

Abstract
Introduction: The aim of any root canal treatment is to achieve a canal free of micro organisms, residual pulp remnants, debris and smear layer for the long term success of the procedure. Manual and automated instrumentation techniques along with proper irrigation regime is used to arrive at the aforementioned goal. Many authors focused on the preparation capabilities of various manual and rotary instruments but very few investigators stressed on the actual cleaning abilities of these instruments.
Aims and objectives: This study was undertaken to evaluate the cleaning efficiency of manual K flex files and rotary Pro File systems in the root canals using a scanning electron microscope.
Material and Methods:Thirty single rooted mandibular first premolars were divided into two groups and randomized (the manual group-M and the ProFile group-P) with respect to the preparation technique. The Manual group was hand instrumented with stainless steel K- Flexofiles by means of a conventional filing technique. The Pro File group was instrumented according to the manufacturer's instructions using a rotary handpiece. All canals were shaped and cleaned under frequent irrigation with EDTA. Final irrigation was carried out with 3 mL of normal saline solution to neutralize the action of the irrigant. The roots were split, one half of each tooth was selected for further SEM technique analysis and examined under the scanning electron microscope. The canal walls were quantitatively evaluated for the amount of debris and smear layer. The apical, middle and coronal regions of the canal surface, were graded (1-5) for debris and smear layer. A statistical analysis was performed using a Mann-Whitney Rank Sum test. ProFile performed least effective cleaning. Manual K-Flexofiles led to a grooved pattern.
Results and Conclusion: A statistically significant difference was observed (p<0.05) between the two instrumentation techniques concerning the amount of debris and smear layer at the apical level. The manually filed canals had less debris and smear layer than those using a rotary technique. It was concluded from this study that none of the instrumentation techniques employed, produced the canal walls which were free of surface debris and smear layer. The manual instrumentation technique was better in cleaning the canals compared to the ProFile rotary Ni-Ti instruments despite the step-back technique used for manual instrumentation.
How to cite this article: Manjunatha M, Kini A, Sudhakar V, Sunil K V C, Hiremath V K, Shah A. Smear Layer Evaluation on Root Canal Preparation with Manual and Rotary Techniques using EDTA as an Irrigant: A Scanning Electron Microscopy Study. J Int Oral Health 2013; 5(1):66-78.
Keywords: : Clinical research, Tooth loss, Oral Health
Introduction
The main objectives of cleaning and shaping of root canal is to eliminate residual pulp tissue, removal of debris and the maintenance of the original canal curvature. Based on the evidence of several studies on the instrumented canals, it was found that it is difficult to completely clean the root canals, especially the curved ones.1,2,3,4
Removal of smear layer prior to root canal obturation remains controversial. It has been suggested that the smear layer may decrease the permeability of dentin and prevent bacterial penetration into underlying dentinal tubules.5 Most of the authors believe that the smear layer may prevent antimicrobial agents from gaining access to underlying contaminated dentinal tubules.6,7
Several studies have indicated that cleaning ability of manual root-canal instrumentation is found to be superior to automated devices.3,8,9 However, certain studies have shown superiority of automated devices using rotary nickel-titanium instruments with various tapers, even in severely curved root canals.
Since most of the studies conducted focused little on the cleaning ability of the rotary Ni-Ti instruments, this study was undertaken for a comparative evaluation of the cleaning ability of rotary Ni-Ti instrumentation technique and manual instrumentation technique using scanning electron microscope.
Aims and Objectives:
Compare the cleanliness of the root canal walls either with the manual technique and rotary technique of canal instrumentation.
Check the amount of debris and smear layer present on the canal walls at the cervical, middle and apical thirds after hand instrumentation or a rotary technique of instrumentation.
Materials and Methods:
Thirty single rooted mandibular first premolars which were extracted for orthodontic reasons were selected. Following extraction, the teeth were rinsed in tap water in order to remove blood and tissue debris, stored in 0.2% Chlorhexidine Gluconate till usage. Access cavities were prepared according to the standard extension for optimal inspection of root canal openings.
The teeth were divided into two groups and randomized (the manual group-M and the ProFile group-P) with respect to the preparation technique. The Manual group was hand instrumented with stainless steel K- Flexofiles by means of a conventional filing technique, i.e. the canal was enlarged along its entire length. The instruments were inserted to the working length (WL), twisted or bound and withdrawn by forcing them against the walls. Working length was determined with a size 10 K- File, which was inserted until it reached the apical foramen and one-half millimeter subtracted from this length. Filing motions were repeated until that particular size file was loose.10 This was repeated successively with larger instruments of sizes 15-35.
The ProFile group was instrumented with rotary Ni-Ti files in a 250- r.p.m. handpiece to size 35 (.06). The instruments were used in the canal with a continuous, slight in and out passive movement with intermittent irrigation with EDTA and were never forced apically. The operation sequence comprised four phases: 1) crown-down, 2) determination of the working length, 3) apical preparation and 4) final shaping.
The protocol was as follows:
For crown-down preparation the instruments 25.06 and 20.06 were introduced successively at 250 r.p.m. into the canal until resistance was perceived by the operator or approximately half to possibly two-thirds of the length of the estimated canal.
Canal preparation proceeded using the 25.04 and 20.04 instruments in a similar way but not beyond three-quarters of the estimated canal length. The optimal depth of the root canal (Working Length) was determined by inserting a size 10 K- File until it reached the apical foramen and subtracting one- half millimeter from this length.
The apical stop at the working length was created using 15.04, 20.04, 25.04 instruments.
The final shaping achieved to working length was performed successively by means of 20.06, 25.06, 30.06, 35.06 instruments.
All canals were shaped and cleaned under frequent irrigation with EDTA. Final irrigation was carried out with 3 ml of normal saline solution to neutralize the action of the irrigant. All canals were dried with sterile adsorbent paper points.
The roots were split using a tapering fissure diamond bur cutting a groove in a longitudinal direction. To avoid contamination of the canals by the separation process, the last part of the separation was performed by splitting the root with a chisel. The root halves were cleaned from grinding material and dried using water- and air-blasting for three seconds. One half of each tooth was selected for further SEM technique analysis. The criteria for use were that the root canal wall should be intact and available for quantitative measurements at apical, middle and coronal level.
The criteria for use were that the root canal wall should be intact and available for quantitative measurements at apical, middle and coronal level. The specimens were left to dry overnight. The root sections were mounted on aluminium stub, sputter-coated with 10% gold-palladium in the sputtering machine (JFC-1100E, Ion Sputtering Device) and examined under the scanning electron microscope (JEOL, JSM-840 A Scanning Microscope, Tokyo, Japan).
The entire surface and each region (apical, middle and coronal) of each canal were examined at a magnifications ranging from x12 to x1500. The micrographs depicting a magnification x200 were chosen for the analysis.
The canal walls were quantitatively evaluated for the amount of debris and smear layer.
Debris was defined as dentine chips, pulpal remnants or other particles loosely stuck to the canal wall.3
Debris were scored as follows
Score 1: clean root canal wall, very slight debris (photograph 1)
Photograph 1: Photomicrograph Showing Debris-Score 1.

