

Propofol is a hypnotic agent that is widely used for the induction and maintenance of general anesthesia and sedation in critically ill patients. Its properties of fast action and fast recovery allows for frequent neurological evaluations and assessments during sedation in the intensive care unit (ICU). Here, we report 3 cases of green discoloration of urine after continuous infusion of propofol.
Case 1
A 49-year-old female patient with a history of epilepsy and alcohol abuse was admitted to the emergency room (ER) for loss of consciousness after suffering a seizure. Central pontine myelinolysis was suspected. On admission to the ICU, the following laboratory results were found: albumin, 3.8 g/dl; total bilirubin, 3.2 mg/dl; aspartate aminotransferase (AST), 209 U/L; alanine transaminase (ALT), 50 U/L; blood urea nitrogen (BUN), 9.2 mg/dl; and creatinine, 0.8 mg/dl. Mechanical ventilation was instigated under sedation with midazolam. As frequent neurological examinations were required, midazolam was replaced with propofol. After titration, adequate depth of sedation was achieved at a rate of 4 mg/kg/h. Green urine was found 64 hours after continuous infusion of propofol (Fig. 1A). Blood examination revealed a serum albumin level of 2.5 g/dl, total bilirubin 0.7 mg/dl, and direct bilirubin 0.4 mg/dl. Urinalysis revealed the following: pH, 6.0; urine specific gravity (SG), 1.020; bilirubin content, negative; and urobilinogen level, 8.0 EU/dl. Urine cultures were negative. We suspected propofol to be the cause of the green urine. Urine color recovered 6 hours after discontinuation of propofol. A repeat urinalysis showed: pH, 7.0; urine SG, 1.015; bilirubin content, negative; and urobilinogen level, 8.0 EU/dl. During 3 months of admission, this was the only instance of urine discoloration.
Fig. 1.
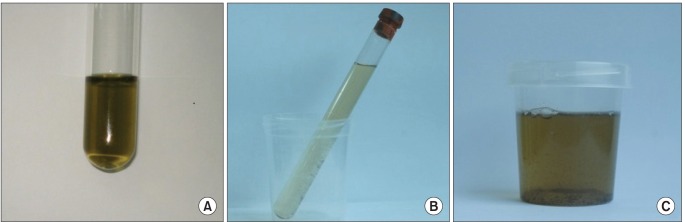
Green discoloration of urine after propofol infusion in (A) case 1, (B) case 2, (C) case 3.
Case 2
A 19-year-old male patient with a history of epilepsy was admitted to the ER for generalized convulsive status epilepticus. The patient was admitted to the ICU and we instigated mechanical ventilation under deep sedation with propofol. On admission to the ICU, the following laboratory results were found: albumin, 3.2 g/dl; total bilirubin, 1.1 mg/dl; AST, 44 U/L; ALT, 38 U/L; BUN, 14.7 mg/dl; and creatinine, 1.1 mg/dl. After titration, adequate depth of sedation was acquired at a rate of 3.5 mg/kg/h. The patient's urine changed to a green color 6 hours after the continuous infusion of propofol (Fig. 1B). Blood examination revealed a serum albumin level of 3.0 g/dl, total bilirubin level of 1.1 mg/dl, and direct bilirubin 0.5 mg/dl. Urinalysis revealed the following: pH, 6.0; urine SG, 1.015; bilirubin content, negative; and urobilinogen level, 0.2 EU/dl. Even before the urine culture results were available, we suspected propofol to be the cause of the green urine. The urine color returned to normal 3 hours after discontinuation of propofol. A repeat urinalysis showed: pH, 7.0; urine SG, 1.020; bilirubin content, negative; and urobilinogen level, 8.0 EU/dl. After 2 days, we confirmed the cessation of seizure activity and transferred the patient to the general ward.
