

Abstract
Conflict of interest: none declared.
Introduction
Anemia is a blood disorder characterized by abnormally low levels of healthy red blood cells or reduced hemoglobin, the iron-bearing protein in red blood cells that delivers oxygen to tissues throughout the body. The most common symptoms of this disorder are fatigue, weakness and, in extreme cases, shortness of breath or palpitations, or you may have no symptoms at all. Sports anemia is a term loosely applied to a least three different conditions: hemodilution, iron deficiency anemia and foot-strike anemia. Not exclusive to athletes, iron deficiency anemia occurs most often among women who may lose more iron each month when they menstruate than they take in.
Material and Methods
Therefore, we examined its effect on the physical condition of female athletes. Several years (since 2010th until 2012th), we studied how anemia among girls (pioneers, juniors and seniors categories) that are involved in sports (women’s soccer, volleyball and handball) in Rasina’s district (Serbia), affecting their physical fitness. When their trainers approach to us, complaining that they have players who are great, so extraordinary talents, but by no means able to withstand more than twenty minutes in the game, we suggest them to perform laboratory tests. It was tested 134th female athletes.
Results and Discussion
Anemia was observed in 43. (9. pioneers, 19. juniors and 15. seniors). So, laboratory results showed that in these girls anemia causes poor sport condition. After that, the girls enhanced nutrition. Their diet consisted of iron supplements and vitamins. Altitude training was organized for them, also. After all these treatments, condition significantly improved. It was first time that trainers in Rasina’s district realizing significance of laboratory tests.
Key words: anemia, RBC, iron, haemoglobin, sport environment, monitoring, prevention, altitude training
1. INTRODUCTION
Anemia is a condition in which blood does not have enough red blood cells (1-7). Erythrocytes are produced in the bone marrow. For the proper synthesis of red blood cells is important in the organism to enter enough: iron, protein, minerals, vitamins, but it’s also very important normal function of liver and kidney. Red blood cells contain hemoglobin, a protein that is rich in iron. Hemoglobin binds oxygen and transmits it from the lungs to vital organs: brain, kidneys, heart, muscles and other tissues. The body can not function without oxygen: oxygen-rich blood, providing a healthy work of all organs.
Anemia is typically diagnosed on a complete blood count (2). Apart from reporting the number of red blood cells, the hemoglobin level and concentration of iron, the automatic counters also measure the size of the red blood cells by flow cytometry, which is an important tool in distinguishing between the causes of anemia. Examination of a stained blood smear using a microscope can also be helpful, and it is sometimes a necessity in regions of the world where automated analysis is less accessible.
In modern counters, four parameters (RBC count, hemoglobin concentration, MCV and RDW) are measured, allowing others (hematocrit, MCH and MCHC) to be calculated, and compared to values adjusted for age and sex. The treatment of the anemia is achieved by treating the underlying disease (3). Blood transfusions are reserved for acute blood loss when symptoms of hypovolemia and shock are present, or in chronic anemia if there are signs of inadequate cardiovascular or pulmonary compensation and an underlying cause cannot be found or treated.
Sport represents a significant part of our different lifestyles. Many sports associations have built up professional and voluntary structures and include environmental issues in their public relations. If environmental aspects are to be considered regularly and not just sporadically, operators of sports facilities need systematic environmental management. Each athlete must undergo the proper training in order to acquire the physical skills required to participate in each sport.
Improving energy efficiency in spoprtista is an important prerequisite for achieving results and preservation of health. In fact, proper nutrition and quality living environment play an important role.Adequate food and fluid should be consumed before, during, and after exercise to help maintain blood glucose concentration during exercise, maximize exercise performance, and improve recovery time. Athletes should be well hydrated before exercise and drink enough fluid during and after exercise to balance fluid losses.
1.1. Types and symptoms of anemia
There are several kinds of anemia: it can be mild or severe, acute or chronic (4).
It is important to emphasize that anemia is, (similar temperature) SYMPTOM and not the diagnosis itself. About 10% of the population has a general exclusion anemia, and in some countries this figure is even higher, more frequent in women (menstruation), vegetarians (vitamin and iron), infants.