Score 2: slight debris (photograph 2)
Photograph 2: Photomicrograph Showing Debris-Score 2.

Score 3: moderate amount of debris, less than 50% of the sample surface covered (photograph 3)
Photograph 3: Photomicrograph Showing Debris-Score 3.

Score 4:substantial debris, more than 50% of the sample surface covered (photograph 4)
Photograph 4: Photomicrograph Showing Debris-Score 4.

Score 5: the root canal sample was completely or almost completely covered with debris (photograph 5)
Photograph 5: Photomicrograph Showing Debris-Score 5.
Smear layer3 was scored as follows
Score 1: no smear layer, open dentinal tubuli (photograph 6)
Photograph 6: Photomicrograph Showing Smear Layer - Score 1.

Table 1: Scores of Debris and Smear Layer Recorded.
| M- GROUP | P- GROUP | ||||||||
| Scores | Cervical | Middle | Apical | Cervical | Middle | Apical | |||
| Debris | |||||||||
| 1 | 4 | - | - | 3 | 3 | - | |||
| 2 | 9 | 12 | 7 | 6 | 6 | - | |||
| 3 | 2 | 3 | 4 | 6 | 6 | 8 | |||
| 4 | - | - | 2 | - | - | 4 | |||
| 5 | - | - | 2 | - | - | 3 | |||
| Smear layer | |||||||||
| 1 | 6 | - | - | 5 | 2 | - | |||
| 2 | 8 | 9 | 5 | 10 | 7 | - | |||
| 3 | 1 | 6 | 5 | - | 6 | 5 | |||
| 4 | - | - | 4 | - | - | 7 | |||
| 5 | - | - | 1 | - | - | 3 | |||
| n=15 | |||||||||
Score 2: slight smear layer, most tubuli were open (photograph 7)
Photograph 7: Photomicrograph Showing Smear Layer - Score 2.

