

Abstract
Intestinal current measurements (ICM) from rectal biopsies are a sensitive means to detect cystic fibrosis transmembrane conductance regulator (CFTR) function, but have not been optimized for multicenter use. We piloted multicenter standard operating procedures (SOPs) to detect CFTR activity by ICM and examined key questions for use in clinical trials. SOPs for ICM using human rectal biopsies were developed across three centers and used to characterize ion transport from non-CF and CF subjects (two severe CFTR mutations). All data were centrally evaluated by a blinded interpreter. SOPs were then used across four centers to examine the effect of cold storage on CFTR currents and compare CFTR currents in biopsies from one subject studied simultaneously either at two sites (24 hours post-biopsy) or when biopsies were obtained by either forceps or suction. Rectal biopsies from 44 non-CF and 17 CF subjects were analyzed. Mean differences (µA/cm2; 95% confidence intervals) between CF and non-CF were forskolin/IBMX=102.6(128.0 to 81.1), carbachol=96.3(118.7 to 73.9), forskolin/IBMX+carbachol=200.9(243.1 to 158.6), and bumetanide=-44.6 (-33.7 to -55.6) (P<0.005, CF vs non-CF for all parameters). Receiver Operating Characteristic curves indicated that each parameter discriminated CF from non-CF subjects (area under the curve of 0.94-0.98). CFTR dependent currents following 18-24 hours of cold storage for forskolin/IBMX, carbachol, and forskolin/IBMX+carbachol stimulation (n=17 non-CF subjects) were 44%, 47.5%, and 47.3%, respectively of those in fresh biopsies. CFTR-dependent currents from biopsies studied after cold storage at two sites simultaneously demonstrated moderate correlation (n=14 non-CF subjects, Pearson correlation coefficients 0.389, 0.484, and 0.533). Similar CFTR dependent currents were detected from fresh biopsies obtained by either forceps or suction (within-subject comparisons, n=22 biopsies from three non-CF subjects). Multicenter ICM is a feasible CFTR outcome measure that discriminates CF from non-CF ion transport, offers unique advantages over other CFTR bioassays, and warrants further development as a potential CFTR biomarker.
Introduction
Cystic fibrosis (CF) is the most common lethal genetic disease in the Caucasian population, with autosomal recessive inheritance and an incidence of 1:3000 US births [1]. Cystic fibrosis is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene, which encodes the CFTR ATP-binding cassette protein. CFTR is a chloride and bicarbonate anion channel and regulates the transport of salt and water across several epithelia [2–7]. The CFTR gene has >1800 disease-causing mutations, with deletion of phenylalanine at position 508 found in >85% of CF patients. F508del-CFTR is rapidly degraded in the 26S proteosome, with little if any mature protein reaching the plasma membrane [8–11]. The F508del-CFTR mutation is an appropriate target for drug development as recent results indicate that small molecules that modulate F508del-CFTR maturation (‘correctors’) demonstrate modest bioactivity in Phase II clinical trials [12].
There are two biomarkers of CFTR function that have been commonly used to detect the activity of CFTR modulators: sweat chloride (Cl-) and nasal potential difference (NPD) [13] [12,14–20]. These bioassays have demonstrated variable sensitivity to detect CFTR modulator bioactivity, and both biomarkers have advantages and shortcomings. For example, while sweat Cl- is feasibly performed in subjects from infancy through adulthood, it is an indirect measure of CFTR function that is inextricably linked to sodium absorption through the epithelial sodium channel (ENaC) [13]. Sweat Cl- values can be influenced by a number of external factors such as age, salt intake, aldosterone and other hormone levels, skin integrity, and additional medical conditions (e.g., ectodermal dysplasia, thyroid function) that are independent of CFTR activity. NPD is the only CFTR biomarker commonly used in clinical trials that fully isolates CFTR activity, thereby providing a high degree of specificity for functional CFTR at the plasma membrane [20–22]. However, the test is technically difficult to perform, may be insensitive to small changes in CFTR function, and is less feasible in children who cannot cooperate with the test. Thus, additional CFTR biomarkers that are sensitive and isolate CFTR activity, are highly discriminatory between CF and non-CF individuals, can be easily performed in young CF patients, and monitor CFTR in a target organ with disease manifestations are needed.
