

Abstract
During regular dissection classes, we came across tripled falx cerebelli in a male cadaver. The main (middle) falx cerebelli was large and was attached to the internal occipital crest. It contained the occipital sinus. There were two smaller folds (right and left), one on either side of the falx cerebelli. There were two aberrant venous sinuses; each one connecting the ipsilateral sigmoid and transverse sinuses with each other. The complex dural-venous variation reported here is seldom reported in the literature. Knowledge of such variation is important for neurosurgeons and neuroradiologists as these aberrant folds could cause haemorrhage during suboccipital approaches or may lead to erroneous interpretation during imaging of the posterior cranial fossa.
Keywords: falx cerebelli, dura mater, venous sinus, meninges
Implications for Practice
-
What is known about this subject?
Duplicated, fenestrated, small and complete absence are the reported variations of the falx cerebelli. Occurrence of triple falx cerebelli associated with two aberrant venous sinuses in the floor of the posterior cranial fossa is seldom reported in the literature.
-
What is the key finding in this case report?
Triple falx cerebelli associated with two aberrant venous sinuses in the infra-tentorial compartment of posterior cranial fossa.
-
What are the implications for future practice?
Knowledge of incidence of a rare complex dural-venous variation, reported here is important for neurosurgeons and neuroradiologists to avoid iatrogenic injuries during suboccipital approaches and erroneous interpretation during diagnostic and operative procedures in the posterior cranial fossa.
Background
The falx cerebelli is a small sickle-shaped fold of dura mater situated below the tentorium cerebelli. It projects forward into the posterior cerebellar notch. Occipital sinus is situated along its posterior attachment to the internal occipital crest.1 Variations in the morphology of the falx cerebelli are very rare. Duplicated, triplicated, fenestrated, small and complete absence are some of the reported variations of the falx cerebelli.2-7 The formations of dural venous sinuses are concurrent with the development of dural folds. Hence the duplicated falx cerebelli are usually associated with duplicated occipital sinus and occurrence of such cases has already been reported.3 The occurrence of triplicated falx cerebelli associated with an aberrant venous sinus in the floor of the posterior cranial fossa has been reported.3 Herein, we report a case of triple falx cerebelli associated with two aberrant venous sinuses in the infra-tentorial compartment of posterior cranial fossa. Knowledge of incidence of such rare complex dural-venous variation is important for neurosurgeons and neuroradiologists to avoid iatrogenic injuries during suboccipital approaches and erroneous interpretation during diagnostic and operative procedures in the posterior cranial fossa.3
Case details
During a regular dissection class for medical undergraduates, we came across a tripled falx cerebelli associated with two aberrant venous sinuses, in the floor of posterior cranial fossa. It was noted in a 55-year-old male cadaver of South Indian origin, which was donated to Manipal University, for the purpose of anatomical examination, medical education and research. While exposing the cranial cavity, the calvaria and brain were removed carefully. The tentorium cerebelli was reflected by cutting along its lateral border to expose the infra-tentorial compartment. The falx cerebelli was found to be triplicated (right, middle and left falces) (Figures 1 and 2). A corresponding triplication of the internal occipital crest was also noted (Figure 3). The length and width of all the three folds (right, middle and left falces) were measured. The distances between the two adjacent falces were also measured at the proximal, middle, and distal thirds. The length of the right, middle and left falces were 38mm, 44mm, and 36mm respectively. The width of the right, middle, and left falces were 3mm, 5mm, and 3mm, respectively. The distances between the right and middle falces were 3, 5, and 8mm at the proximal, middle, and distal thirds. The distances between the middle and left falces were 3, 4, and 8mm at the proximal, middle, and distal thirds.
Figure 1. Dissection of cranial cavity showing the infra-tentorial space. Note three distinct folds of falx cerebelli (F1: middle falx, F2: right falx, F3: left falx, TC: tentorium cerebelli).
