

Abstract
Introduction:
Controversy exists over the pain during prostate biopsy. Periprostatic nerve block (PNB) is a gold standard anesthetic technique during transrectal ultrasound (TRUS)-guided prostate biopsy. Recent studies showed that PNB alone is insufficient as analgesic. We compared the efficacy of tramadol and intraprostatic nerve block (INB) in addition to PNB.
Materials and Methods:
We conducted a prospective double blinded placebo controlled study at our institute in 150 consecutive patients. Patients were randomized into three groups. Group A received PNB with INB with 1% lignocaine. Group B received oral tramadol with PNB. Group C patients were administered PNB only with 1% lignocaine. Patients were asked to grade the pain level using 11 point linear visual analog scale (VAS) at the time of ultrasound probe insertion, at time of anesthesia, during biopsy, and 30 min after biopsy.
Results:
The study groups were comparable in demographic profile, prostate-specific antigen (PSA) levels, and prostate size. Group A recorded the minimum mean pain score of 2.66 during prostate biopsy which was significantly lower than group 3 (P < 0.001). Group B recorded significantly lower pain score at time of probe insertion and at anesthetic needle insertion than other two groups.
Conclusions:
PNB provides better pain control in TRUS-guided prostate biopsy but still there is need of additional analgesic in the form of tramadol or INB. Tramadol has advantage of oral intake and analgesic effect at time of probe insertion and at nerve block. Both tramadol and INB may be used in combination along with PNB.
Keywords: Analgesia, intraprostatic nerve block, lignocaine, tramadol
INTRODUCTION
Transrectal ultrasound (TRUS)-guided biopsy has become the standard procedure to diagnose prostatic carcinoma. Histological diagnosis is must before jumping on any kind of treatment of prostatic carcinoma and TRUS-guided biopsy is only way to it. In recent years, a consensus have been reached that sextant sampling is inadequate and sampling with 8 cores or greater is suggested.[1] These extended techniques allow us to obtain more biopsy samples and increase the prostate cancer detection rate. This increased no. of cores translates to cumulative pain and increased pain scores if no analgesia is given. This concept was called ‘cumulative pain’ given by Kevar et al.[2]
Studies show that almost 20% of patients reported significant pain and they would refuse re-biopsy without analgesia.[1] Men fixed for TRUS-guided biopsy experience considerable psychological stress. Reasons for this stress are manifold like fear of diagnosis of cancer, anal route of penetration, examined organ being part of male sexual system, and anticipated pain during the procedure. Although most of the morbidities are minor yet traumatic and worrisome to patient. Crudwell et al. found moderate to severe pain scores during prostate biopsy in his patients.[3] Anxiety is common in men before and during the procedure. In those patients who are anxious experience higher pain scores for example young people.[4] Similarly, patients having past unpleasant experiences have higher pain scores.
Various modalities have been described in the literature to give analgesia during TRUS-guided prostate biopsy but no standard technique has been proved to be most effective. In recent times periprostatic nerve block (PNB) has emerged as a gold standard technique for prostate biopsy but it has been shown by various authors that it provide significant analgesia yet insufficient for making it acceptable alone. This led to combining other analgesics with PNB like tramadol or intra-prostatic nerve block. But only few studies are available at present and needs more studies to reach any consensus. In this study, we compared tramadol and intraprostatic nerve block (INB) with PNB in TRUS-guided prostate biopsy to find best adjunct to PNB in TRUS biopsy.
MATERIALS AND METHODS
This prospective randomized controlled trial comparing tramadol and INB with PNB was done in 150 patients in department of urology in collaboration with department of radio-diagnosis between June 2010 and September 2011. The plan has been approved by local ethics committee. Patients were randomized using card method. Patients were asked to pick an envelope from three packs of opaque sealed envelope. Drugs also were grouped according to the number on envelope. Urologist doing the biopsy was unaware of the grouping. He then used drugs from the numbered drugs (without information about its content) according to the number on envelope. The drug was prepared by the fellow who unaware of study protocol as per envelope selected.