One assay that may address many of these limitations is Intestinal Current Measurements (ICM) from rectal biopsy samples [23–30]. This method is attractive since similar measures of ion transport (e.g., short-circuit current, Isc) with commercially available equipment are commonly used to quantify CFTR activity in preclinical model systems (e.g., CF and non-CF mice and pigs) [31–36]. Furthermore, ex vivo ICM is a direct assay to isolate and quantify CFTR dependent currents compared with in vivo measures of nasal potential difference or Na+ and Cl- ion concentrations (that are the product of CFTR activity). CFTR is expressed at high levels in the rectum, the tissue is a target organ of disease that is not altered by CF manifestations or progression, and the biopsies are studied ex vivo, all of which provide flexibility in the reagents that can be used to detect and quantify CFTR activity.
ICM studies of human rectal tissue have been examined for nearly two decades, predominately in European and more recently South American CF care and research sites [27,29,37] [38]. This experience indicates that the assay is safe and well tolerated, that ICM is sensitive and specific for CFTR function, and it is highly discriminatory between severe CF (with no detectable CFTR activity), mild CF (with residual CFTR activity), and non-CF (normal CFTR function) [25,30] [23,38]. Rectal biopsies can be performed safely in infants and are routinely used to diagnose conditions in the neonatal period such as Hirschsprung’s disease. Together, these data provide strong rationale to examine the feasibility of this assay in a multicenter format prior to clinical studies of CFTR modulators.
To date there have been no studies of ICM that have used common SOPs across study centers. This lack of standardized practices could impede its use as a biomarker in future clinical trials, where standardized CFTR biomarker procedures (sweat Cl-, NPD) are important contributors to the successful study of CFTR modulators [18,20]. It is also unknown whether the electrophysiologic aspects of the assay (which require specialized equipment and training) can be centralized (i.e., can biopsies performed at a one site be studied by ICM at a second site) and whether different biopsy methods (e.g., use of suction or forceps) produce similar ICM data. In the current study, common SOPs for ICM performance were used across three CF research sites to generate data regarding ICM performance in CF patients with severe mutations compared with non-CF controls. The SOPs were then used to examine questions relevant to next steps in biomarker development, including the effects of cold storage on ICM results, the feasibility of performing ICM on biopsied tissue at a second site (relative to the site of origin), and ICM characteristics of rectal biopsies obtained by suction and forceps techniques.
Methods
Ethics statement
This study was approved by the local institutional review board at each study site, and all clinical investigation was conducted according to the principles expressed in the Declaration of Helsinki. All study subjects signed informed consents for study participation.
Study subjects
Initial studies were completed in non-CF subjects to demonstrate assay proficiency (five sequential subjects) using a central data interpreter. Subsequently, CF and non-CF subjects were enrolled prospectively using the common SOPs developed by the study team. Non-CF subjects undergoing scheduled lower endoscopy for clinical purposes (e.g., cancer screening) were targeted for enrollment, and bowel preparation was per the practices of the treating gastroenterologist. All CF patients underwent the biopsy for research purposes, and performed a self-administered enema (in each 118 mL delivered dose, monobasic sodium phosphate monohydrate = 19 gm, and dibasic sodium phosphate heptahydrate = 7 gm) prior to the procedure. CF patients were offered sedation, and a simple questionnaire assessing their tolerance of the procedure was administered following completion.
SOP development
Common equipment, biopsy methods, tissue dissection, voltage clamp, and reagents were defined based on review of prior publications, discussions with personnel experienced in ICM performance, and testing of conditions [23,25,27,29,30]. Personnel from each of the study sites underwent common onsite training in tissue dissection, mounting, and Ussing chamber assessment.
Biopsy
Forceps biopsies were performed using the Olympus endojaw pinless beveled biopsy forceps (FB-230U, Olympus medical systems, Japan) under direct visualization by a trained gastroenterologist. Suction biopsies were performed using the C-Rbi2 rectal biopsy system (Aus systems Pty Ltd, South Australia, Australia). Biopsies were placed in iced RPMI 1640 buffer, and transported directly to the ICM technician for dissection and mounting. The time between biopsy and mounting was typically less than one hour.