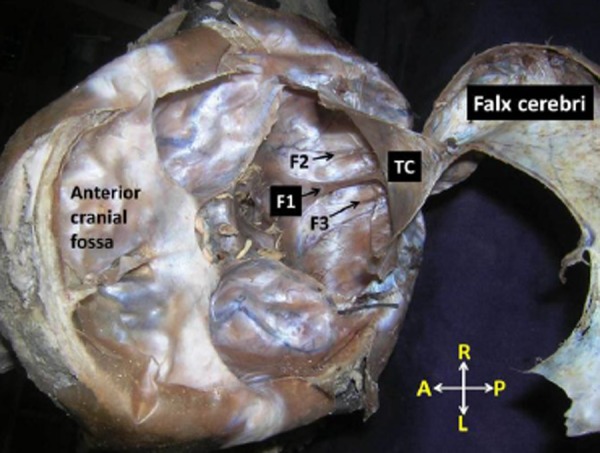
Figure 2. Closer view of dissection of cranial cavity showing the infra-tentorial space. Note three distinct folds of falx cerebelli (F1, F2 & F3). The right aberrant venous sinus (ras) connected the right sigmoid sinus (SS) with the ipsilateral transverse sinus. The left aberrant venous sinus (las) connected the left sigmoid sinus (SS) with the ipsilateral transverse sinus. (F1: middle falx, F2: right falx, F3: left falx, TC: tentorium cerebelli, PT: petrous part of the temporal bone).
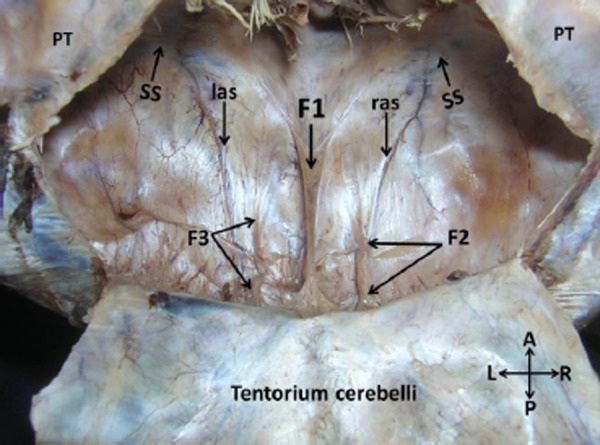
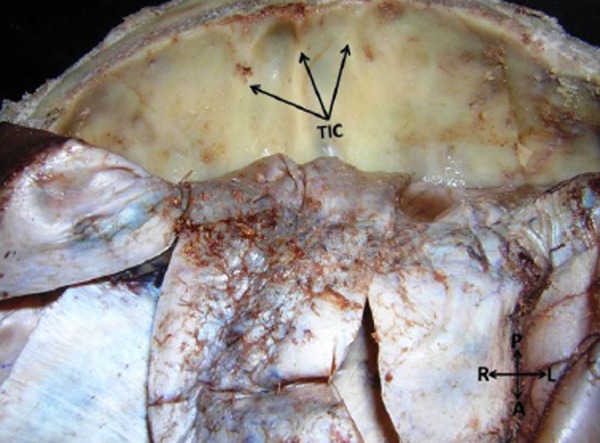
Figure 3. Photograph showing the triplicate internal occipital crest (TIC).
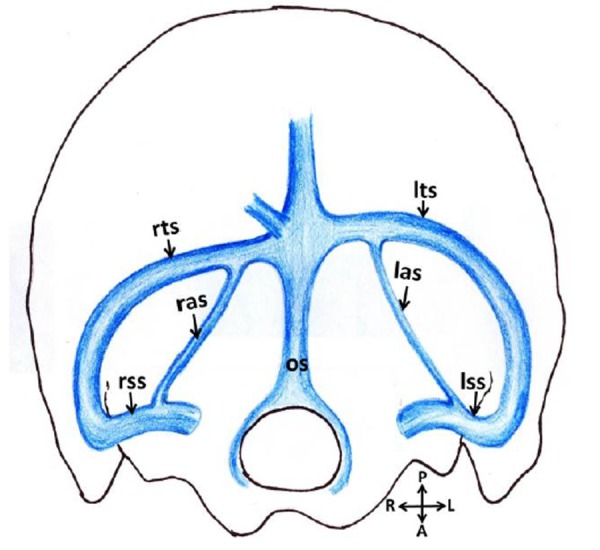
The main (middle) falx divided into two parts near the foramen magnum and there was only one occipital venous sinus in its posterior attachment. It terminated at the confluence of sinuses bilaterally. On each side of the middle falx cerebelli, at the floor of the posterior cranial fossa two aberrant dural venous sinuses were observed. The right aberrant venous sinus connected the right sigmoid sinus to ipsilateral transverse sinus. It travelled along the posterior margin of the right falx cerebelli to enter the ipsilateral transverse sinus. The left aberrant venous sinus connected the left sigmoid sinus to ipsilateral transverse sinus. It travelled along the left side of the left falx cerebelli (Figure1, 2 and 4).
