 | 35.9% | |
| Hand | 11 | 17.2% | |
| Years of experience in hand surgery | < 5 years | 14 | 21.5% |
| 6-10 years | 19 | 29.7% | |
| 11-15 years | 18 | 28.1% | |
| > 16 years | 14 | 21.5% | |
| Years of experience in wrist arthroscopy | <5 years | 32 | 49.2% |
| 6-10 years | 17 | 26.1% | |
| 11-15 years | 7 | 10.8% | |
| > 16 years | 9 | 13.8% | |
| Number of wrist arthroscopies performed per month | None | 3 | 4.6% |
| < 5 | 37 | 56.9% | |
| 6-10 | 17 | 26.1% | |
| 11-15 | 2 | 3.1% | |
| > 15 | 5 | 7.7% | |
| Number of wrist arthroscopies to qualify as expert | < 50 | 14 | 21.5% |
| 50 | 19 | 29.2% | |
| 100 | 19 | 29.2% | |
| > 100 | 9 | 13.8% | |
| ? | 4 | 6.1% | |
| Number of wrist arthroscopies per year to keep expert level | < 25 | 26 | 40% |
| 25-50 | 28 | 43.1% | |
| 60-100 | 8 | 12.3% | |
| ? | 3 | 4.6% |
More than half of the respondents perform fewer than five wrist arthroscopies per month, and only seven indicated that they perform more than ten wrist arthroscopies per month (Table 5).
When asked about the indications a minority considers wrist arthroscopy as a first choice for diagnostic purposes, and most consider it as either an adjunct to radiology or that there is never an indication for an arthroscopy purely for diagnostic reasons. Individual remarks about diagnostic and therapeutic indications for wrist arthroscopy can be found in Table 6. For therapeutic wrist arthroscopy the majority of respondents feel it is useful for specific indications. Most often mentioned are TFCC lesions and ulnar-sided wrist pain (Table 6).
Table 6. Remarks from EWAS member respondents.
| Remarks on diagnostic wrist arthroscopy | Remarks on therapeutic wrist arthroscopy |
|---|---|
Positive:
|
Positive:
|
We asked the participants how many wrist arthroscopies someone should perform before calling himself or herself an expert in wrist arthroscopy. Seventy-eight percent of the respondents considered that one should have performed more then 50 arthroscopies before one could be regarded as an expert in this field. The number of arthroscopies respondents believed an arthroscopist should perform per year to keep up an expert level varied between <25 (26 respondents) and more then 60 (8 respondents) (Table 5).
The results of the surveys sent to members of national hand surgery societies can be found in Table 7. If we leave out the Netherlands, where the percentage of hand surgeons performing wrist arthroscopy is only 15.4%, a majority (72.6%) of the hand surgeons in these countries perform wrist arthroscopies. This percentage is higher among hand surgeons with an orthopedic background (74.7%) than among those with a plastic surgery background (36.8%). Also, orthopedic hand surgeons perform more therapeutic wrist arthroscopies than their colleagues with a plastic surgery background do (48.5% against 23.1%).
Table 7. Summary of survey responses from national hand surgery society members.
| Nation | Members | Responses | Orthopedic surgeons | Plastic surgeons | Other | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wrist arthroscopy Yes |
WA No |
Wrist arthroscopy Yes |
WA No |
Wrist arthroscopy Yes |
WA No |
||||||
| Netherlands | 154 | 117 | 3 | 11 | 15 | 88 | 0 | 0 | |||
| Diag | 0 | Diag | 11 | Diag | 0 | ||||||
| Ther | 2 | Ther | 0 | Ther | 0 | ||||||
| 50/50 | 1 | 50/50 | 4 | 50/50 | 0 | ||||||
| France | 450 | 85 | 52 | 13 | 8 | 8 | 1 | 3 | |||
| Diag | 9 | Diag | 7 | Diag | 1 | ||||||
| Ther | 43 | Ther | 1 | Ther | 0 | ||||||
| 50/50 | 0 | 50/50 | 0 | 50/50 | 0 | ||||||
| Belgium | 16 | 13 | 3 | 0 | 0 | 0 | 0 | ||||
| Diag | 2 | Diag | 0 | Diag | 0 | ||||||
| Ther | 6 | Ther | 0 | Ther | 0 | ||||||
| 50/50 | 5 | 50/50 | 0 | 50/50 | 0 | ||||||
| Germany | 500 | 74 | 4 | 1 | 30 | 0 | 37 | 2 | |||
| Diag | 0 | Diag | 4 | Diag | 4 | ||||||
| Ther | 3 | Ther | 11 | Ther | 16 | ||||||
| 50/50 | 1 | 50/50 | 15 | 50/50 | 17 | ||||||
| Italy | 71 | 36 | 26 | 0 | 4 | 0 | 4 | ||||
| Diag | 8 | Diag | 0 | Diag | 0 | ||||||
| Ther | 15 | Ther | 0 | Ther | 0 | ||||||
| 50/50 | 13 | 50/50 | 0 | 50/50 | 0 | ||||||
| Australia | 80 | 36 | 23 | 0 | 8 | 5 | 0 | 0 | |||
| Diag | 0 | Diag | 4 | Diag | 0 | ||||||
| Ther | 15 | Ther | 2 | Ther | 0 | ||||||
| 50/50 | 8 | 50/50 | 2 | 50/50 | 0 | ||||||
| Spain | 363 | 42 | 32 | 3 | 1 | 0 | 4 | 2 | |||
| Diag | 4 | Diag | 0 | Diag | 0 | ||||||
| Ther | 10 | Ther | 1 | Ther | 1 | ||||||
| 50/50 | 17 | 50/50 | 0 | 50/50 | 3 | ||||||
| Japan | 3,000 | 151 | 109 | 35 | 2 | 5 | 1 | ||||
| Diag | 24 | Diag | 1 | Diag | 0 | ||||||
| Ther | 38 | Ther | 0 | Ther | 0 | ||||||
| 50/50 | 47 | 50/50 | 1 | 50/50 | 1 | ||||||
| Total | 272 | 92 | 64 | 110 | 43 | ||||||
| Diag | 47 | Diag | 27 | Diag | 5 | ||||||