There are three basic principles of occurrence of anemia:
Lack of synthesis of hemoglobin / RBC, Loss of hemoglobin / red blood cells (blood), Destruction / hemolysis / red blood cells faster than the reconstruction.
By the size of blood cells anemia is classified in three basic types:
Normocyte’s: if the red blood cells of normal size (for the Laboratory abbreviated MCV: mean corpuscular volume), microcyte’s: red blood cells small volume (MCV decreased), macrocyte’s: red blood cells increased volume (MCV increased),
The most common causes of anemia are (5):
Acute or chronic bleeding / blood loss, Iron deficiency or anemia sideropenic: affecting approximately 1-2% of the population, more women because of menstrual bleeding, Lack of vitamin B12 and folic acid causes pernicious anemia, Anemia of chronic disease: cancer, rheumatic, immunological diseases, HIV / AIDS, kidney or liver disease can cause anemia, aplastic anemia: a serious, life-threatening anemia in which bone marrow does not produce enough red blood cells, Anemia caused by a disorder of bone marrow, Hemolytic anemia: red blood cells are destroyed at the periphery so that the bone marrow does not have time to create a sufficient number of red blood cells.This anemia is present in some autoimmune diseases. genetic variants of anemia.
The symptoms of anemia vary according to the type of anemia, the underlying cause, and any underlying health problems, such as hemorrhage, ulcers, menstrual problems, or cancer (6). Specific symptoms of those problems may be noticed first. The body also has a remarkable ability to compensate for early anemia. If your anemia is mild or has developed over a long period of time, you may not notice any symptoms (1, 5).
Symptoms of anemia are: fatigue, exhaustion, pallor of skin and mucous membranes, rapid heart beat, tachycardia, difficulty breathing, stenocardia, fainting, headaches, cold hands / feet (7).
2. THE AIM AND METHODS OF STUDY
a) The aim of study: The aim of this study was to determine whether anemia cause poor sport condition in female athletes. During the three years, we monitored the impact of environmental and dietary preparations to improve health and physical fitness of female athletes. b) Research methods: Laboratory tests we performed on the automated blood counter elements “Celly” (RBC, hemoglobin) and biochemical automatic analyzer “Selectra” (iron). c) Subjects: Laboratory tests was included in 134 football, handball and volleyball players, all categories, from pioneers to the seniors (41 pioneers aged 10 ± 3.2 years, 42 juniors aged 15 ± 2.1 years and 51 seniors age 23 ± 5, 7 years old).
3. RESULTS OF STUDY
In this paper we present the results of our study in anemic female athletes. (Table 1, Figure 3, 4 and 5). It is the position of the Academy of Nutrition and Dietetics that the total diet or overall pattern of food eaten is the most important focus of healthy eating. All foods can fit within this pattern if consumed in moderation with appropriate portion size and combined with physical activity. The authors are trying to communicate with sportist’s, to be used by healthy food and living environment, in order to reduce the conditions for the occurrence of anemia and improve performance on the sports field.
Table 1.
Results of testing 43 players with established anemia
| Year | Players | RBC (T/L) | Haemoglobin (g/L) | Iron (mmol/L) |
|---|---|---|---|---|
| 2010. | pioneers | 3,2 ± 0,6 | 96,5 ±19,2 | 7,0 ± 2,5 |
| 2010. | juniors | 2.9 ± 0,7 | 91,4 ± 21, 5 | 6,4 ± 3,5 |
| 2010. | seniors | 2,8 ± 0,8 | 89,8 ±23,5 | 5,7 ±4,8 |
| 2011. | pioneers | 3,4 ± 0,5 | 101,3 ± 21,2 | 8,7 ±2,1 |
| 2011. | juniors | 3,07 ±0,7 | 95,0 ±31,7 | 7,9 ±4,9 |
| 2011. | seniors | 3,01 ±0,7 | 92,8 ±21,3 | 7,1 ±1,7 |
| 2012. | pioneers | 3,9 ± 0,4 | 118 ±23,0 | 9,9 ± 2,4 |
| 2012. | juniors | 3,6 ± 0,7 | 112 ± 19,5 | 9,5 ± 2,0 |
| 2012. | seniors | 3,5 ± 1,2 | 110 ± 18,5 | 9,4 ± 1,9 |
| By histogram: | ||||
| X – ordinates: examine years (pioneers, juniors, seniors) | ||||
| Y–Ordinates: | ||||
| Diagram RBC | ||||
| Diagram Haemoglobin | ||||
| Diagram Iron | ||||
Figure 3.