Figure 4. Schematic picture showing the right and left aberrant venous sinuses, in the floor of the posterior cranial fossa. The right aberrant venous sinus (ras) connected the right sigmoid sinus (rss) with the right transverse sinus (rts). The left aberrant venous sinus (las) connected the left sigmoid sinus (lss) with the left transverse sinus (lts). (os: occipital sinus).
Discussion
The falx cerebelli is a sickle-shaped dural fold, which extends forward from the internal occipital crest into the posterior cerebellar notch and encloses the occipital venous sinus along its posterior margin. Usually, falx cerebelli is a single midline located structure, which may be divided inferiorly to create a V-shaped “vermian fossa”. The length of falx cerebelli usually lies between 2.8 and 4.5cm and it measures approximately 1–2 mm thick.2 The reported variations of falx cerebelli include its duplication, triplication, fenestration, and variation in dimensions or its total absence.2-7 Hassler andSchlenker5 have reported a case of duplicated falx cerebelli associated with an arachnoid cyst between the two falces. Shoja et al.2 have reported a case of duplicated falx cerebelli associated with two distinct occipital sinuses and internal occipital crests. A case of duplicated falx cerebelli associated with a constellation of other intracranial variations such as a Menelfe type 1 accessory middle cerebral artery; a duplicated anterior communicating artery and a persistent intracranial (olfactory) artery have also been reported.8 D’costa et al. have conducted a cadaveric study in which duplicated falx cerebelli was observed in 15.4% of cases. In their study, duplicated falx cerebelli was associated with two distinct occipital sinuses and internal occipital crests.9 In another case, Shoja et al.3 have reported the presence of triplicate falx cerebelli associated with single occipital venous sinus. In their case, among the three falces the left falx was very small and did not mention about the internal occipital crest. Contrary to previous reports, we observed three distinct falces and corresponding triplication of the internal occipital crest as well.
Formation of dural venous sinuses usually depends on the development of dural folds. Any changes in the morphology of the dural folds automatically results in the variations in the course or number of the dural venous sinuses.3 Duplication of falx cerebelli is frequently associated with formation of two distinct occipital sinuses. Occurrence of such cases has been reported in the past.2 Browder et al.10 have demonstrated that the doubling of occipital sinuses in adults may be due to the persistence of previously existing infant multi-channelled venous pathways in the midline suboccipital dura mater. However, they have not attempted to explain the genesis of duplication of the falx cerebelli. According to Lang,11 the occipital sinus may be tripled. In a cadaveric study, Knott12 has noted absence of the occipital sinus in two cases and a doubled sinus in nine cases, one lying on either side of a single internal occipital crest. In the present case, the triplicate falx cerebelli associated with a single occipital sinus, but the presence of two aberrant venous sinuses was noted in the floor of posterior cranial fossa. The case reported by Shoja et al. is somewhat similar to our case, but they have noted the presence of only one aberrant venous sinus.3 Incidence of such aberrant venous sinus in the infra-tentorial compartment of the posterior cranial fossa has seldom been reported. A study on posterior cranial fossa magnetic resonance venography of 211 paediatric patients did not reveal the presence of any such aberrant venous sinuses.13 It has been demonstrated that morphological alterations in the posterior cranial fossa dural sinuses are attributed to the development of the brain and that postural hemodynamic changes are induced by being erect.14 Evolution of aberrant venous structures in the foetus may affect cerebrovascular, brain or skull development.15 Knowledge of aberrant venous sinuses reported in the present case is important to prevent iatrogenic injuries during craniotomies of this region. Furthermore, calcification or ossification of the left and right falces might injure the cerebellum during rapid movements as in this instance they are directly in contact with the cerebellar hemisphere without a notch intervening.
To conclude, the complex dural-venous variation reported in the present case is seldom reported in the literature. Awareness of such variation is important for neurosurgeons and neuroradiologists as these could be a potential source of haemorrhage during suboccipital approaches, or may lead to erroneous interpretation during imaging of the posterior cranial fossa.
Footnotes
PEER REVIEW
Not commissioned. Externally peer reviewed.
CONFLICTS OF INTEREST
The authors declare that they have no competing interests.
CONSENT
The authors, Satheesha Nayak B, Srinivasa Rao Sirasanagandla, Deepthinath R, Naveen Kumar, declare that: This submission is compliant with the requirements of local research ethics committees.