| Ther | 132 | Ther | 15 | Ther | 17 | ||||||
| 50/50 | 92 | 50/50 | 22 | 50/50 | 21 | ||||||
Discussion
On the timeline of endoscopic developments, wrist arthroscopy is one of the more recent interventions. Currently, wrist arthroscopy is an established technique, and there is a growing interest in this subject. The increasing number of papers on wrist arthroscopy reflects this. However, the number of papers is still significantly lower than those on knee arthroscopy.
In addition to the publication rate, the growing number of members of wrist arthroscopy societies such as the EWAS is indicative of an increasing interest in this subject. In 2009 there were 185 members, whereas in 2013 there are more than 700 members.14 The same goes for the Association of Arthroscopy of North America, with an increase from 70 (1975) to 1,553 (1999).1
Not only is the general interest in wrist arthroscopy increasing, but the place of wrist arthroscopy in the toolbox of the hand surgeon is also shifting. In times when radiologic tools were not available for imaging of tissues, arthroscopy emerged as a means to visualize and inspect the interior of the body.1 This possibility to inspect the inside of the joint has given us a better understanding of the internal wrist anatomy. Ritt describes this development with a clever paradox: “The tunnel vision of wrist arthroscopy has expanded our view of the wrist.”15
Arthroscopy of the wrist in its early years was thus mainly diagnostic. But when it is used as a diagnostic tool, there are also limitations, as McGinthy stated: “Arthroscopy is an operative technique that requires certain motor skills. However, it is not a substitute for careful and complete physical examination and imaging studies.” Furthermore, not every identifiable pathology on arthroscopy is symptomatic or correlated to clinical findings.16
As with most new modalities, once a technique is put in place, the users will try to expand its boundaries and usefulness. Sennwald, in 2001, expressed his concern that perhaps some people are now considering arthroscopy as the panacea for many of the diagnostic troubles we encountered in the past and as an infinite pool of new possibilities for minimally invasive interventions.17
In this literature study we chose to focus on indications and the position of wrist arthroscopy in the diagnosis of wrist pathology. Subjects such as complications and new arthroscopic interventions were left out but are equally interesting to study.
Hand surgeons who initially had an orthopedic training are accustomed to exploring joints with a scope, and the move from knee and shoulder arthroscopy to wrist arthroscopy is probably just a small side-step, as they have already acquired the basic arthroscopic skills such as hand-eye coordination and triangulation skills, which may explain the higher proportion of arthroscopists among hand surgeons than among plastic surgeons.
The respondents to the survey consider the learning curve to be a gentle slope, the majority indicating that a surgeon should have done more than 50 wrist arthroscopies before being able to call himself or herself an expert. The skill should also be sustained by doing a minimum of 20-30 arthroscopies per year. Sixteen respondents even consider a minimum of 50 arthroscopies per year a requirement for keeping an expert level. This represents personal opinion only, however, since there are no data to confirm nor refute these claims, especially since there is no definition of what constitutes an expert.
A limitation of this study is the fact that the EWAS survey was performed in 2009 and the survey of national hand society members in 2011; thus, it may not reflect the current situation. Furthermore, neither the American Society for Surgery of the Hand (ASSH) nor its British counterpart (BSSH), both societies with many members, participated in this study. Lastly, many orthopedic and plastic surgeons who are not members of these participating societies, which have relatively small membership numbers compared with orthopedics and plastic surgical organizations, are excluded, which is a source of bias and may significantly underestimate the incidence of wrist arthroscopy.
Wrist arthroscopy's place as a diagnostic and therapeutic tool will not be a static but rather a dynamic one, shifting in relation to the further development of imaging tools and the development of new arthroscopic interventions.
Most authors of papers on wrist arthroscopy and most respondents to the surveys do agree, however, that it is a skill with a long learning curve. It is certainly a tool that has taken up a place in the armamentarium of the hand surgeon.