Equipment and reagents
Identical voltage clamps and tissue mounts were used at all study sites (Physiologic Instruments, San Diego, CA), including VCC MC8 clamps and chambers. Tissues were warmed to 37°C by a circulating pump and continuously gassed with 95% O2: 5% CO2 in RPMI 1640 media + 25 mM HCO3 unless indicated otherwise, when Ringers buffer (NaCl 120 mM, NaHCO3 25 mM, KH2PO4 3.33 mM, K2HPO4 0.83 mM, CaCl2.2H2O 1.2 mM, MgCl2.6H2O 1.2 mM, and gluconic acid 10 mM) replaced RPMI media. Tissue was dissected under a dissection microscope, removing the muscularis mucosa followed by mounting in P2302T, 0.33cm2 sliders. The tissue was then placed in the Ussing chambers, and voltage clamped to monitor Isc as previously described [27]. Tissue was treated with 10 µM indomethacin (mucosal and serosal compartments) to reduce CFTR dependent Cl- secretion to baseline. Following stabilization of currents (~30 min) the tissue was treated with amiloride (100 µM, mucosal compartment) to block Na+ absorption for 15 min. Tissues were then stimulated with 10 µM forskolin + 100 µM IBMX (mucosal and serosal compartments) to raise intracellular cAMP and monitored for 20 min. Tissues were then stimulated with carbachol (100 µM, serosal) to activate basolateral K+ channels and augment CFTR-dependent currents. These maneuvers have been shown to isolate CFTR activity, producing a large CFTR-dependent Cl- secretory current (serosal to mucosal direction) that is evident in the presence of functional CFTR at the mucosal plasma membrane [23,25,27]. In the absence of CFTR, these maneuvers can produce a small secretory K+ current with a downward deflection in the Isc. Following current stabilization (15-20 min), bumetanide (100 µM) was added to the serosal compartment to block the Na+/K+/2Cl- co-transporter. This inhibited CFTR-dependent Cl- transport in the presence of CFTR (downward deflection in Isc), or produced an upward deflection in the absence of CFTR (inhibition of K+ secretion). Examples of tracings from non-CF and CF subjects are included in Figure S1 in File S1. The CFTR blockers CFTRinh-172 (10-50 µM) and GLYH101 (50-100 µM) failed to predictably inhibit CFTR currents in human rectal biopsy tissue (Figure S2 in File S1), and thus were not routinely used in our studies.
Forskolin, 3-isobutyl-1-methylxanthine (IBMX, a nonspecific phosphodiesterase inhibitor), carbachol, and bumetanide were obtained from Sigma-Aldrich, St. Louis, MO, aliquoted into single use tubes, and stored frozen until the biopsies were studied. RPMI 1640 media was obtained from Invitrogen, Carlsbad, CA. CFTRinh172 and GLYH101 were purchased through the CFFT Compound Distribution Program.
Data collection
Prior to analyses, all data were interpreted by a blinded reader (site and diagnosis). Each biopsy sample had up to five Isc parameters calculated, including the change in Isc following amiloride, forskolin/IBMX, carbachol, forskolin/IBMX + carbachol, and bumetanide additions. Mean values were calculated in subjects with multiple biopsies obtained at the same study site or on the same day.
Statistical analysis
A descriptive analysis was performed with calculation of means, medians, and standard deviations for continuous data and percentages for categorical data. Analyses of SOP effectiveness, including the impact of storage conditions, study site agreement and extraction method agreement, were conducted using Isc parameters from biopsies of only non-CF subjects. The impact of storage condition (cold versus fresh tissue) on each Isc parameter was examined using the paired t-test and intraclass correlation coefficient (ICC) analysis [39], where fresh tissue was considered to be the gold standard. In addition to the paired t-test and ICC, measurement agreement between sites with respect to each Isc parameter was assessed using Bland-Altman analysis [40]; the site of biopsy origin was treated as the gold standard. Due to the limited number of subjects providing forceps and suction biopsies, descriptive statistics for the two methods are shown. For comparisons of tissue resistance in forceps vs suction biopsies, paired t-tests were used. Data transformations were used for Isc parameters to achieve normality assumptions for inferential analyses.
Differences between CF and non-CF subjects with respect to continuous measures were assessed using the Wilcoxon Mann-Whitney test. The diagnostic performance of each Isc parameter at distinguishing CF and non-CF tissues was examined using Receiver Operator Characteristic (ROC) curves; results are reported as Area Under the Curve (AUC). Power analyses were used to determine the capability of ICM and NPD parameters to detect statistically significant differences in increasing levels of CFTR function. The approach was based on a one-sided paired t-test for mean differences observed pre- and post-observation with alpha = 0.05, assuming intrasubject correlation of 0.50 between observation periods. The intersubject SD observed from the study data was used as the upper bound on calculations.
To assess variance in CFTR responses (intra-site and inter-site), Analysis of variance (ANOVA) was performed. This produced the model sum-of-squares (inter-site variation) and error sum-of-squares (intra-site variation), along with the total sum-of-squares. This information was then converted to variances (SD2 / [n -1]).