Patients having elevated prostate-specific antigen (PSA) (>4 ng/ml) and abnormal digital rectal examination (discrete nodule, focal induration, a diffusely hard prostate) were included in this study.
Patient having history of any analgesic intake within last 48 h (5), history of previous biopsy (8), chronic prostatitis (2), chronic pelvic pain (2), inflammatory bowel diseases (0), anorectal problems (1), active urinary tract infections (7), local anesthetic allergy were excluded from this study. A total of 25 patients were excluded from study, the number of patients excluded written in bracket against each criterion.
Patient preparation
Informed consent was obtained prior to the procedure. All patients were given phosphatidyl choline enema 1 h before procedure. Administration of prophylactic antibiotics around the time of biopsy was given starting 1 day before in form of ciprofloxacin 500 mg twice a day for 3 day to prevent infection.
A digital rectal examination with lubricating jelly was performed prior to insertion of the probe to rule out any rectal pathology that would contraindicate insertion of the probe, and to allow the identification of any palpable prostatic abnormalities to which special attention could be paid during ultrasound examination.
All patients were assigned in three groups A, B, C randomly of 50 patients each.
Group A (Nerve block with INB): Patients were given multivitamin (Vitamin c and vitamin b12) as placebo tablet 3 h before the procedure. Nerve block using 5 ml 1% lignocaine was injected just lateral to the junction between prostate base and seminal vesicle just before biopsy. The probe was adjusted to the sagittal plane, with the on-screen biopsy-guide operational before placement. A 22-gauge, 7-inch spinal needle was placed through the biopsy-guide channel under ultrasound guidance into the area where the prostatic innervation enters the gland through the guide fitted on probe. The probe is angled laterally until the notch between the prostate and the seminal vesicle was visualized. One % lignocaine (5 ml) was injected on each side. Successful placement of the needle was confirmed when the injected causes a separation of the seminal vesicles and prostate from the rectal wall called, the ultrasonic wheal. After this 5 ml of 1% lignocaine is infilterated with the intraprostatic injection technique. This involved direct prostatic injection under ultrasound guidance on both sides near base.
Group B (Tramadol): Patients were given 100 mg tramadol tablet 3 h before procedure and 1% lignocaine used for PNB and 0.9% NaCl was used for intraprostatic injection.
Group C (Control): Same as group A expect 0.9% NaCl was used for intraprostatic injection.
Method of taking biopsy
The patients were positioned in left lateral decubitus position (lying on left side). This allows for easier insertion of the rectal probe. The probe was gently advanced into the rectum, to the base of the bladder until the seminal vesicles are visualized. Transverse images were then obtained as the probe moved back from the prostate base to the prostate apex. With the transducer at the largest cross-sectional image in the transverse plane and in the mid-sagittal plane, prostate volume was calculated.
An 18-gauge and 20 cm biopsy needle loaded in a spring-action automatic biopsy device was used to procure 12 prostate core biopsy specimens. Needle was introduced through the needle guide fitted over the probe under ultrasound guidance. Area of interest was viewed and biopsies taken under ultrasound guidance.
Pain was assessed using numeric visual analog scale (VAS) by the same urologist upon completeness of biopsy procedure. Patients were already shown 11 point visual scale and about marking procedure [Figure 1]. After taking biopsy patients were shown 10 cm visual scale again and asked to mark the pain score at these times individually.
Figure 1.
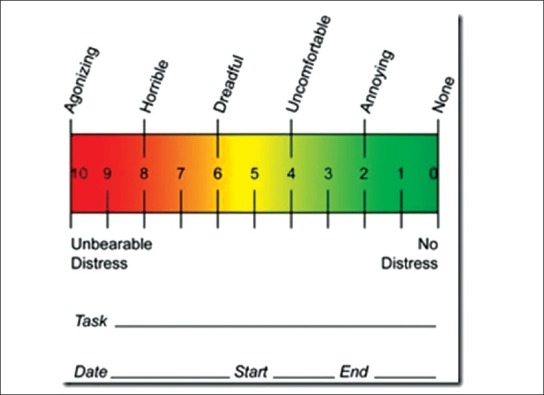
Visual analog scale
At the time of probe insertion
At the time of anesthesia
At the time of taking biopsy.