The literature search shows a steady increase of publications on wrist arthroscopy. Both the increase in the number of papers and the increase of wrist arthroscopy societies and their number of members indicate a growing interest in this subject. The place of wrist arthroscopy in daily practice is related to the background of the hand surgeon.
Footnotes
Conflict of interest None
References
- 1.Jackson R W. A history of arthroscopy. Arthroscopy. 2010;26(1):91–103. doi: 10.1016/j.arthro.2009.10.005. [DOI] [PubMed] [Google Scholar]
- 2.Jackson R W. Quo venis quo vadis: the evolution of arthroscopy. Arthroscopy. 1999;15(6):680–685. doi: 10.1016/s0749-8063(99)00141-3. [DOI] [PubMed] [Google Scholar]
- 3.De Smet L. Pitfalls in wrist arthroscopy. Acta Orthop Belg. 2002;68(4):325–329. [PubMed] [Google Scholar]
- 4.Bain G I, Munt J, Turner P C. New advances in wrist arthroscopy. Arthroscopy. 2008;24(3):355–367. doi: 10.1016/j.arthro.2007.11.002. [DOI] [PubMed] [Google Scholar]
- 5.Mahmood A, Fountain J, Vasireddy N, Waseem M. Wrist MRI arthrogram v. wrist arthroscopy: What are we finding? Open Orthop J. 2012;6:194–198. doi: 10.2174/1874325001206010194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bille B, Harley B, Cohen H. A comparison of CT arthrography of the wrist to findings during wrist arthroscopy. J Hand Surg Am. 2007;32(6):834–841. doi: 10.1016/j.jhsa.2007.04.005. [DOI] [PubMed] [Google Scholar]
- 7.Kato H, Nakamura R, Shionoya K, Makino N, Imaeda T. Does high-resolution MR imaging have better accuracy than standard MR imaging for evaluation of the triangular fibrocartilage complex? J Hand Surg Br. 2000;25(5):487–491. doi: 10.1054/jhsb.2000.0371. [DOI] [PubMed] [Google Scholar]
- 8.Magee T. Comparison of 3-T MRI and arthroscopy of intrinsic wrist ligament and TFCC tears. Am J Roentgenol. 2009;192(1):80–85. doi: 10.2214/AJR.08.1089. [DOI] [PubMed] [Google Scholar]
- 9.Haims A H, Schweitzer M E, Morrison W B. et al. Internal derangement of the wrist: indirect MR arthrography versus unenhanced MR imaging. Radiology. 2003;227(3):701–707. doi: 10.1148/radiol.2273020398. [DOI] [PubMed] [Google Scholar]
- 10.Smith D K. MR imaging of normal and injured wrist ligaments. Magn Reson Imaging Clin N Am. 1995;3(2):229–248. [PubMed] [Google Scholar]
- 11.Zlatkin M B, Chao P C, Osterman A L, Schnall M D, Dalinka M K, Kressel H Y. Chronic wrist pain: evaluation with high-resolution MR imaging. Radiology. 1989;173(3):723–729. doi: 10.1148/radiology.173.3.2813777. [DOI] [PubMed] [Google Scholar]
- 12.Potter H G, Asnis-Ernberg L, Weiland A J, Hotchkiss R N, Peterson M G, McCormack R R Jr. The utility of high-resolution magnetic resonance imaging in the evaluation of the triangular fibrocartilage complex of the wrist. J Bone Joint Surg Am. 1997;79(11):1675–1684. doi: 10.2106/00004623-199711000-00009. [DOI] [PubMed] [Google Scholar]
- 13.Mathoulin C, Massarella M. Therapeutic interest of wrist arthroscopy: concerning 1,000 cases [in French] Chir Main. 2006;25 01:S145–S160. doi: 10.1016/j.main.2006.07.011. [DOI] [PubMed] [Google Scholar]
- 14.del Piñal F EWAS Council Meeting 2012-13 http://www.wristarthroscopy.eu/hall-of-fame-ewas.php?PHPSESSID=e3dff35eed21d46de2f2f15b0e007fc2&bas=.GEAPtool01&id=475&mit=51cfff5287c80&&adm=PUBLICATION. Revised April 20, 2013. Accessed June 30, 2013.
- 15.Ritt M J. Arthroscopy: the giant leap forward in wrist surgery? J Hand Surg Br. 2001;26(3):238–240. doi: 10.1054/jhsb.2001.0617. [DOI] [PubMed] [Google Scholar]
- 16.McGinty J B, Johnson L L, Jackson R W, McBryde A M, Goodfellow J W. Uses and abuses of arthroscopy: a symposium. J Bone Joint Surg Am. 1992;74(10):1563–1577. [PubMed] [Google Scholar]
- 17.Sennwald G. Diagnostic arthroscopy: indications and interpretations of findings. J Hand Surg [Br] 2001;26B(3):241–246. doi: 10.1054/jhsb.2001.0578. [DOI] [PubMed] [Google Scholar]