Agreement analyses for Isc parameters have been back-transformed to original scale. Model adequacy was verified with each agreement assessment using residual diagnostics. All results are reported as mean (95% CI) for continuous data and N (%) for categorical data unless stated otherwise. Analyses were performed using R version 2.13 (R Foundation for Statistical Computing, Vienna, Austria) and SAS version 9.3 (SAS Institute, Cary, NC).
Results
Development of SOPs for ICM performance
The studies supporting SOP development are summarized in the online Supporting Information, including examples of CF and non-CF tracings (Figure S1 in File S1), the effects of CFTR blockers on CFTR currents (Figure S2 in File S1), the impact of indomethacin on ICM parameters (Figure S3 in File S1), comparison of buffer conditions (Figure S4 in File S1), and stimulation with CFTR-activating conditions (Figure S5 in File S1). Guidelines for SOP development were based on conversations with experts in the field and published reports coupled with an overriding goal of a simple, straightforward assay that utilized common equipment and software [23,25,27,29,30]. All studies supporting SOP development were performed in non-CF subjects (n = 5-6 for each condition). Based upon these results, the reagents and conditions shown in Figure S1 in File S1 were used for the ensuing studies.
Prospective multi-center ICM in CF and non-CF subjects
A total of 45 non-CF and 12 F508del/F508del subjects were enrolled in this component of the study, and data was available from 44 non-CF subjects (%) and 11 CF subjects (%). Consent from one CF and one non-CF subject was withdrawn prior to biopsy (non-CF subject due to discovery of ulcerative colitis; CF subject due to painful hemorrhoids). In addition, six CF subjects were enrolled in a parallel protocol at one site (genotypes were F508del/F508del for five subjects, E60X/621+1G-T for the sixth subject). All study conditions were identical in this parallel study except for the use of Ringers buffer rather than RPMI 1640 buffer. Based on the similar ICM results comparing Ringer’s and RPMI buffer (Figure S4 in File S1), data from these additional CF subjects was included in the full analysis.
Subject demographics are shown in Table 1. As expected based on the enrollment populations, the non-CF subjects were 25 years older than the CF subjects, and had a more diverse racial and ethnic background. Sixty-five percent of CF subjects were male whereas forty-five percent of non-CF subjects were male. Enrollment was similar across the three study sites, ranging between 25%-44% of the total enrollment. A total of 291 biopsies were obtained from all study subjects, with 227 (78%) providing interpretable results based on central interpretation criteria (stable baseline current and tissue resistance). A total of six biopsies were inverted (2%) based on directional responses to agonists and post-analysis un-blinding to diagnosis (CF or non-CF). Of the 44 non-CF subjects, 37 had bowel preparation with polyethylene glycol (PEG), with a minority having pre-procedure preparation with magnesium citrate with or without PEG (n = 4) or not specified (n = 3). A total of five AEs were reported, including post-procedure bleeding (n = 4, all self-resolved) and pain from the procedure (n = 1, self-resolved). All AEs were assessed as probably related to the procedure by the gastroenterologist. The median number of biopsies per subject was four (range 2-8), and all interpretable biopsies were averaged to provide one value per subject for each of the ICM parameters.
Table 1. Demographics characteristics by study group.
| non CF | CF | All | |
|---|---|---|---|
| n = 44 | n = 17 | n = 61 | |
| Age - yrs | |||
| Mean (SD) | 56.0 (9.97) | 31.0 (8.59) | 49.1 (14.8) |
| Median | 54.4 | 28.2 | 51.3 |
| Min, Max | 26.0, 76.9 | 21.5, 50.1 | 21.5, 76.9 |
| Age distribution – no. (%) | |||
| 18 - ≤ 24 | 0 | 3 (18) | 3 (5) |
| 24 - ≤ 36 | 2 (5) | 9 (53) | 11 (18) |
| 36 - ≤ 48 | 4 (9) | 4 (24) | 8 (13) |
| > 48 | 38 (86) | 1 (6) | 39 (64) |
| Sex – no. (%) | |||
| Male | 20 (45) | 11 (65) | 31 (51) |
| Female | 24 (55) | 6 (35) | 30 (49) |
| Race – no. (%) | |||
| no. with race recorded | 44 | 17 | 55 |
| Caucasian | 35 (80) | 16 (94) | 45 (82) |
| African American | 8 (18) | 1 (6) | 9 (16) |
| Other | 1 (2) | 0 | 1 (2) |
The ICM results for the CF and non-CF subjects across all study sites are summarized in Table 2. Tissue resistance was similar for both the CF and non-CF groups (P = NS). Statistically significant differences in Isc responses between the CF and non-CF subjects were observed following amiloride (P = 0.002), forskolin/IBMX (P < 0.001), carbachol (P < 0.001), forskolin/IBMX + carbachol (P < 0.001), and bumetanide (P < 0.001). The absolute change in amiloride-sensitive current was greater in the non-CF subjects compared with the CF subjects, while the changes in all other ICM parameters were as predicted for the absence of CFTR-function in the CF compared with the non-CF sample.