Patients were asked to rest for 30 min and asked to mark again after 30 min on the same scale.
Statistics
The data was analyzed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). The differences in pain scales, age, PSA and gland size between the three groups were analyzed using Student's t test.
RESULTS
The study groups were comparable in demographic profile PSA and prostate size [Table 1]. The mean pain scores in group A during probe insertion, during anesthesia, during biopsy, and 30 min after biopsy were 2.94 ± 0.77, 4.02 ± 1.12, 2.66 ± 0.69, 0.60 ± 0.78, respectively. The mean pain scores in group B during probe insertion, during anesthesia, during biopsy, and 30 min after biopsy were 2.69 ± 0.77, 3.32 ± 0.62, 3.22 ± 0.51, 0.59 ± 0.63, respectively [Table 2, Figure 2]. The mean pain scores in group C during probe insertion, during anesthesia, during biopsy, and 30 min after biopsy were 3.02 ± 0.85, 4.01 ± 1.46, 3.36 ± 0.94, 0.78 ± 0.74, respectively. Group A recorded the minimum mean pain score of 2.66 during prostate biopsy which was significantly lower than group C (P < 0.001). Group B recorded significantly lower pain score at time of probe insertion and at anesthetic needle insertion than group A. The tramadol group also recorded significantly lower pain score at time of probe insertion, anesthesia and biopsy but not at 30 min post-biopsy than the control group. There is no significant difference in pain score at time of biopsy between A and B. So tramadol provides significant analgesia at all times expect post procedure time with added advantage of oral intake. Post procedure pain is less than 1 so not significant at all. Our complications were rectal bleed (42), urinary retention (15), hematuria (24), prostatits (5), nausea and vomiting (3). Number in bracket shows complication in our study. Nausea and vomiting in the tramadol group only. A total of 34 patients had complications. They were distributed in each group with 12 in group A, 10 in group B, and 12 in group C.
Table 1.
Patients characteristics
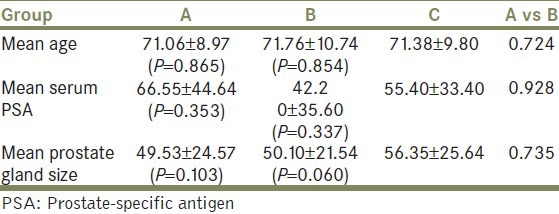
Table 2.
Result of mean pain score
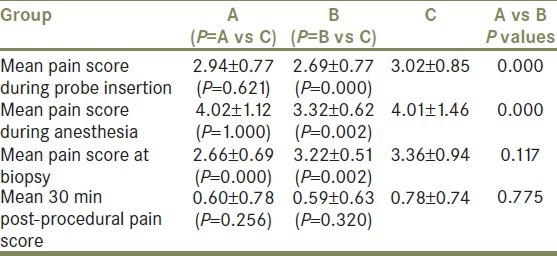
Figure 2.
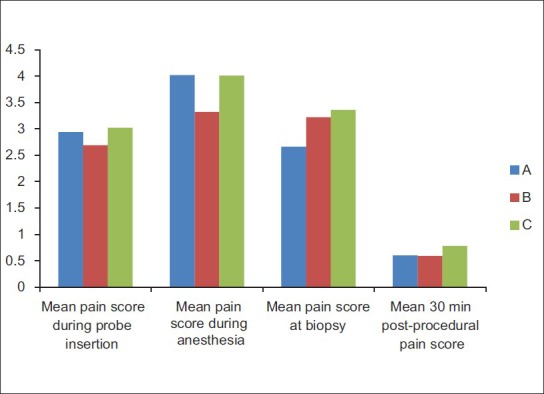
Result of mean pain score
DISCUSSION
Although TRUS-guided prostate biopsy is safe but patients experiences significant discomfort during the procedure.[5] Pain associated with TRUS-guided prostate biopsy is important since many patients must undergo re-biopsy and pain may prevent them from doing this.
