

Abstract
The latissimus dorsi is the larger, flat, dorso-lateral muscle on the trunk, posterior to the arm, and partly covered by the trapezius on its median dorsal region. Origin of the latissimus dorsi is from spinous processes of thoracic T7–T12, thoracolumbar fascia, iliac crest and inferior 3 or 4 ribs, inferior angle of scapula and insertion on floor of intertubercular groove of the humerus. We have studied 50 cadavers in the different medical colleges in which we found 2% case of anterior and posterior slip of the muscle fibers with their extension up to the pectoralis major and teres major respectively. Usually, latissimus dorsi involve in extension, adduction, transverse extension also known as horizontal abduction, flexion from an extended position, and internal rotation of the shoulder joint. It also has a synergistic role in extension and lateral flexion of the lumbar spine. The latissimus dorsi may be used for the tendon graft surgeries. Tight latissimus dorsi has been shown to be one cause of chronic shoulder pain and chronic back pain. Because the latissimus dorsi connects the spine to the humerus, tightness in this muscle can manifest as either sub-optimal glenohumeral joint function (which leads to chronic shoulder pain) or tendinitis in the tendinous fasciae connecting the latissimus dorsi to the thoracic and lumbar spine. Latissimus dorsi used for pedicle transplant rotator cuff repair reconstruction of breast, face, scalp and cranium defect. The extra slip of the latissimus dorsi may puzzle any transplant operations. We as anatomist discuss the clinical implication of the extra slip of latissimus dorsi.
Keywords: Latissimus dorsi, Slips
1. Introduction
Latissimus dorsi muscle arise as broad aponeurosis that originates from the spines of lower six thoracic vertebrae and from the posterior layer of thoracolumbar fascia attached to the spines and supraspinous ligaments of all lumbar vertebrae; sacral vertebrae and posterior crest of ilium, lower 3 or 4 ribs, and an attachment of the tip of the scapula.1 Flat tendon that twists upon itself to insert into the intertubercular groove of the humerus, just anterior to and parallel with the tendon of pectoralis major. It is supplied by the sixth, seventh, and eighth cervical nerves through the thoracodorsal (long scapular) (long subscapular) nerve. Electromyography suggests that it consists of six groups of muscle fibers that can be independently coordinated by the central nervous system.2 It extends, adducts and medially rotates the humerus at the shoulder; draws the inferior angle of the scapula inferior and medial (draws shoulder downward and backward). The synergistic muscles are rhomboids, pectoralis major, teres major. Variation in the muscle in the latissimus dorsi is not uncommon. A rare muscular anomaly of the axilla the axillary arch muscle (AAM) known as Langer's muscle, axillopectoral muscle or the “Achselbogen Muskel”. It is a thin muscular slip extending from the latissimus dorsi to the pectoralis major. Variations of this muscular anomaly have been observed commonly as adhering to the coracoid of the scapula, medial epicondyle of the humerus, teres major, long head of the triceps brachii, coracobrachialis or biceps brachii, and pectoralis minor. The most common form of this muscle extends from the latissimus dorsi to the pectoralis major, the short head of the biceps brachii or to the coracoid process.3 The neurovascular compression in the cervico-axillary region is main clinical importance. Here we are showing the anterior and the posterior slip of the latissimus dorsi muscle which can be puzzling the operation in transplantation or reconstructive surgery.
2. Material & method
We have studied 50 adult cadavers of unknown sex for 2 years of Government Medical College, Surat and in different medical colleges in Gujarat in present study. We dissect latissimus dorsi by dissection method with the reference from the Cunningham manual of anatomy.4
3. Results
We found in one case the two extra slip of the latissimus dorsi, one slip arises from the upper edge of the latissimus dorsi about the middle of the posterior fold of the axilla, and crosses the axilla in front of the axillary vessels and nerves, to join the undersurface of the tendon of the pectoralis major, the coracobrachialis and the fascia over the biceps brachii. The anterior slip is of 14 cm in length and 5 mm in breadth. One posterior slip arises from the same plane is going into the substance of the teres major muscle behind the axillary vessels and nerves (Fig. 1). The posterior slip is 12 cm in length and 4 mm in diameter (Fig. 2). Up till now the other studied shows only anterior slip but the posterior slip not has been mentioned yet in any other study.
Fig. 1.

Anterior slip.
Fig. 2.
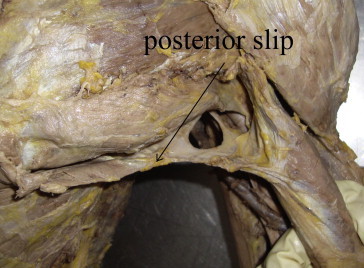
Posterior slip.
4. Discussion
The axillary arch muscle (AAM) is the most common variation of the axilla with an incidence of 7%–8%. Frequencies change from 0.25% to 37.5%, as per population and South Indian population 1.47%6 (Table 1). Variations of this muscle commonly involve a bidirectional slip with one origin and one insertion. Few cases have been described where the muscle's connections are more complex, inserting at multiple sites. We noted a case where the AMM originated from the latissimus dorsi and had two branches with insertion as follows: an anterior muscular slip, the axillary arch 14 cm in length and from 5 mm in breadth, springs from the upper edge of the latissimus dorsi about the middle of the posterior fold of the axilla and crosses the axilla in front of the axillary vessels and nerves to join the undersurface of the tendon of the pectoralis major, the coracobrachialis and the fascia over the biceps brachii.