Score 3: homogeneous smear layer covering the major part of the surface, a few dentinal tubuli open (photograph 8)
Photograph 8: Photomicrograph Showing Smear Layer - Score 3.

Score 4:homogeneous smear layer covering the surface, no dentinal tubuli open (photograph 9)
Photograph 9: Photomicrograph Showing Smear Layer - Score 4.

Score 5: thick non-homogeneous smear layer covering the surface (photograph 10)
Photograph 10: Photomicrograph Showing Smear Layer - Score 5.

Central beam of SEM was directed to the centre of the object by the SEM- operator under x12 magnification and the magnification was increased gradually to x1500. The canal wall region appearing on the screen at x200 magnification was scored. The scoring was done by a second operator who could not identify the coded specimens nor the device used for root canal preparation. The second operator was trained in the scoring procedure, resulting in a sufficient intra observer reproducibility.3
The apical, middle and coronal regions of the canal surface, were graded (1-5) for debris and smear layer, assessed and recorded. A statistical analysis was performed using a Mann-Whitney Rank Sum test. In addition, a comparison between the scores of the Manual and Pro File groups for smear layer and debris was made to determine possible differences in the effectiveness of the two techniques employed.
Discussion
Removal of vital and/or necrotic pulp tissue, infected dentin, and dentin debris are the important objectives during root-canal instrumentation. This procedure is important in order to eliminate most of the microorganisms from the root canal system.
The smear layer is a surface film of a thickness of approximately 1-2 μ which remains on the root canal wall after instrumentation.11 Smear layer is absent on areas that are not instrumented. Smear layer contains both organic and inorganic components i.e. residual vital or necrotic pulp tissue, dentin particles, protein agglomerates, bacterial components, blood cells along with retained irrigants, which blocks up the openings of the dentinal tubuli. In this way, a thick and non-homogeneous smear layer can prevent effective removal of intracanal microorganisms, and complete sealing of the root canal.12,13
In this investigation, hand instrumentation was performed with K-Flexofiles made of stainless steel. These instruments utilize a triangular blank as used for reamer with the flutes twisted more tightly to give more cutting edges but maintaining the same narrow cross-sectional diameter for increased flexibility.14 They feature a non-cutting tip15,16 and they were included in the investigation because it was known on the basis of earlier investigation that they are able to enlarge, even severely curved canals with little or no transportation.17 In a study of the machining efficiency of various Ni-Ti and stainless steel files reported that the most efficient of those examined were Ni-Ti instruments and Flexofiles. They attributed their findings to the increased flexibility of these two instruments together with their 'aggressive' cutting designs.18
Although it is recommended to use antibacterial irrigants along with chelating agents in order to remove debris and inorganic/organic smear layer,3,12,19 in the present study EDTA was used as an irrigant owing to its chelating properties on inorganic component.7 But, it is not possible to completely remove the smear layer with EDTA.20,21,22,23 Recently, the paste type chelators containing EDTA have regained popularity to be used with Ni-Ti instruments, manufacturers recommend their use as a lubricant during rotary root canal preparation, to reduce the risk of instrument separation.24 Nevertheless, the major objective of the present investigation was to solely compare the cleaning effectiveness of the two instrumentation techniques under similar conditions. To avoid any association of different irrigation solutions, a simple irrigation technique was used. Hence, it has to be considered that the cleaning efficiency of the two instrumentation techniques evaluated in the present study might be further improved using a combination of NaOCl and EDTA.
The SEM technique produces images of high resolution and magnification. Apical, middle and coronal sites for quantitative measurements were chosen at random. On those occasions when unprepared surfaces were found, a new site was chosen for micrographic examination. The magnification 200x was employed because it offered a wider view and also a detailed image of the surface. The micrographs at x1500 magnification might cover too small a surface, give limited information and lead to a potential misrepresentation of cleanliness.25 One weakness of the evaluation of the micrograph was that the measurements of debris and smear layer were arbitrary and at best ordinal in nature. However, there is currently no consensus in the standardization of measurements of debris and smear layer.26,27
Apical extrusion of the material was observed during the manual instrumentation, which is consistent with earlier studies.28,29,30However this problem was not evaluated, considering the low frequency of exacerbation during clinical endodontic work; this in vitro observation may not be relevant in the clinical situations.
In the present study, the cleaning efficacy of two instrumentation methods was examined by means of an SEM evaluation of the coronal, middle and the apical portions of the canals.3,4,27,31,32,33,34 on the basis of a separate numerical evaluation scheme for debris and smear layer. Partially un-instrumented areas with remaining debris were found in all canal sections, with both instrumentation techniques. This finding has also been supported by other authors.1,2,3,9,27,32,33,35,36,37
Using stainless steel K-Flexofiles resulted in no significant differences in the amount of debris and smear layer compared to the ProFile instruments at the cervical and middle thirds of the canals (Tables 2,3,4,5 Graphs 1,2,3,4 p>0.05).
Table 2: Mean Score of Debris at the Cervical Level among the Study Group.
| Experiment | Mean ± SD | 'U' Statistics | Significance |
| M- Group | 1.87 ±0.64 | 84.00 | p> 0.05 |
Table 3: Mean Score of Smear Layer at the Cervical Level among the Study Group.
| Experiment | Mean ± SD | 'U' Statistics | Significance |
| M- Group | 1.67 ±0.62 | 110.00 | p> 0.05 |
| P- Group | 1.67 ±0.49 | ||
| P- Group | 2.20 ±0.77 |
Table 4: Mean score of Debris at the Middle Level among the Study Group.
| Experiment | Mean ± SD | 'U' Statistics | Significance |
| M- Group | 2.20 ±0.41 | 108.00 | p> 0.05 |
| P- Group | 2.20 ±0.77 |
Table 5: Mean Score of Smear Layer at the Middle Level among the Study Group.
| Experiment | Mean ± SD | 'U' Statistics | Significance |
| M- Group | 2.40 ±0.51 | 103.50 | p> 0.05 |
| P- Group | 2.27 ±0.70 |
Graph 1:Mean Cervical Debris Score among the Study Group.

