

Abstract
Context:
The concerns of caregivers of patients with neurological disorders have been a felt need for a long time, with many of them experiencing significant psychiatric morbidity.
Aims:
This study aimed to find the effect of yoga in reducing anxiety and depression, as well as improving quality-of-life in caregivers of patients with neurological disorders.
Settings and Design:
The study was conducted using a randomized controlled design, with yoga intervention and waitlisted controls.
Methodology:
Sixty consenting caregivers of inpatients in neurology wards were randomized into two groups: Yoga and control. Demographic variables except years of education and length of caretaking were comparable in the two groups, as also baseline scores of anxiety, depression and quality-of-life. A specific yoga module comprising yogāsanas, prāṇāyāma, and chanting was taught to the participants in the yoga group by the researcher. At follow-up 43 patients (yoga n=20 and control group n=23) were available. Two-way repeated measures analysis of variance was used to test the change from pre-test to post-test scores within and between groups. Analysis of covariance was performed to compare the post-test scores between the groups adjusting for education and length of caretaking.
Results:
Following one month intervention of yoga therapy, there was a significant (P<0.001) decrease in anxiety and depression scores, as well as improved quality-of-life among the participants in the yoga group as compared with the control group.
Conclusion:
This study highlights the usefulness of a yoga intervention for caregivers of inpatients with neurological problems. The small sample size and lack of blinding were some of the limitations of this study.
Keywords: Anxiety, caregivers, depression, neurological illness, yoga
INTRODUCTION
The prevalence of neurological disorders globally in the year 2005 was 155.36/1000 people.[1] The major burden of taking care of these patients lies with their primary caregivers. Care-giving is a difficult and physically demanding role. It disrupts familial roles as well as vocational and other activities of the caregiver. A number of studies have pointed out that the majority of these caregivers suffer from stress-related disorders such as anxiety, depression and also have poor quality-of-life.[2,3,4,5]
Yoga, which includes yogāsanas, meditation, relaxation techniques and prāṇāyāma is one of the forms of complementary and alternative medicine and is commonly used to counter the effects of stress. Yoga elevates brain neurotransmitter levels like gamma-amino butyric acid that may help treat depression and anxiety.[6] Stress has a strong association with the causation and maintenance of depression.[7] Yoga has been found to be effective in the management of stress.[8] Yoga has also been shown to be an effective treatment option for depression; it is cost-effective and is easy to implement.[9] It produces many beneficial emotional, psychological and biological effects.[10] Therefore, yoga practice may help caregivers to improve their mood as well as their ability to cope and manage stress.
Very few studies have looked at the effect of yoga in caregivers of inpatients with neurological disorders. In this context, there is a pressing need to test the efficacy of yoga for caregivers, with the objective of helping them reduce their anxiety levels as well as improving quality-of-life. This study aims at studying the efficacy of such a yoga package on the caregivers of inpatients with neurological illness using a randomized controlled design.
METHODOLOGY
The study was conducted at a tertiary research and clinical care hospital. Care-givers of inpatients with neurological disorders between the ages of 18 and 60 years, who were physically able to do yoga, were included. They were excluded if they had severe psychiatric or neurological illness, other severe medical conditions or present history of substance dependence (excluding nicotine). Each subject gave informed written consent for the study. The participants were randomized to one of two groups (yoga or control) by a computer-generated list of random numbers. The randomization was performed by an independent researcher with allocation concealment. There were 30 participants in yoga and 30 in the control arm.
A semi-structured pro forma for socio-demographic data was used to collect relevant demographic details. Patients were assessed at baseline and at the end of the study period (1 month) using the hospital anxiety and depression scale and the World Health Organization quality of life-BREF.[11,12,13]
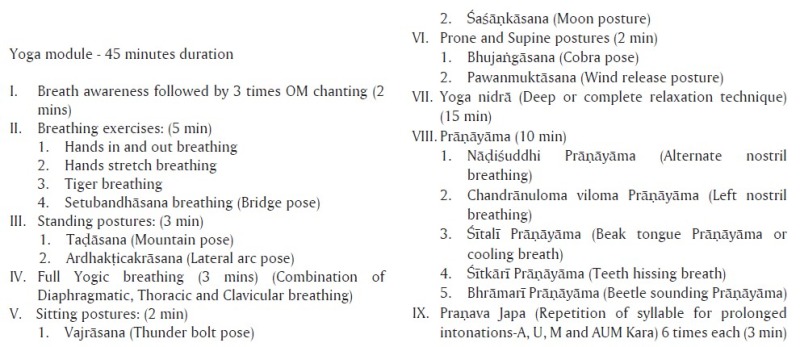
Sixty eligible and consenting caregivers were thus assessed at baseline by the researcher. The first author then taught a specific yoga module [Appendix 1] to the subjects in the yoga group for 10 days, following which they practiced yoga on their own for another 20 days. The subjects in the control group received no specific intervention, but were available for assessments. Post-test assessments were performed for both yoga and control group at the end of 1 month.