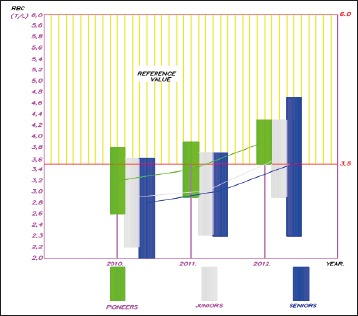
Number of RBC included in our research
Figure 4.

Concentration of Haemoglobin in our sample
Figure 5.
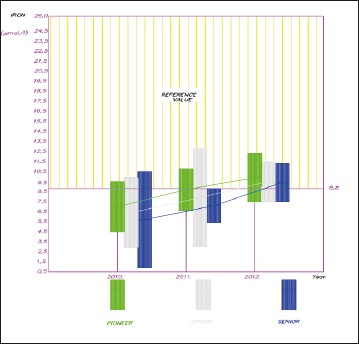
Concentration of Iron in our sample
4. DISCUSSION
Anemia is a condition in which you have a reduced amount of hemoglobin or a low number of red blood cells (8, 9, 10, 11, 12). Another condition known as sports anemia is iron deficiency anemia (13). Not exclusive to athletes, it occurs most often among women who may lose more iron each month when they menstruate than they take in. Not all women athletes are equally at risk for anemia. Risk factors include: recent childbirth, excessive menstrual flow, disadvantaged socioeconomic background, dietary restrictions such as vegetarian diet, weightloss diets, or fad diets, intense or prolonged endurance training, personal or family history of anemia, chronic disease, or bleeding disorders, use of anti-inflammatory medications, and recent blood donation.
Iron plays a critical role in aerobic capacity and performance because of its role as an oxygen transporter to working muscles (14). Less than adequate iron results in less oxygen delivered to muscles, resulting in maximal oxygen consumption deterioration and less that optimal performance. Athletes have a higher rate of iron deficiency than non-athletes because of iron loss through sweat, urine, and in the gastrointestinal tract, and female athletes are particularly at risk for deficiency due to menstruation. Depleted iron stores result in iron deficiency which develops and progresses through stages: depleted iron stores (functional iron remains normal); early functional iron deficiency without anemia; and iron-deficiency anemia.
Iron deficiency is a common problem for women athletes (8). Studies have routinely found that athletes, especially female athletes, are often iron-deficient or anemic (9). Iron is essential for athletic performance (10). One of its major functions is to carry oxygen to and carbon dioxide away from all the cells in your body. The brain also relies on oxygen transport and without enough iron you will find it hard to concentrate and feel tired and irritable. Iron is also needed to maintain a healthy immune system. If you don’t have enough iron you may be prone to more frequent infections.
Because women experience menstruation once a month, an increase in iron is necessary due to blood loss.
Oral iron supplements are the best way to restore iron levels in blood (11). There are two forms of supplemental iron: ferrous and ferric. Ferrous iron is better absorbed and is the preferred form of iron tablets. Ferrous iron is available in three forms: ferrous fumarate, ferrous sulfate, and ferrous gluconate.
Iron absorption from any foods, whether plant or animal, is decreased if they are accompanied at meals by caffeine. Calcium and zinc also reduce the ability of the body to absorb iron. However adding fruit (citrus fruit in particular), to meals enhances iron absorption. The best sources of iron in the diet include: Lean red meat, iron-fortified breakfast cereal, nuts and legumes, (combined these with foods high in vitamin C).