Graph 2:Mean Cervical Smear Layer Score among the Study Group.

Graph 3:Mean Middle Debris Score among the Study Group.

Graph 4:Mean Middle Smear Layer Score among the Study Group.

Edgar Schafer et al. (2000) compared the efficacy of manual and automated instruments. The results indicated that stainless steel hand K-Flexofiles performed better than ProFile rotary Ni-Ti instruments.31
In a study by E.Schafer and R.Schlingemann (2001) to check the efficacy of rotary Ni-Ti K3 instruments and stainless steel hand K-Flexofile, the results indicated that Flexofiles allowed significantly better removal of debris than K3 instruments.33
M.Ahlquist et al. (2001) checked the effectiveness of stainless steel S-files and ProFile rotary Ni-Ti files in cleaning of root canals and they found stainless steel S-files produced cleaner root canal walls.
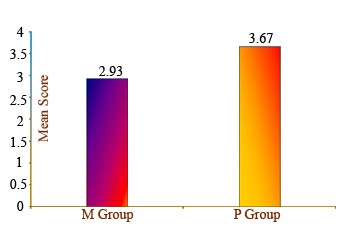
The results of the evaluation of the apical third of the specimens for debris and smear layer in this study showed statistically significant differences (p<0.05) between both the systems (Tables 6, 7 Graphs 5, 6). The manual group showed better cleaning ability with respect to the remaining debris and smear layer than ProFile group. Similar results were obtained by M.Ahlquist et al.(2001) when they compared stainless steel S-files and ProFile rotary Ni-Ti files.27
Table 6: Mean Score of Debris at the Apical Level among the Study Group.
| Experiment | Mean ± SD | 'U' Statistics | Significance |
| M- Group | 2.93 ±1.10 | 63.00 | p< 0.05* |
| P- Group | 3.67±0.82 | ||
| * Statistically significant | |||
Table 7: Mean Score of Smear Layer at the Apical Level among the Study Group.
| Experiment | Mean ± SD | 'U' Statistics | Significance |
| M- Group | 3.07 ±0.96 | 60.00 | p< 0.05* |
| P- Group | P- Group | ||
| * Statistically significant | |||
Graph 5:Mean Apical Debris Score among the Study Group.
Graph 6:Mean Apícal Smear Layer Score among the Study Group.