Table 1.
Axillary arch muscles incidence study by different authors.
| Author (year) | No. of arches | No. of subjects | Percentage | Population |
|---|---|---|---|---|
| Kopsch | – | – | 7–8 | Caucasian |
| Meckel (1816) | 1 | 30 | 3.33 | Caucasian |
| Langer (1846) | 1 | 4 | 25 | Caucasian |
| Struthers (1854) | 8 | 105 | 7.62 | Caucasian |
| Wood (1868) | 6 | 102 | 5.88 | Caucasian |
| Perrin (1871) | 7 | 29 | 24.14 | Caucasian |
| MacAlister (1875) | 1 | 16 | 6.25 | Caucasian |
| Krause (1880) | 7 | 100 | 7 | Caucasian |
| Princeteau (1892) | 25 | 208 | 12.02 | Caucasian |
| Le Double (1897) | 6 | 95 | 6.3 | Caucasian |
| Pichler (1916) | – | – | 3–4 | Unknown |
| Wagenseil (1927) | 7 | 16 | 43.8 | Chinese |
| Nishi (1953) | – | – | 11.7 | Japanese |
| Kasai (1977) | 10 | 88 | 11.4 | Japanese |
| Schramm (1984) | 9 | 60 | 15 | Caucasian |
| Takafuji (1991) | 3 | 47 | 6.4 | Japanese |
| Serpell and Baum (1991) | 4 | 2000 | 0.2 | Caucasian |
| Dharap5 (1994) | 4 | 1 | – | Asian |
| Clarys (1996) | 16 | 183 | 8.7 | Caucasian |
| Kalaycioglu (1998) | 1 | 60 | 1.7 | Caucasian |
| Miguel (2001) | 3 | 50 | 6 | Caucasian |
| Merida-Velasco (2003) | 3 | 32 | 9.4 | Caucasian |
| Turgut (2005) | 1 | 26 | 3.8 | Caucasian |
| Georgiev (2006) | 2 | 56 | 3.6 | Caucasian |
| Nayak et al6 (2008) | – | – | 1.47 | South Indian |
| Lama7 (2010) | 2 | 1 | – | Indian |
| Present study | 2 | 50 | 2 | Indian |
This axillary arch crosses the axillary artery, just above the spot usually selected for the application of a ligature and may mislead a surgeon. The incidence of anterior arch is around 7% cases where as we found around 2% cases. The anterior slip may be present in some cases but the posterior slip has not been yet noted in the past.
It is also possible that a muscle connecting the latissimus dorsi to the pectoralis major covering the base of the axilla, may also serve some protective function.3 Latissimus dorsi muscle with its neurovascular pedicle transplant can performed to compensate for paralysis of triceps and posterior part of deltoid muslcle.8 Tight latissimus dorsi has been shown to be one cause of chronic shoulder pain and chronic back pain. Latissimus dorsi transfer is a useful surgical technique for treating massive irreparable postero-superior tears of the rotator cuff in young and/or active patients, providing significant pain relief and improved shoulder strength.9 Replacing the paralyzed muscle with latissimus dorsi like anterior deltoid has achieved good results in cases which have retained even weak muscle power in the rotator cuff muscles and/or the long head of the biceps.10 Latissimus dorsi transfer can be effective in restoring shoulder function after massive irreparable tears of the rotator cuff.11 Latissimus-serratus-rib osteomusculocutaneous free flaps are effective for reconstruction of composite defects of the mandible in patients in which vascularized bone containing free flaps can not be used.12 The use of latissimus dorsi myocutaneous flap with tissue expansion has proved to be an effective and esthetic method of immediate breast reconstruction after skin sparing mastectomy,13 rifle wounds to the face,14 reconstruction of scalp and cranium defect.15 Because the latissimus dorsi connects the spine to the humerus, tightness in this muscle can manifest as either sub-optimal glenohumeral joint function (which leads to chronic shoulder pain) or tendinitis in the tendinous fasciae connecting the latissimus dorsi to the thoracic and lumbar spine. Latissimus dorsi is used very frequently for the grafting as well as reconstruction flap for the extremities or for the upper limb, even for the breast surgery. The variation in the latissimus dorsi muscle should be kept in the mind for the surgeons for the operative procedures or during operation. The latissimus dorsi muscle is the largest muscle in the body, and it is useful for covering extremely large wounds. Despite its size, no practical functional motor deficit results from its transposition. Blood is supplied to the latissimus dorsi muscle via the subscapular artery, a branch of the axillary artery. The subscapular sends off a circumflex scapular branch posteriorly, then distributes a serratus branch before it enters the substance of the muscle on its undersurface as the thoracodorsal artery. A 5–10-cm pedicle can be obtained off the subscapular system. A single venae comitantes typically accompanies the artery. The pedicle can be approached directly by dissecting the latissimus dorsi from the axilla, or it can be found by following the undersurface of the muscle in a distal to proximal approach. Because the artery divides in the substance of the muscle, the muscle can be split longitudinally to form a bilobed, or two-tongued, flap. The muscle also is supplied by perforators from the thoracic intercostal and lumbar arteries that allow it to be used as a pedicled flap that can resurface posterior defects. In addition to this practical application of anatomical knowledge of anterior and posterior slip is required to operate in this region to avoid any complication. Further we need more number of cadavers to support and may get exact result. Further thorough description of muscular anomalies of the axilla will help in gaining a better understanding of the basis of associated lesions.