Pain is a complex perceptual experience and is difficult to quantify. This pain is translation of actual somatic and visceral pain, anxiety, psychological stress, and the interpretation of scores remain subjective. In the report of Desgrandchamps et al., at the end of the procedure patients were asked to score the severity of discomfort using a self-administered verbal rating scale, which consisted of a list of adjectives describing different levels of pain, from none to intolerable pain.[6] Linear 11 point VAS is easily comprehensible and easy to demonstrate and remains the most established method to score pain. Others have modified it and used this in various ways.
Pain during prostate biopsy is due to insertion of the ultrasound probe and needle puncture into the prostate. The nerve supply of prostate is autonomic and originates from the inferior hypogastric plexus. Nerves pass along the plane between the rectum and prostatic capsule. The pain associated with prostate biopsy is thought to be contributed by direct contact of the biopsy needle with these nerves within the stroma and the prostatic capsule.[7]
Conde et al. in 2006 found that bilateral PNB is better analgesic than oral morphine.[8]
But over the years it has been established by various authors that PNB is very effective for TRUS-guided prostate biopsy pain. Since its introduction by Nash et al., this technique has gone further to the extent of a gold standard technique of prostate biopsy. Various authors in their study found it very effective than placebo, control, and other analgesic methods.[9,10,11,12]
But it is far from settlement as others found procedure still very painful. Wu et al. proposed that PNB is not effective for prostatic biopsy pain.[13] Bozlu et al. proposed in 2004 that PNB and tramadol have no analgesic effect during prostate biopsy.[14]
So need for better analgesic was felt and in 2005 when Mutaguchi et al. proposed a new intraprostatic analgesia technique to anaesthetize the prostate that requires blocking all sensory nerves from the posterior and anterior sides. They found that in 71 patient out of 170 patients have mean pain score of 1.9 as compared to 2.6 in PNB. This was found to be clinically significant.[15] We also found similar result but with the combination of PNB and INB. We also find that tramadol is effective at probe insertion and at anesthetic application where intraprostatic block is not effective.
Cam et al. also reported that combining intraprostatic local anesthetic and PNB is an effective form of analgesia. They used this technique in 100 patient and found it to be very effective with mean pain score of 0.75 as compared to 2.17 of PNB alone.[16] In our study, we also found similar result.
In 2007, Lee et al. published results of their study in which they divided 152 patients in three groups. One group received PNB alone, other received INB alone and third received both. They found that group with both PNB and INB has best pain control at time of anesthesia and biopsy. It was found to be statistically significant. In our study, a significant pain difference was found only at time of biopsy.[17]
Obek et al. found that tramadol has role in prostate biopsy but could not comment much. In our study, tramadol has proved its role at time of probe insertion and at nerve block time.[18]
In 2008, Olmez et al. published a study comparing intramuscular lornoxicam and tramadol and found tramadol as significantly better analgesic. In our study, oral tramadol was found better at certain times of procedure.[19]
Hirsh et al. also found tramadol to be effective as analgesia at time of biopsy.[20]
In our study, the mean pain scores in group A during probe insertion, during anesthesia, during biopsy, and 30 min after biopsy were 2.94 ± 0.77, 4.02 ± 1.12, 2.66 ± 0.69, 0.60 ± 0.78, respectively. The mean pain scores in group B during probe insertion, during anesthesia, during biopsy, and 30 min after biopsy were 2.69 ± 0.77, 3.32 ± 0.62, 3.22 ± 0.51, 0.59 ± 0.63, respectively [Table 2]. The mean pain scores in group C during probe insertion, during anesthesia, during biopsy, and 30 min after biopsy were 3.02 ± 0.85, 4.01 ± 1.46, 3.36 ± 0.94, 0.78 ± 0.74, respectively. Group A recorded the minimum mean pain score of 2.66 during prostate biopsy which was significantly lower than group C (P < 0.001). Group B recorded significantly lower pain score at time of probe insertion and at anesthetic needle insertion than group A. The tramadol group also recorded significantly lower pain score at time of probe insertion, anesthesia and biopsy but not at 30 min post biopsy than the control group. There is no significant difference in pain score at time biopsy between A and B. So tramadol provides significant analgesia at all times expect post procedure time with added advantage of oral intake. Post procedure pain is less than 1 so not significant at all. So tramadol provides significant analgesia at all times expect post procedure time with added advantage of oral intake.