The results of the present study indicate that on an average the apical third of the canals was less clean than the middle and coronal thirds regardless of the instrument used. This observation is also in agreement with other studies. The results of E.Schafer and D.Lohmann (2002) comparing rotary instrumentation and stainless steel hand K-Flexofile showed that completely cleaned root canals were not found with any of the two instruments.32
In a SEM study of debris and smear layer remaining following use of GT rotary instruments by G.Gambarini and J.Laszkiewicz (2002), the results showed that GT rotary instruments removed debris effectively, but left root canal walls covered with smear layer particularly in the apical third.38
F.Heard and R.E.Walton (1997) in their SEM study to compare four root canal preparation techniques found the middle level was cleaner than the apical or coronal levels.39
M.Hulsmann et al. (1997) compared the canal cleanliness after the preparation with eight different instrumentation techniques including both engine driven and hand. They found best cleaning ability achieved at the middle and cervical thirds.3
The results of some investigations were not in agreement with the above. M.F.Bertrand et al.(1999) in the comparative study of removal of smear layer using the Quantec Series 2000 and stainless steel hand K-files found that Quantec rotary system produced cleaner canal walls than conventional manual instruments, particularly in the middle and apical thirds.40
In the present study, overall performance of the hand instrumentation was better than rotary Ni-Ti despite the step-back technique used for hand instrumentation group. The reason may be the ability to clean effectively the endodontic space is dependent on both instrumentation and irrigation.38 The dentin filing using mechanical endodontic devices is more extensive than manual instrumentation and the amount of dentinal shavings produced is, therefore, higher.21 It can be concluded that obviously, even different rotary Ni-Ti instruments vary in their debris removal efficiency, possibly due to their flute design.19,40,41
ProFile instruments have U-shaped blades with radial lands and it has been shown that this file design was less efficient in debris removal. They perform a planing action, compared to rotary instruments having a positive rake angle which could be the main reason for the inferior cleaning ability.4,31
It was also observed that the cleaning ability was inferior in the apical third of the canals when compared to the middle and cervical third. The reason for the incomplete removal may be an irregular secondary dentin which is associated with the physiological ageing of the Root42 so that surface morphology, especially in the apical region, is far from smooth, which is generally advocated in endodontics to be typical of the normal or well-debrided canal wall.35 The incomplete removal of debris and smear layer in the apical third may be due to the failure of irrigants to reach the apical third.
During endodontic instrumentation of root canals, products containing EDTA are used to remove/reduce smear layer and debris, thereby creating better access for disinfectants as well as achieving a clean surface for the final seal of the root canal. Two different instrumentation techniques with EDTA as irrigant were used in the study to assess the effective cleanliness. The manual technique employed in the present study produced cleaner root canal walls than ProFile rotary technique. The subjective estimation was that rotary instrumentation technique employed was faster and was less tiring for the operator.
Summary and Conclusion
Summary
The aim of this study was to evaluate the cleanliness of the root canal walls after preparation with ProFile rotary Ni-Ti and hand instruments.