5. Conclusions
These anomalies of latissimus dorsi therefore clinically important because of its surgical importance and may be of particular interests to orthopedic surgeons, neurologist and cosmetic surgeons.
Conflicts of interest
All authors have none to declare.
References
- 1.Susan Standring. 39th ed. Elsevier Churchill Livingstone; Edinburgh: 2004. Gray's Anatomy. 836. [Google Scholar]
- 2.Brown J.M.M., Wickham J.B., McAndrew D.J., Huang X.F. Muscles within muscles: coordination of 19 muscle segments within three shoulder muscles during isometric motor tasks. J Electromyogr Kinesiol. 2007;17:57–73. doi: 10.1016/j.jelekin.2005.10.007. [DOI] [PubMed] [Google Scholar]
- 3.Loukas M., Noordeh N., Tubbs R.S., Jordan R. Variation of the axillary arch muscle with multiple insertions. Singapore Med J. 2009;50(2):e88–e90. [PubMed] [Google Scholar]
- 4.Romanes G.J. 50th ed. vol. 1. Oxford Medical Publications; 2008. Cunningham's Manual of Practical Anatomy. (Upper and Lower Limbs). 37. [Google Scholar]
- 5.Dharap A. An unusually medial axillary arch muscle. J Anat. 1994;184:639–641. [PMC free article] [PubMed] [Google Scholar]
- 6.Nayak S.R., Krishnamurthy A., Ramanathan L.A. Multiple muscular anomalies of upper extremity: a cadaveric study. Rom J Morphol Embryol. 2008;49(3):411–415. [PubMed] [Google Scholar]
- 7.Lama Polly, Potu B.K., Bhat K.M.R. Chondrohumeralis and axillary arch of Langer: a rare combination of variant muscles with unique insertion. Rom J Morphol Embryol. 2010;51(2):395–397. [PubMed] [Google Scholar]
- 8.Du Toit G.T., Pretoria Levy S.L. Transposition of latissimus dorsi for paralysis of triceps brachii. J Bone Joint Surg. February 1967;49B(1):135–137. [PubMed] [Google Scholar]
- 9.Zafra Manuel, Carpintero Pedro, Carrasco Carmen. Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff. Intern Orthop (SICOT) 2009;33:457–462. doi: 10.1007/s00264-008-0536-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Itoh Y., Sasaki T., Ishiguro Uchinishi K., Yabe Y., Fukuda H. Transfer of latissimus dorsi to replace a paralysed anterior deltoid. J Bone Joint Surg. August 1987;69-B(4):647–651. doi: 10.1302/0301-620X.69B4.3611175. [DOI] [PubMed] [Google Scholar]
- 11.Aoki M., Okamura K., Fukushima S., Takahashi T., Ogino T. Transfer of latissimus dorsi for irreparable rotator-cuff tears. J Bone Joint Surg Br. 1996;78-B:761–766. [PubMed] [Google Scholar]
- 12.Kim Paul D., Blackwell Keith E. Latissimus-serratus-rib free flap for oromandibular and maxillary reconstruction. Arch Otolaryngol Head Neck Surg. Aug 2007;133(8):791–795. doi: 10.1001/archotol.133.8.791. [DOI] [PubMed] [Google Scholar]
- 13.Abdalla Hassan M., Shalaan Mohamed A., Fouad Fouad A., Elsayed Ahmed A. Immediate breast reconstruction with expander assisted latissimus dorsi flap after skin sparing mastectomy. J Egyptian Nat Cancer Inst. June 2006;18(2):134–140. [PubMed] [Google Scholar]
- 14.Danino A.M., Hariss P.G., Servant M. Early management, with a minimal initial hospitalization length, of major self-inflicted rifle wounds to the face by a single latissimus dorsi free musculocutaneous flap: a 10-year experience. J Plastic Surg. 9 June 2009;9:e23. Open Access. [PMC free article] [PubMed] [Google Scholar]
- 15.Arai Hajime, Yanai Akira, Nishida Masanobu, Yoshikata Rie, Nakanishi Hajime, Sato Kiyoshi. Reconstruction of scalp and cranium defect utilizing latissimus dorsi musculocutaneous and serratus anterior muscle free flaps with interpositional anastomosis of T-shaped flap artery. Skull Base Surg. April 1995;5(2):117–121. doi: 10.1055/s-2008-1058942. [DOI] [PMC free article] [PubMed] [Google Scholar]