The study was approved by the interdepartmental review committee as part of the post-graduate dissertation of the principal author on 12th August 2009. Written informed consent was taken from all participants before enrolment into the study. The principal author, who has a master's degree in psychiatric nursing, also had received formal training for teaching yoga from a recognized center.
Statistical analysis
The baseline variables were compared between the yoga and control groups using independent t-test or Fisher's test. Two-way repeated measures analysis of variance was used to test the change from pre-test to post-test scores within and between groups. Analysis of covariance was performed to compare the post-test scores between the groups, adjusting for socio-demographic variables (education and length of caretaking) between the groups. Significance was defined as P<0.05.
RESULTS
Among the 60 participants (30 each in yoga and control groups), there were 17 dropouts (10 in the yoga group and 7 in the control group). The main reasons for dropout were discharge or death of the primary patient and inability of the caregiver to come for follow-up. The 17 patients who dropped out and the 43 who completed were comparable on baseline demographic measures such as age (P=0.760) and gender (P=0.364). Analysis was performed for the 43 participants who completed (controls=23 and yoga=20). The caregivers were looking after patients with vascular disorders such as stroke (35%), central nervous system infections (33%), fracture and dislocations (14%), tumors (9%), myasthenia gravis (5%), cerebral palsy (2%) and seizure (2%). The socio-demographic variables [Table 1] were comparable in both groups except the education and length of caretaking.
Table 1.
Socio-demographic data of the study subjects
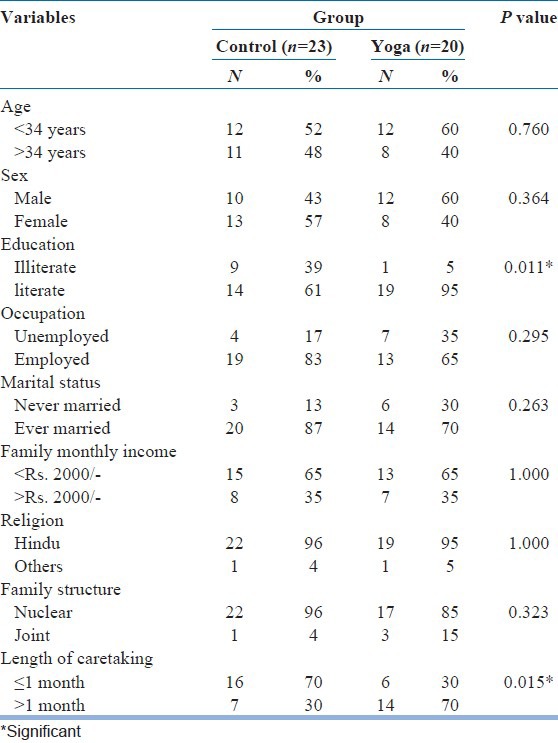
More participants in the control group were illiterate than in the yoga group (P=0.011). Caregivers in the yoga group had taken care of patients for a longer period compared with those in the control group (P=0.015).
Baseline scores of anxiety, depression and quality-of-life were comparable in the two groups [Table 2]. There was a significant association between the family type and the level of depression as well as quality-of-life. More participants from nuclear families had higher levels of depression (P=0.035) and low quality-of-life (P=0.025) as compared with participants from joint families. Gender was also significantly associated with the quality-of-life. Female caregivers had a lower quality-of-life (P=0.031).
Table 2.
Comparisons of pre- and post-test scores of anxiety, depression and quality-of-life between the yoga and control group

There was a significant (P<0.001) decrease in anxiety and depression and improved quality-of-life among the participants in the yoga group as compared with the control group following intervention [Table 2].
DISCUSSION
This study looked at the effect of yoga intervention on improving anxiety, depression and quality-of-life in caregivers of inpatients with neurological disorders. In the current study, the baseline anxiety, depression and quality of life scores did not differ significantly between the two groups, which indicate that they were comparable.