ProFile rotary Ni-Ti instruments and K- Flexofiles were utilized to prepare the canals with EDTA as an irrigant. After the preparation of the canals the specimens were split longitudinally and observed under scanning electron microscope (SEM), to quantitatively evaluate the amount of remaining debris and smear layer using a numerical scoring system.
The results of the present study confirm the results of previous studies on rotary Ni-Ti systems concerning the cleaning ability. Both systems were ineffective in removing debris and smear layer completely and K- Flexofiles were better in removing the debris and smear layer compared to ProFile rotary Ni-Ti instruments especially in the apical third.
It can be concluded from this study that none of the instrumentation techniques employed, produced the canal walls which were free of surface debris and smear layer. The manual instrumentation technique was better in cleaning the canals compared to the ProFile rotary Ni-Ti instruments despite the step-back technique used for manual instrumentation. Had a crown-down technique been used for manual instrumentation, it would have removed the debris more effectively and produced better canal walls. During endodontic instrumentation of root canals, alternating irrigation with 5.25% NaOCl and 15% EDTA should be used to remove/reduce smear layer and debris, thereby creating better access for disinfectants as well as achieving a clean surface for the final seal of the root canal.
Even though the manual technique employed in the present study produced cleaner root canal walls than the ProFile rotary technique, the latter method appeared to be less time consuming in preparation of the root canal space and less tiring for the operator.
Conclusion
K- Flexofiles were better in debris and smear layer removal compared to ProFile rotary Ni-Ti instruments.
No statistically significant differences were observed in the cleaning ability of the two instrumentation techniques at the cervical and middle thirds of the canals.
Statistically significant differences were observed with respect to the remaining debris and smear layer at the apical level.
Footnotes
Source of Support: Nil
Conflict of Interest: None Declared
Contributor Information
M Manjunatha, Bhabha College of Dental Sciences, Bhopal, Madhya Pradesh, India.
Kini Annapurna, Rajarajeshwari Dental College, Bangalore, India.
V Sudhakar, Mansarovar Dental college and Hospital, Bhopal, Madhya Pradesh, India.
VC Sunil Kumar, Bhabha College of Dental Sciences, Bhopal, Madhya Pradesh, India.
Vinay Kumar Hiremath, Mansarovar Dental College and Hospital, Bhopal, Madhya Pradesh, India.
Ankur Shah, Aditya Dental College, Beed, Maharastra, India.
References
- 1.Bolanos OR, Jensen JR. Scanning Electron Microscopic comparisons of the efficacy of various methods of root canal preparation. J Endod. 1980;6:815–822. doi: 10.1016/S0099-2399(80)80034-3. [DOI] [PubMed] [Google Scholar]
- 2.Haikel Y, Allemann C. Effectiveness of four methods for preparing root canals; a scanning electron microscopic evaluation. J Endod. 1988;14:340–345. doi: 10.1016/S0099-2399(88)80195-X. [DOI] [PubMed] [Google Scholar]
- 3.Hulsmann M, Rummelin C, Schafers F. Root canal cleanliness after preparation with different endodontic handpieces and hand instruments; a comparative scanning electron microscopy investigation. J Endod. 1977;23:301–306. doi: 10.1016/S0099-2399(97)80410-4. [DOI] [PubMed] [Google Scholar]
- 4.Versumer J, Hulsmann M, Schafers F. A comparative study of root canal preparation using ProFile .04 and Lightspeed rotary Ni-Ti instruments. Int Endod J. 2002;35:37–46. doi: 10.1046/j.1365-2591.2002.00454.x. [DOI] [PubMed] [Google Scholar]
- 5.Pashley DH, Michelich V, Kehl T. Dentin permeability; effects of smear layer removal. J Prosthet Dent. 1981;46:531–537. doi: 10.1016/0022-3913(81)90243-2. [DOI] [PubMed] [Google Scholar]
- 6.Chirnside LM. The bacteriological status of dentine around infected pulp canals. N Z Dent J. 1958;54:173–183. [Google Scholar]