Case 3
A 32-year-old female patient had an emergency splenectomy after a traffic accident. Because of bilateral multiple rib fractures and accompanying bilateral hemothorax and pneumothorax, we decided to maintain prolonged mechanical ventilation after the surgery. A controlled mechanical ventilation mode was selected because of possible respiratory muscle fatigue and ventilator fighting. Appropriate sedation was achieved via continuous infusion of propofol at a rate of 3 mg/kg/h, with remifentanil at 2 mcg/kg/h. The patient's urine became yellowish green 19 hours after continuous propofol infusion (Fig. 1C). Urinalysis revealed the following: pH, 6.0; urine SG, 1.015; bilirubin content, 1+; and urobilinogen level, 8.0 EU/dl. Urine culture was negative. As there were no signs of infection and no other known medication that could have discolored the urine, we suspected propofol as the cause. The urine color returned to normal 6 hours after discontinuation of propofol. The patient fully recovered after 2 weeks and was discharged from the ICU without further complications.
The main metabolic pathway of propofol is oxidation, reduction, and hydrolysis by cytochrome P450 and glucuronate conjugation in liver microsomes. Propofol exhibits a rapid distribution from the blood into tissue and a slow return from deep peripheral compartments back into the blood. Propofol is excreted in the urine after glucuroconjugation of the parent drug (to form the propofol-glucuronide) and sulfo- and glucuroconjugation of the hydroxylated metabolite to form 4-(2,6-diisopropyl-1,4-quinol)-sulphate, 1-, or 4-(2,6-diisopropyl-1,4)-glucuronide, respectively [1,2]. These quinol derivatives may be the cause of discoloration [3]. These derivatives do not reflect or alter renal function [4].
Urobilinogen, which is known to indicate liver parenchymal damage, was elevated in all 3 cases, as seen in previous reports [3,5]. This suggests that in a situation of dysfunction or functional decline of the liver, an extrahepatic pathway of propofol metabolism is augmented, resulting in the green coloration of the urine. As seen in case 1, changes in the pharmacokinetics may interfere with hepatic metabolism and may augment extrahepatic metabolism of propofol.
The total amount of infused propofol does not seem to be related to the induction of green urine (approximately 23500 mg in case 1, 4720 mg in case 2, and 2720 mg in case 3). Tan et al. [3] reported that even injection with 100 mg of propofol, could cause green discoloration of the urine. The length of the administration period does not seem to be related either. While, Blakey and Hixson-Wallace [4] reported that discoloration developed after 3 days of infusion, Tan et al. [3] reported that the urine showed discoloration in 1 hour of propofol administration. In the present cases, green urine was shown after 6-64 hours of continuous infusion.
In conclusion, the green discoloration of urine was related to the circumstances facilitating extrahepatic metabolism, rather than the amount of propofol administered or the duration of administration. Although green urine associated with propofol is benign and rare, prompt recognition of such side effects is important in limiting medical expenditures, inordinate drug exposure, and distress among patients and clinicians [4].
References
- 1.Simons PJ, Cockshott ID, Douglas EJ, Gordon EA, Hopkins K, Rowland M. Disposition in male volunteers of a subanaesthetic intravenous dose of an oil in water emulsion of 14C-propofol. Xenobiotica. 1988;18:429–440. doi: 10.3109/00498258809041679. [DOI] [PubMed] [Google Scholar]
- 2.Sneyd JR, Simons PJ, Wright B. Use of proton nmr spectroscopy to measure propofol metabolites in the urine of the female Caucasian patient. Xenobiotica. 1994;24:1021–1028. doi: 10.3109/00498259409043299. [DOI] [PubMed] [Google Scholar]
- 3.Tan CK, Lai CC, Cheng KC. Propofol-related green urine. Kidney Int. 2008;74:978. doi: 10.1038/ki.2008.139. [DOI] [PubMed] [Google Scholar]
- 4.Blakey SA, Hixson-Wallace JA. Clinical significance of rare and benign side effects: propofol and green urine. Pharmacotherapy. 2000;20:1120–1122. doi: 10.1592/phco.20.13.1120.35041. [DOI] [PubMed] [Google Scholar]
- 5.Lee YC, Lee JN, Bae JS, Park YC. Green urine in a patient who received a continuous infusion of propofol - A case report. Korean J Anesthesiol. 2009;56:325–327. doi: 10.4097/kjae.2009.56.3.325. [DOI] [PubMed] [Google Scholar]