The participants had high levels of anxiety and depression, which is on par with previous studies. A previous study found that caregivers of stroke patients demonstrated higher levels of anxiety and depression, but the study was limited by non-randomization of the subjects.[14] Another study in 37 women caregivers of patients with Alzheimer's disease showed that 54, 21 and 29% of the sample had high levels of stress, anxiety and depression, respectively.[15]
The present study found that female participants had lower quality-of-life and participants from nuclear families had higher depression scores and lower quality-of-life. A previous study also found that female gender and advanced age were the main predictors of lower quality-of-life in caregivers of patients with multiple sclerosis.[16] A descriptive study on anxiety and depression among 34 female Italian caregivers of patients with Alzheimer's disease showed that the anxiety scores were positively correlated with hours of care, physical and psychological illness scores and negatively correlated with the levels of education and time for leisure activities; although, the sample size and lack of the control group was a limitation.[17] Higher demands on females in terms of homemaking duties along with care giving, as well as an underlying predisposition to depression, may explain the higher depression and lower quality-of-life. Availability of physical and emotional support from extended family may help to protect caregivers from depression and poor quality-of-life.
Pre-to post-test comparisons in our study revealed statistically significant reduction in anxiety and depression and improved quality-of-life in the yoga group as compared with the control group (P<0.001) [Table 2]. Some previous studies have found similar findings in different populations. 48 healthy volunteers who participated in the practice of yoga over a period of 4 months were assessed on subjective well-being inventory (SUBI) before and after the course, in order to evaluate the effect of practice of yoga on subjective feelings of well-being and quality-of-life. A significant improvement in 9 of the 11 factors of SUBI was observed at the end of 4 months in these participants.[18] Another study among caregivers of patients with dementia revealed statistically significant reductions in depression and anxiety and improvements in perceived self-efficacy after a six-session manualized yoga-meditation program; although, it was only a feasibility study and had no control group.[19] Overall, the literature seems to suggest that in tertiary care services “care for caregivers” should be a routine component of the treatment of these patients and their families and yoga may be useful as an intervention for the same.
One of the limitations of the study may be that the outcomes of the patients who were being cared for and any other life events during the month of the study were not assessed. It is possible that these may have had a significant impact on the caregivers’ mental state. The heterogeneous nature of neurological illness in patients, the rater not being blinded and the relatively small sample size after the dropouts may be other limitations.
Future researchers in this area may be well-advised to systematically study caregivers of patients suffering from a single neurological condition, with rater blinding and measures to control for other significant factors contributing to change in anxiety/depression scores in subjects.
This study showed that caregivers of patients with neurological disorders had high levels of stress and anxiety and that yoga therapy was effective in decreasing anxiety, depression and improving the quality-of-life in this population. This study also found that female sex and nuclear family structure were associated with higher levels of depression and lower quality-of-life. These findings have great significance in the context of the rapidly changing socio-demographic profile of developing countries, and need to be explored in greater detail in the future. In view of the small sample size and non-blinded nature of this study, the results may need confirmation by larger studies.
In the present scenario of predominantly nuclear families and rapid growth of the elderly population, caregiver stress is likely to increase despite the advances in health technology. In this context, simple but planned yoga intervention has a significant scope in reducing caregiver stress and may be a cost-effective method to handle the imminent crisis. This is an area, which needs more exploration in both research and service settings.
ACKNOWLEDGMENTS
We thank Mr. Sushrutha and Mr. Bhagath of Swami Vivekananda Yoga Anusandhana Samsthana for their help with transliteration
APPENDIX 1
Footnotes
Source of Support: The research was done under the Advanced Centre for Yoga - Mental Health and Neurosciences, a collaborative centre of NIMHANS and the Morarji Desai Institute of Yoga, New Delhi
Conflict of Interest: None declared.