- 7.Shovelton DS. The presence and distribution of microorganisms within nonvital teeth. Br Dent J. 1964;117:101–107. [Google Scholar]
- 8.Mizrahi SJ, Tucker JW, Seltzer S. A scanning electron microscopic study of the efficacy of various endodontic instruments. J Endod. 1975;1:324–333. doi: 10.1016/s0099-2399(75)80012-4. [DOI] [PubMed] [Google Scholar]
- 9.Schwarze T, Geurtsen W, editors. Comparative qualitative scanning electron microscopic study of automated vs. hand instrumentation of root canals. Dtsch Zahnarztl Z. 1996;51:227–230. [Google Scholar]
- 10.Walton RE. Histologic evaluation of different methods of enlarging the pulp canal space. J Endod. 1976;2:304–311. doi: 10.1016/S0099-2399(76)80045-3. [DOI] [PubMed] [Google Scholar]
- 11.American Association of Endodontists. 6. Chicago III, USA: 1998. American Association of Endodontists. Glossary Contemporary Terminology for Endodontics. [Google Scholar]
- 12.West JD, Roane JB, Goerig AC. Pathways of the Pulp. In: Cohen S, Burns RC, editors. Mosby Year Book. 6. Boston, MA, USA: 1994. pp. 179–218. [Google Scholar]
- 13.Petschelt A, Stumpf B, Roab W. Tightness of root canal sealers with and without smear layer. Dtsch Zahnarztl Z. 1987;42:743–746. [PubMed] [Google Scholar]
- 14.Franklin S, Weine . Intracanal treatment procedures, Basic and advanced topics. In: Franklin S, Weine, editors. Endodontic Therapy. 6. Mosby: 2004. p. 208. [Google Scholar]
- 15.Larz Spanberg. Instruments, Materials and Devices. In: Cohen S, Burns RC, editors. Pathways of the pulp. 8. St. Louis, Mosby: 2002. p. 530. [Google Scholar]
- 16.John I Ingle, Leif K Bakland, Donald L Peters, Buchnan L Stephen, Thomas P Mullamy. Endodontic Cavity Preparation. In: John I Ingle, Leif K Bakland., editors. Endodontics. 4. 1994. p. 168. [Google Scholar]
- 17.Joachim Tepel, dent Dr. med., Edgar Schafer, Hoppe Wolfgang. Properties of endodontic hand instruments used in rotary motion. J Endod. 1995;8:418–421. doi: 10.1016/S0099-2399(06)80828-9. [DOI] [PubMed] [Google Scholar]
- 18.Camps JJ, Pertot WJ. Machining efficiency of Ni-Ti K-type files in a linear motion. Int Endod J. 1995;28:279–284. doi: 10.1111/j.1365-2591.1995.tb00316.x. [DOI] [PubMed] [Google Scholar]
- 19.Gambarini G. Shaping and cleaning of root canal system; a scanning electron microscopic evaluation of a new instrumentation and irrigation technique. J Endod. 1999;25:800–803. doi: 10.1016/S0099-2399(99)80300-8. [DOI] [PubMed] [Google Scholar]
- 20.Sen BH, Wesselink PR, Turkun M. The smear layer; a phenomenon in root canal therapy. Int Endod J. 1995;28:141–148. doi: 10.1111/j.1365-2591.1995.tb00289.x. [DOI] [PubMed] [Google Scholar]
- 21.Liolios E, Economides N, Parissis-Messimeris S, Boutsioukis A. The effectiveness of three irrigating solutions on root canal cleaning after hand and mechanical preparation. Int Endod J. 1997;30:51–57. doi: 10.1111/j.1365-2591.1997.tb01098.x. [DOI] [PubMed] [Google Scholar]
- 22.O'Conell Michael S, Leslie A Morgan, J Beeler William, Baumgartner J Craig. A comparative study of smear layer removal using different salts of EDTA. Int Endod J. 2000;12:739–743. doi: 10.1097/00004770-200012000-00019. [DOI] [PubMed] [Google Scholar]
- 23.Baumgartner J Craig, L Mader Carson. A scanning electron microscopic evaluation of four root canal irrigation regimens. J Endod. 1987;4:147–157. doi: 10.1016/s0099-2399(87)80132-2. [DOI] [PubMed] [Google Scholar]
- 24.Hulsmann M, Heckendoroff M, Lennon A. Chelating agents in root canal treatment; mode of action and indications for their use. Int Endod J. 2003;36:810–830. doi: 10.1111/j.1365-2591.2003.00754.x. [DOI] [PubMed] [Google Scholar]
- 25.Mandel E, Machtou P, Friedman S. Scanning electron microscopic observations of canal cleanliness. J Endod. 1990;6:279–283. doi: 10.1016/S0099-2399(06)81630-4. [DOI] [PubMed] [Google Scholar]
