

Abstract
Primary perineal hernia is a rare clinical condition wherein herniation of viscera occurs through pelvic diaphragm. They are usually mistaken for sciatic hernia, rectal prolapse or other diseases in the perineum. Correct identification of the type of hernia by imaging is crucial for planning treatment. We present a case of primary posterior herniation of urinary bladder and rectal wall through levator ani repaired laparoscopically using a mesh repair.
Keywords: Laparoscopy, perineal hernia, laparoscopy
INTRODUCTION
Primary perineal hernia is a rare clinical condition wherein herniation of viscera occurs through pelvic diaphragm. They are usually mistaken for sciatic hernia, rectal prolapse, or other diseases in the perineum. Correct identification of the type of hernia by imaging is crucial for planning treatment. We present a case of primary posterior herniation of urinary bladder and rectal wall through levator ani repaired laparoscopically using a mesh repair.
CASE REPORT
A 63-year-old multiparous lady presented with complaints of a bulge in the gluteal region that appeared while coughing. Physical examination revealed a visible bulge in the posterior perineal region that could be reduced to reveal a defect in the perineum with an expansile cough impulse [Figure 1]. Per rectal examination revealed a palpable defect in the pelvic floor muscles. Computed tomography (CT) scan and magnetic resonance imaging (MRI) of pelvis demonstrated a perineal hernia with herniation of a portion of the urinary bladder and rectal wall through pelvic floor [Figures 2a–c].
Figure 1.

Figure showing the herniation near right gluteal region near anus
Figure 2.
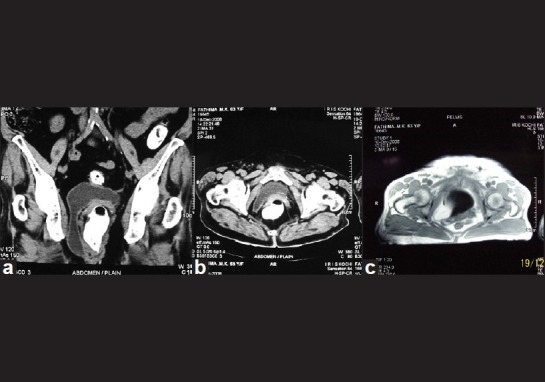
(a-c) CT scan and MRI images showing urinary baldder herniating through perineum
She underwent laparoscopic exploration, mesh repair of the hernial defect, and rectopexy. A defect was noticed in the levator ani on the right side, through which the urinary bladder and a portion of rectum was herniated. Herniated contents were dissected free, rectum was fully mobilized up to the pelvic floor, and a defect in the pelvic floor was displayed. A polypropylene mesh was deployed to cover the defect, mesh rectopexy was done using a polypropylene mesh [Figure 3], and hitching of urinary bladder to the anterior abdominal wall was performed. At the time of writing this article, the patient is symptom free on follow-up of 22 months.
Figure 3.

Laparoscopic appearance of mesh being deployed
DISCUSSION
Primary perineal hernias are very rare, with about 100 cases reported in the literature.[1] They usually protrude through the pelvic diaphragm, and an anterior or posterior form can be distinguished based on their position relative to the transverse perineii muscle.[1] These hernias occur most commonly in older, multiparous women and manifest clinically as a unilateral bulge in the area of the labia or the gluteal or the perineal region, and they are frequently detected on bimanual rectal-vaginal examination.[1] However, perineal hernias maybe mistaken for other diseases of the perineum and adjacent organs, most importantly, a sciatic hernia.[2] Rectal prolapse also may be confused with a posterior perineal hernia, although the two can exist concomitantly. CT Scan and dynamic MRI of the pelvis provide excellent delineation of the pelvic floor anatomy and the details of the hernia and its contents.[2,3]
Repair of perineal hernias may be done using transperitoneal, perineal, and combined approaches.[1,4] The transperitoneal, open or laparoscopic approach is the preferred method for complete repair, the contents of the hernia are reduced, and the defect in the pelvic floor is covered with a non-absorbable mesh with the addition of a rectopexy and or bladder fixation.[1,4,5] Sorelli[5] has recently reported advantages of laparoscopic approach in repair of perineal hernia. The perineal approach may be suitable for a small hernia defect in an unhealthy patient although the risk of recurrence is high.[4]
CONCLUSION
Primary perineal hernias are rare. Accurate delineation of the defect by proper imaging is essential for planning the treatment. Laparoscopic repair provides good relief of symptoms with minimal morbidity.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Salameh JR. Primary and unusual abdominal wall hernias. Surg Clin N Am. 2008;88(1):45–60. doi: 10.1016/j.suc.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 2.Salum MR, Prado-Kobata MH, Saad SS, Matos D. Primary perineal posterior hernia: An abdominoperineal approach for mesh repair of pelvic floor. Clinics (Sao Paulo) 2005;60:71–4. doi: 10.1590/s1807-59322005000100013. [DOI] [PubMed] [Google Scholar]
- 3.Baleato GS, Vilanova J, Lopez CL, Gracía-Figueiras R, Pazos GG, Ortiz-Terán L. Perineal hernia. Emerg Radiol. 2009;16(5):395–8. doi: 10.1007/s10140-008-0768-4. [DOI] [PubMed] [Google Scholar]
- 4.Michael JZ, Stanley WA. Hernias. In: Michael Zinner, Jr, Stanley Ashley., editors. Maingot's Abdominal Operations. 11th ed. New York: McGraw Hill; 2007. pp. 128–30. [Google Scholar]
- 5.Sorelli PG, Clark SK, Jenkins JT. Laparoscopic repair of primary perineal hernias: The approach of choice in the 21st century. Colorectal Dis. 2012;14:72–3. doi: 10.1111/j.1463-1318.2011.02807.x. [DOI] [PubMed] [Google Scholar]