Iron replacement therapy can cause gastrointestinal problems, sometimes severe ones. Excess iron may also contribute to heart disease, diabetes, and certain cancers. Doctors generally advise against iron supplements in anyone with a healthy diet and no indications of iron deficiency anemia (12).
With that knowledge, some trainers of female athletes in Rasina’s district had came in Health Center Krusevac, complaining that they have players who are great, so extraordinary talents, but by no means able to withstand more than twenty minutes in the game. Doctors suggest them to perform laboratory tests.
It was tested 134th female athletes. Anemia was observed in 43. (9. pioneers, 19. juniors and 15. seniors). Anemia was defined using the following parameters: a diminished number of red blood cells, decreased values of hemoglobin concentration and decreased values of serum iron concentration (16).
The testing results are presented in Table 1. and Figures 3, 4 and 5. It is evident that the lowest values of all parameters in all groups of respondents were in 2010th year. The number of erythrocytes in the pioneers was 3.2 ± 0.6, T/L which was significantly lower than the reference value (4.75 ± 1.25 T/L). In the juniors, number of red blood cells in 2010th year amounted to 2.9 ± 0.7 T/L, which is also significantly different from the reference value. In the seniors, the number of red blood cells in 2010th year was 2.8 ± 0.8 T/L, which was significantly different from the reference value. Hemoglobin in the pioneers was 96.5 ± 19.2 g/L, in 2010th year, which was significantly different compared to the reference value (142 ± 32.5 g /L). In the juniors, concentration of hemoglobin was 91.4 ± 21, 5 g / L, (In 2010th year) which is also significantly different from the reference value. Hemoglobin of the seniors (in 2010th year) was 89.8 ± 23.5 g/L, which was significantly different from the reference value.
In 2010th year, the concentration of iron in serum was also significantly lower than the reference value (17.4 ± 8.6 mmol/L) in all investigated groups. In the pioneers it was 7.0 ± 2.5 mmol/L, the junior 6.4 ± 3.5 mmol/L, and the senior 5.7 ± 4.8 mmol/L. The following year, the results in all groups were better, because the athletes, received therapy that abutment preparations of iron and vitamins But, the results were not quite satisfactory. Most female athletes told us that they willingly ended therapy because they felt much stronger than they were.
In 2011th year the number of red blood cells was: in the pioneers 3.4 ± 0.5 T/L, in the juniors 3.07 ± 0.7 T and in the seniors 3, o1 ± 0.7 T/L. That was still significantly different from the reference value. Values of hemoglobin in all groups in 2011th year were significantly different from reference values: the pioneer value of hemoglobin was 101.3 ± 21.2 g /L, the junior 95.0 ± 31.7 g/L and the seniors 92.8 ± 21.3 g /L. The concentration of iron in serum from all groups in 2011th year was also significantly lower than the reference values: the pioneers 8.7 ± 2.1 mmol/L, the juniors 7.9 ± 4.9 mmol/L and the seniors 7.1 ± 1.7 mmol/L.
In 2012 th year results was improved and in all athletes were within normal ranges. The number of red blood cells was: in the pioneers 3.9 ± 0.4 T/L, in the juniors 3.6 ± 0.7 T/L, and in the seniors 3.5 ± 1.2 T/L. Hemoglobin was: in the pioneers 118 ± 23.0 g/L, in the juniors 112 ± 19.5 g/L and in the seniors 110 ± 18.5 g /L. Hemoglobin concentration was also within normal values, although close to the lower limit. It was: in the pioneers 9.9 ± 2.4 mmol/L, in the juniors 9.5 ± 2.0 mmol/L and in the seniors 9.4 ± 1.9 mmol/L. It were pretty surprised that the results in 2012th year were within the reference values. In that year, the tested athletes were taking part at sports camp on Jastrebac mouth (three weeks), and five days after that, at biweekly high altitude training on Kopaonik mount. In both case, they were prepared at an altitude of 800 meters (an altitude titled as –“factory of red blood cells”).