Please cite this paper as: Satheesha Nayak B, Srinivasa Rao Sirasanagandla, Deepthinath R, Kumar N. Triple falx cerebelli associated with two aberrant venous sinuses in the floor of posterior cranial fossa. AMJ 2013, 6, 8, 397-400. http//dx.doi.org/10.4066/AMJ.2013.1740
References
- 1.Williams PL. 38th International edition. Edinburgh: Churchill Livingstone: 1999. Gray’s Anatomy. [Google Scholar]
- 2.Shoja MM, Tubbs RS, Khaki AA, Shokouhi G. A rare variation of the posterior cranial fossa: duplicated falx cerebelli, occipital venous sinus, and internal occipital crest. Folia Morphol (Warsz) 2006;65(2):171–173. [PubMed] [Google Scholar]
- 3.Shoja MM, Tubbs RS, Loukas M, Shokouhi G, Oakes WJ. A complex dural-venous variation in the posterior cranial fossa: a triplicate falx cerebelli and an aberrant venous sinus. Folia Morphol (Warsz) 2007;66(2):148–51. [PubMed] [Google Scholar]
- 4.Naidich TP, Pudlowski RM, Naidich JB, Gornish M, Rodriguez FJ. Computed tomographic signs of the Chiari II malformation. Part I: Skull and dural partitions. Radiology. 1980;134(1):65–71. doi: 10.1148/radiology.134.1.7350637. [DOI] [PubMed] [Google Scholar]
- 5.Hassler W, Schlenker M. Double falx cerebelli. Case report. Acta Neurochir (Wien) 1982;62(3-4):265–269. doi: 10.1007/BF01403633. [DOI] [PubMed] [Google Scholar]
- 6.Michaud J, Mizrahi EM, Urich H. Agenesis of the vermis with fusion of the cerebellar hemispheres, septooptic dysplasia and associated anomalies. Report of a case. Acta Neuropathol. 1982;56(3):161–166. doi: 10.1007/BF00690631. [DOI] [PubMed] [Google Scholar]
- 7.Tubbs Rs, Dockery SE, Salter G, Elton S, Blount JP, Grabb PA, Oakes WJ. Absence of the falx cerebelli in a Chiari II malformation. Clin Anat. 2002;15(3):193–195. doi: 10.1002/ca.10013. [DOI] [PubMed] [Google Scholar]
- 8.Shoja MM, Tubbs RS, Shokouhi GH, Ashrafian A, Oakes WJ. Abstract presented at the 23rd Annual Meeting of the American Association of Clinical Anatomists. Milwaukee, Wisconsin: 2006. A triple dural-venous variation in the posterior cranial fossa: A duplicated plus accessory falx cerebelli and an aberrant venous sinus. [Google Scholar]
- 9.D'Costa S, Krishnamurthy A, Nayak SR, Madhyasta S, Prabhu LV, Jiji P, Ranade AV, Pai MM, Vadgaonkar R, Ganesh Kumar C, Rai R. Duplication of falx cerebelli, occipital sinus, and internal occipital crest. Rom J Morphol Embryol. 2009;50(1):107–10. [PubMed] [Google Scholar]
- 10.Browder J, Kaplan HA, Krieger AJ. Venous lakes in the suboccipital dura mater and falx cerebelli of infants: surgical significance. Surg Neurol. 1975;4(1):53–55. [PubMed] [Google Scholar]
- 11.Lang J. Thieme: New York: 1991. Clinical anatomy of the posterior cranial fossa and its foramina; p. P.6. [Google Scholar]
- 12.Knott JF. On the cerebral sinuses and their variation. J Anat Physiol. 1881;16(Pt 1):27–42. [PMC free article] [PubMed] [Google Scholar]
- 13.Rollins N, Ison C, Booth T, Chia J. MR venography in the pediatric patient. Am J Neuroradiol. 2005;26(1):50–55. [PMC free article] [PubMed] [Google Scholar]
- 14.Okudera T, Huang YP, Ohta T, Yokota A, Nakamura Y, Maehara F, Utsunomiya H, Uemura K, Fukasawa H. Development of posterior fossa dural sinuses, emissary veins, and jugular bulb: morphological and radiologic study. Am J Neuroradiol. 1994;15(10):1871–1883. [PMC free article] [PubMed] [Google Scholar]
- 15.Reddy AT, Hedlund GL, Percy AK. Enlarged parietal foramina: association with cerebral venous and cortical anomalies. Neurology. 2000;54(5):1175–1178. doi: 10.1212/wnl.54.5.1175. [DOI] [PubMed] [Google Scholar]