Table 2. Summary of changes in Na+ and Cl- ICM currents (µA/cm2).
| CF | Non-CF | Difference | |
|---|---|---|---|
| Condition | n = 17 | n = 44 | (CF vs non-CF) |
| Change Amiloride (µA/cm2) | |||
| Mean (SD) | -10.5 (29.08) | -21.4 (27.79) | Mean diff = -11.0 |
| Median | -1.1 | -12.3 | 95% CI = (6.4, -28.4) |
| Min, Max | -112.5, 7.9 | -159, 6 | P = 0.002* |
| Change cAMP (forskolin/IBMX)** (µA/cm2) | |||
| Mean (SD) | -5.0 (12.67) | 99.5 (71.84) | Mean diff = 102.6 |
| Median | -0.9 | 92 | 95% CI = (128.0, 81.1) |
| Min, Max | -35.7, 16.4 | 6.1, 269.4 | P < 0.001* |
| Change CCh (µA/cm2) | |||
| Mean (SD) | 5.9 (10.21) | 102.2 (69.21) | Mean diff = 96.3 |
| Median | 3.9 | 97.26 | 95% CI = (118.7, 73.9) |
| Min, Max | -12.7, 28.1 | 0.8, 318.7 | P < 0.001* |
| Change cAMP + CCh (µA/cm2) | |||
| Mean (SD) | 0.8 (14.66) | 201.7 (131.98) | Mean diff = 200.9 |
| Median | -1.8 | 193.1 | 95% CI = (243.1, 158.6) |
| Min, Max | -30.3, 31.9 | 19.5, 588.1 | P < 0.001* |
| Change Bumetanide (µA/cm2) | |||
| Mean (SD) | 8.8 (9.7) | -35.8 (31.35) | Mean diff = -44.6 |
| Median | 6.4 | -27.4 | 95% CI = (-33.7, -55.6) |
| Min, Max | -2.6, 30.9 | -166.2, 3.3 | P < 0.001* |
cAMP, forskolin/ IBMX; CCh, carbochol; CI, confidence interval
P values were obtained using the Mann-Whitney test
Represents the primary clinical endpoint: difference in mean change in current for cAMP-stimulated tissue between CF and non-CF participants.
ICM data from 16 CF and 41 non-CF subjects were available for analysis.
The CFTR-dependent responses for non-CF subjects at each site (forskolin/IBMX, carbachol, forskolin/IBMX + carbachol) and their variances (within and across sites) are shown in Figure 1A–C and Table 3. Mean and median values for the three conditions were similar across the three study sites for the carbachol and forskolin/IBMX + carbachol-stimulated currents, and one site (S032) in general demonstrated higher variability for all three stimuli compared with the other two sites (S076 and S191). Table 3 summarizes the contribution of inter-site (between) and intra-site (within) variability to total variability for the same parameters shown in Figure 1. Greater than 90% of total variance for all three CFTR measures was due to intra-site variability, and not due to site-specific differences in assay conduct or results.
Figure 1. Individual ICM responses across study sites.