- 26.Jeon In- Soo, Spangberg Larz SW, Yoon Tai- Cheol, Reza B, Kazemi, Kum Kee- Yeon. Smear layer production by three rotary reamers with different cutting blade designs in straight root canals; a scanning microscopy study. Oral Surg Oral Med Oral Pathol Oral Radiol, Endod. 2003;96:601–607. doi: 10.1016/s1079-2104(03)00303-2. [DOI] [PubMed] [Google Scholar]
- 27.Ahlquist M, Henningsson O, Hultenby K, Ohlin J. The effectiveness of manual and rotary techniques in the cleaning of root canals; a scanning electron microscopy study. Int Endod J. 2001;34:533–537. doi: 10.1046/j.1365-2591.2001.00429.x. [DOI] [PubMed] [Google Scholar]
- 28.Martin H, Cunningham WT. The effect of endosonic and hand manipulation on the amount of root canal material extruded. Oral Surg Oral Med Oral Pathol. 1982;53:611–613. doi: 10.1016/0030-4220(82)90350-4. [DOI] [PubMed] [Google Scholar]
- 29.Tucker DM, Wenckus CS, Bentkover SK. Canal wall planing by engine-driven Ni-Ti instruments, compared with stainless steel hand instruments. J Endod. 1997;3:170–173. doi: 10.1016/S0099-2399(97)80269-5. [DOI] [PubMed] [Google Scholar]
- 30.Reddy S, Hicks ML, editors. Apical extrusion of debris using two hand and two rotary instrumentation techniques. J Endod. 1998;3:180–183. doi: 10.1016/S0099-2399(98)80179-9. [DOI] [PubMed] [Google Scholar]
- 31.Schafer E, Zapke K. A comparative scanning electron microscopic investigation of the efficacy of manual and automated instrumentation of root canals. J Endod. 2000;26:660–664. doi: 10.1097/00004770-200011000-00007. [DOI] [PubMed] [Google Scholar]
- 32.Schafer E, Lohmann D. Efficiency of rotary Ni-Ti FlexMaster instruments compared with stainless steel hand K-Flexofile-Part 2. Cleaning effectiveness and instrumentation results in severely curved root canals of extracted teeth. Int Endod J. 2002;35:514–521. doi: 10.1046/j.1365-2591.2002.00515.x. [DOI] [PubMed] [Google Scholar]
- 33.Schafer E, Schlingemann R. Efficiency of rotary Ni-Ti K3 instruments compared with stainless steel hand K-Flexofile. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J. 2003;36:208–217. doi: 10.1046/j.1365-2591.2003.00644.x. [DOI] [PubMed] [Google Scholar]
- 34.Hulsmann M, Herbst U, Scharers F. Comparative study of root-canal preparation using Lightspeed and Quantec SC rotary Ni-Ti instruments. Int Endod J. 2003;36:748–756. doi: 10.1046/j.1365-2591.2003.00725.x. [DOI] [PubMed] [Google Scholar]
- 35.Bechelli C, Orlandini S Zecchi, Colafranceschi M. Scanning Electron Microscopy study on the efficacy of root canal wall debridement of hand versus Lightspeed instrumentation. Int Endod J. 1999;32:484–493. doi: 10.1046/j.1365-2591.1999.00250.x. [DOI] [PubMed] [Google Scholar]
- 36.Kochis KA, Walton RE, Lilly JP, Ricks L, Rivera EM. A histologic comparison of hand and Ni-Ti rotary instrumentation techniques. J Endod. 1998;24:286. [Google Scholar]
- 37.Park JW, TS BH, Lee JY. Scanning electron microscopic evaluation of the prepared root canal surface by hand and rotary instruments. J Endod. 1998;24:293. [Google Scholar]
- 38.Gambarini G, Laszkiewicz J. A scanning electron microscopy study of debris and smear layer remaining following use of GT rotary instruments. Int Endod J. 2002;35:422–427. doi: 10.1046/j.1365-2591.2002.00495.x. [DOI] [PubMed] [Google Scholar]
- 39.Heard F, Walton R.E. Scanning Electron Microscopy study comparing four root canal preparation techniques in small curved canals. Int Endod J. 1997;30:323–331. doi: 10.1046/j.1365-2591.1997.00090.x. [DOI] [PubMed] [Google Scholar]
- 40.Bertrand MF, Pizzardini P, Muller M, Medioni E, Rocca JP. The removal of smear layer using the Quantec system. A study using Scanning Electron Microscope. Int Endod J. 1999;32:217–224. doi: 10.1046/j.1365-2591.1999.00231.x. [DOI] [PubMed] [Google Scholar]
- 41.Hulsmann M, Versummer J, Schade M. A comparative study of Lightspeed, ProFile .04, Quantec and HERO 642. Int Endod J. 2000;33:150. [Google Scholar]
- 42.Sen BH, Wesselink PR, Turkun M. The smear layer; a phenomenon in root canal therapy. Int Endod J. 1995;28:141–148. doi: 10.1111/j.1365-2591.1995.tb00289.x. [DOI] [PubMed] [Google Scholar]