REFERENCES
- 1.Gourie-Devi M. Organization of neurology services in India: Unmet needs and the way forward. Neurol India. 2008;56:4–12. doi: 10.4103/0028-3886.39304. [DOI] [PubMed] [Google Scholar]
- 2.Miyashita M, Narita Y, Sakamoto A, Kawada N, Akiyama M, Kayama M, et al. Care burden and depression in caregivers caring for patients with intractable neurological diseases at home in Japan. J Neurol Sci. 2009;276:148–52. doi: 10.1016/j.jns.2008.09.022. [DOI] [PubMed] [Google Scholar]
- 3.Ownsworth T, Hawkes A, Steginga S, Walker D, Shum D. A biopsychosocial perspective on adjustment and quality of life following brain tumor: A systematic evaluation of the literature. Disabil Rehabil. 2009;31:1038–55. doi: 10.1080/09638280802509538. [DOI] [PubMed] [Google Scholar]
- 4.Kolakowsky-Hayner SA, Miner KD, Kreutzer JS. Long-term life quality and family needs after traumatic brain injury. J Head Trauma Rehabil. 2001;16:374–85. doi: 10.1097/00001199-200108000-00007. [DOI] [PubMed] [Google Scholar]
- 5.McCullagh E, Brigstocke G, Donaldson N, Kalra L. Determinants of caregiving burden and quality of life in caregivers of stroke patients. Stroke. 2005;36:2181–6. doi: 10.1161/01.STR.0000181755.23914.53. [DOI] [PubMed] [Google Scholar]
- 6.Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression: Part I-neurophysiologic model. J Altern Complement Med. 2005;11:189–201. doi: 10.1089/acm.2005.11.189. [DOI] [PubMed] [Google Scholar]
- 7.Reiche EM, Nunes SO, Morimoto HK. Stress, depression, the immune system, and cancer. Lancet Oncol. 2004;5:617–25. doi: 10.1016/S1470-2045(04)01597-9. [DOI] [PubMed] [Google Scholar]
- 8.Parshad O. Role of yoga in stress management. West Indian Med J. 2004;53:191–4. [PubMed] [Google Scholar]
- 9.Janakiramaiah N, Gangadhar BN, Naga Venkatesha Murthy PJ, Harish MG, Subbakrishna DK, Vedamurthachar A. Antidepressant efficacy of Sudarshan Kriya Yoga (SKY) in melancholia: A randomized comparison with electroconvulsive therapy (ECT) and imipramine. J Affect Disord. 2000;57:255–9. doi: 10.1016/s0165-0327(99)00079-8. [DOI] [PubMed] [Google Scholar]
- 10.Shapiro D, Cook IA, Davydov DM, Ottaviani C, Leuchter AF, Abrams M. Yoga as a complementary treatment of depression: Effects of traits and moods on treatment outcome. Evid Based Complement Alternat Med. 2007;4:493–502. doi: 10.1093/ecam/nel114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32:50–5. doi: 10.1111/j.2044-8341.1959.tb00467.x. [DOI] [PubMed] [Google Scholar]
- 12.Skevington SM, Lotfy M, O’Connell KA WHOQOL Group. The World Health Organization's WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00. [DOI] [PubMed] [Google Scholar]
- 13.Szabo S, editor. 2nd ed. Philadelphia, New York: Lippincott-Raven Publishers; 1996. The World Health Organisation Quality of Life (WHOQOL) Assessment Instrument. [Google Scholar]
- 14.Han B, Haley WE. Family caregiving for patients with stroke. Review and analysis. Stroke. 1999;30:1478–85. doi: 10.1161/01.str.30.7.1478. [DOI] [PubMed] [Google Scholar]
- 15.Vellone E, Piras G, Sansoni J. Stress, anxiety, and depression among caregivers of patients with Alzheimer's disease. Ann Ig. 2002;14:223–32. [PubMed] [Google Scholar]
- 16.Patti F, Amato MP, Battaglia MA, Pitaro M, Russo P, Solaro C, et al. Caregiver quality of life in multiple sclerosis: A multicentre Italian study. Mult Scler. 2007;13:412–9. doi: 10.1177/1352458506070707. [DOI] [PubMed] [Google Scholar]
- 17.Sansoni J, Vellone E, Piras G. Anxiety and depression in community-dwelling, Italian Alzheimer's disease caregivers. Int J Nurs Pract. 2004;10:93–100. doi: 10.1111/j.1440-172X.2003.00461.x. [DOI] [PubMed] [Google Scholar]
- 18.Malathi A, Damodaran A, Shah N, Patil N, Maratha S. Effect of yogic practices on subjective well being. Indian J Physiol Pharmacol. 2000;44:202–6. [PubMed] [Google Scholar]
- 19.Waelde LC, Thompson L, Gallagher-Thompson D. A pilot study of a yoga and meditation intervention for dementia caregiver stress. J Clin Psychol. 2004;60:677–87. doi: 10.1002/jclp.10259. [DOI] [PubMed] [Google Scholar]