CONCLUSIONS
Periprostatic nerve block provides better pain control in TRUS-guided prostate biopsy but still there is need of additional analgesic in form of tramadol or intraprostatic nerve block. Tramadol has advantage of oral intake and analgesic effect at time of probe insertion and at nerve block. It is also to use as it avoids intraprostatic injection. Both tramadol and INB may be used in combination along with PNB.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Bingqian L, Peihuan L, Yudong W, Jinxing W, Zhiyong W. Intraprostatic local anesthesia withperiprostatic nerve block for transrectal ultrasound guided prostate biopsy. J Urol. 2009;182:479–83. doi: 10.1016/j.juro.2009.04.029. [DOI] [PubMed] [Google Scholar]
- 2.Kaver I, Mabjeesh NJ, Matzkin H. Randomized prospective study of periprostatic localanesthesia during transrectal ultrasound-guided prostate biopsy. Urology. 2002;59:405–8. doi: 10.1016/s0090-4295(01)01538-2. [DOI] [PubMed] [Google Scholar]
- 3.Crundwell MC, Cooke PW, Wallace DM. Patients’ tolerance of transrectalultrasound-guidedprostatic biopsy: An audit of 104 cases. BJU Int. 1999;83:792–5. doi: 10.1046/j.1464-410x.1999.00011.x. [DOI] [PubMed] [Google Scholar]
- 4.Saraçoğlu T, Unsal A, Taşkın F, Sevinçok L, Karaman CZ. The impact of pre-procedural waiting period and anxiety level on pain perception in patients undergoing transrectal ultrasound- guidedprostate biopsy. Diagn Interv Radiol. 2012;18:195–9. doi: 10.4261/1305-3825.DIR.4643-11.1. [DOI] [PubMed] [Google Scholar]
- 5.Ochiai A, Babaian RJ. Update on prostate biopsy technique. Curr Opin Urol. 2004;14:157–62. doi: 10.1097/00042307-200405000-00004. [DOI] [PubMed] [Google Scholar]
- 6.Desgrandchamps F, Meria P, Irani J, Desgrippes A, Teillac P, Le Duc A. The rectal administration oflidocaine gel and tolerance oftransrectal ultrasonography-guided biopsy of the prostate: A prospective randomized placebo-controlled study. BJU Int. 1999;83:1007–9. doi: 10.1046/j.1464-410x.1999.00080.x. [DOI] [PubMed] [Google Scholar]
- 7.Hollabaugh RS, Jr, Dmochowski RR, Steiner MS. Neuroanatomy of the male rhabdosphincter. Urology. 1997;49:426–34. doi: 10.1016/S0090-4295(96)00497-9. [DOI] [PubMed] [Google Scholar]
- 8.Conde Redondo C, Alonso Fernández D, Robles Samaniego A, Del Valle González N, Castroviejo Royo F, Delgado Marcos C, et al. TRUS-guided biopsy: Comparison of two anesthetic methods. Actas Urol Esp. 2006;30:134–8. doi: 10.1016/s0210-4806(06)73414-3. [DOI] [PubMed] [Google Scholar]
- 9.Nash PA, Bruce JE, Indudhara R, Shinohara K. Transrectal ultrasound guided prostatic nerve blockade eases systematic needle biopsy of the prostate. J Urol. 1996;155:607–9. [PubMed] [Google Scholar]