5. CONCLUSION
Our research has shown that anemia was observed in 32,8% female athletes. Therefore, it is proposed to increase their intake of iron nutrition and vitamins. It also was suggested that they go to altitude training. These measures have improved the condition of the athletes. The concentration of hemoglobin and iron in their blood, as well as the number of red blood cells, after the measures taken were within the reference value. So, It was first time that old-fashioned trainers in Rasina’s district was realizing significance of laboratory tests. Moreover they have accepted the necessity of constant monitoring and control of hematological and biochemical parameters. In the framework of prevention, they also agreed that it is necessary to take into account the quality of the food in the “fight” against anemia and basic preparations carried out under optimal conditions.
Figure 1.

Classification against Red blood cell size
Figure 2.

Laboratory testing in anemic female athletes
REFERENCES
- 1.http//www.MedicineNet.com Definition of Anemia. Last Editorial Review: accessed September 2012 [Google Scholar]
- 2.Maksimovic R.Kliničko-laboratorijska dijagnostika, APEIRON, Banja Luka, 2010 [Google Scholar]
- 3.World Health Organization Worldwide prevalence of anaemia 1993–2005. Geneva: World Health Organization; ISBN 978-92-4-159665-7. Archived from the original on 12 March 2009. Retrieved 2009-03-25 [Google Scholar]
- 4.http//www.eMedicineHealth Anemia by Saimak T. Nabili, MD, MPH Editor: Melissa Conrad Stöppler MD. Last Editorial Review: 12/9/2008. Retrieved on 4 April 2009. [Google Scholar]
- 5.http//www.merriam-webster dictionary Anemia. Retrieved on May 25, 2009 [Google Scholar]
- 6.http//www.NationalHeart Lung and Blood Institute. What Causes Anemia? Retrieved on June 9, 2010 [Google Scholar]
- 7.http// www.Undersea and Hyperbaric Medical Society “Exceptional Blood Loss - Anemia”. Retrieved 2008-05-19. [Google Scholar]
- 8.Halterman JS, Kaczorowski JM, Aligne CA, Auinger P, Szilagyi PG.Iron Deficiency and Cognitive Achievement Among School-Aged Children and Adolescents in the United States. Pediatrics. 2001; 107(6): 1381-1386. 10.1542/peds.107.6.1381.PMID 11389261. [DOI] [PubMed] [Google Scholar]
- 9.Chatard JC.et al. Anemia and iron deficiency in athletes. Sports Medicine. 1999; 27(4): 229-240 [DOI] [PubMed] [Google Scholar]
- 10.http//www.”Iron Deficiency - United States, 1999-2000” MMWR 51 (40): 897–899 October 11, 2002. Retrieved 21 April 2012 [PubMed] [Google Scholar]
- 11.Alleyne M, Horne MK, Miller JL.Individualized treatment for iron-deficiency anemia in adults. Am J Med. 2008. Nov; 121(11): 943-948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.American Dietetic Association (ADA) Nutrition and athletic performance–Position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine. Journal of the American Dietetic Association. 2000; 100: 1543-1556 [DOI] [PubMed] [Google Scholar]
- 13.Grantham-McGregor S, Ani C.“Iron-Deficiency Anemia: Reexamining the Nature and Magnitude of the Public Health Problem”. J Nutr. 2001; 131(2): 649S-668SPMID 11160596 [DOI] [PubMed] [Google Scholar]
- 14.Rockwell M, Hinton P.Understanding iron. Training & Conditioning. 2005; 15(8): 19-25 [Google Scholar]
- 15.Biočanin R, Danelišen D, Amidžić B.Morbiditet stanovništva kao uzrok i posledica devastacije radne i životne sredine, II Kongres »Ekologija, zdravlje, rad i sport«, Banja Luka, 09-8-10. 09. 2011 [Google Scholar]
- 16.Kozomara R, Maksimović R, Biočanin R.Uticaj stresa na pojavu dijabetičke hipertenzije kod raseljenih lica, III Kongres „Zdravlje, ekologija, rad i sport“, Banja Luka, 11-13 09. 2011 [Google Scholar]