- 10.Soloway MS, Obek C. Periprostatic local anesthesia before ultrasound guided prostate biopsy. J Urol. 2000;163:172–3. [PubMed] [Google Scholar]
- 11.Taverna G, Maffezzini M, Benetti A, Seveso M, Giusti G, Graziotti P. A single injection of lidocaineas local anesthesia for ultrasound guided needle biopsy of the prostate. J Urol. 2002;167:222–3. [PubMed] [Google Scholar]
- 12.Matlaga BR, Lovato JF, Hall MC. Randomized prospective trial of a novel local anesthetic technique for extensive prostate biopsy. Urology. 2003;61:972–6. doi: 10.1016/s0090-4295(03)00003-7. [DOI] [PubMed] [Google Scholar]
- 13.Wu CL, Carter HB, Naqibuddin M, Fleisher LA. Effect of local anesthetics on patient recovery after transrectal biopsy. Urology. 2001;57:925–9. doi: 10.1016/s0090-4295(01)00930-x. [DOI] [PubMed] [Google Scholar]
- 14.Bozlu M, Atici S, Ulusoy E, Canpolat B, Cayan S, Akbay E, et al. Periprostaticlidocaine infiltration and/or synthetic opiod (meperidine or tramadol) administration have no analgesic benefit during prostate biopsy. A prospective randomizeddouble-blind placebo-controlled study comparing different methods. UrolInt. 2004;72:308–11. doi: 10.1159/000077683. [DOI] [PubMed] [Google Scholar]
- 15.Mutaguchi K, Shinohara K, Matsubara A, Yasumoto H, Mita K, Usui T. Local anaesthesia during 10 core biopsy of the prostate: Comparison of 2 methods. J Urol. 2005;173:742–5. doi: 10.1097/01.ju.0000152119.28959.3a. [DOI] [PubMed] [Google Scholar]
- 16.Cam K, Sener M, Kayikci A, Akman Y, Erol A. Combined periprostatic and intraprostatic local anesthesia for prostate biopsy: A double-blind, placebo controlled, randomized trial. J Urol. 2008;108:141–4. doi: 10.1016/j.juro.2008.03.052. [DOI] [PubMed] [Google Scholar]
- 17.Lee HY, Lee HJ, Byun SS, Lee SE, Hong SK, Kim SH. Effect of intraprostatic local anesthesia during transrectal ultrasound guided prostate biopsy: Comparison of 3 methods in a randomized, doubleblind, placebo controlled trial. J Urol. 2007;178:469–72. doi: 10.1016/j.juro.2007.03.130. [DOI] [PubMed] [Google Scholar]
- 18.Obek C, Ozkan B, Tunc B, Can G, Yalcin V, Solok V. Comparison of 3 different methods ofanesthesia before transrectal prostate biopsy: A prospective randomized trial. J Urol. 2004;172:502–5. doi: 10.1097/01.ju.0000131601.06286.26. [DOI] [PubMed] [Google Scholar]
- 19.Olmez G, Kaya S, Aflay U, Sahin H. Comparison of lornoxicam versus tramadol analgesia fortransrectal prostate biopsy: A randomized prospective study. Int Urol Nephrol. 2008;40:341–4. doi: 10.1007/s11255-007-9297-4. [DOI] [PubMed] [Google Scholar]
- 20.Hirsh I, Kaploun A, Faris G, Appel B, Shneider I, Stein A, Pizov R. Tramadol improves patients’tolerance of transrectal ultrasound-guided prostate biopsy. Urology. 2007;69:491–4. doi: 10.1016/j.urology.2006.10.035. [DOI] [PubMed] [Google Scholar]