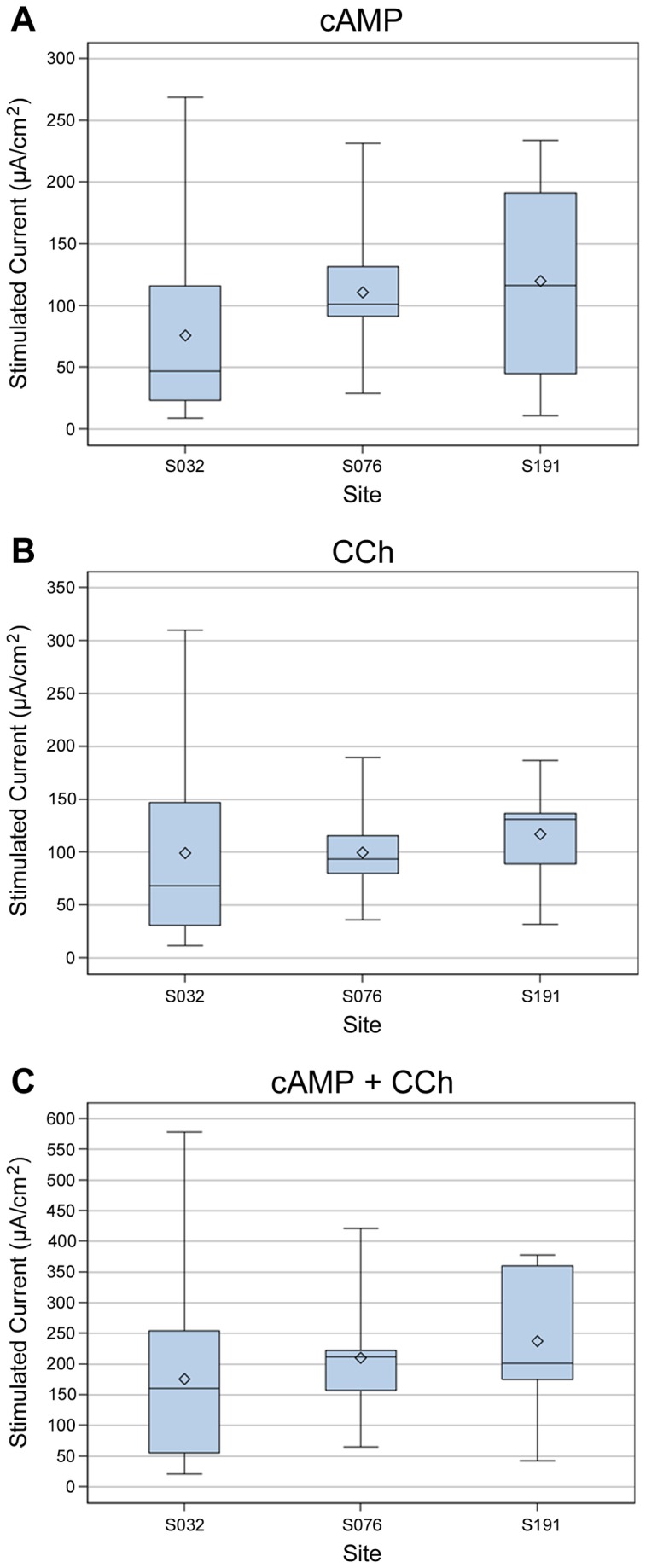
Boxplots of CFTR responses in non-CF subjects segregated by site (site identifiers S032, S076, S191). Whiskers are minimum and maximum values, boxes included data within 25th-75th percentiles, the horizontal line is the median, and the diamond is the mean. A. Change in Isc following cAMP stimulation (10 µM forskolin/100 µM IBMX). B. Change in Isc following carbachol (CCh) stimulation (100 µM, basolateral). C. Change in Isc following cAMP + CCh stimulation (10 µM forskolin, 100 µM IBMX, 100 µM CCh).
Table 3. Camparison of intersite and intrasite variability of CFTR-dependent currents in non-CF subjects using variances.
| Variable | Inter-Site Variability (% of Total) | Intra-Site Variability (% of Total) | Total Variability (% of Total) |
|---|---|---|---|
| cAMP | 384 (8.6) | 4069 (91.4) | 4453 (100) |
| CCh | 64 (1.6) | 3945 (98.4) | 4009 (100) |
| cAMP + CCh | 648 (4.5) | 13879 (95.5) | 14527 (100) |
cAMP, forskolin/ IBMX; CCh, carbochol
ROC curves are shown in Figure 2. All ICM parameters measured except the response to amiloride produced similar ROC curves, with AUC values ranging from 94–98%, indicating that the parameters differentiated CF subjects from non-CF subjects well. Of the parameters examined, the responses to forskolin/IBMX, carbachol, and forskolin/IBMX+carbachol had similar sensitivity. ICM was also capable of detecting partial CFTR activity. Figure 3 depicts the ICM tracing from one F508del/F508del subject (male, age 37 years, sweat Cl- = 113 mMol, pancreatic insufficient, FEV1 = 63%) showing features of functional CFTR, including a clear Cl- upward deflection following stimulation with forskolin/IBMX (compare with non-CF result in Figure S1 in File S1). The total change in Isc produced by forskolin/IBMX+carbachol was 15.8% of the mean wtCFTR response (non-CF subjects).
Figure 2. ROC curve analysis.

Note that CF participants are coded as one, and non-CF participants are coded as zero. Average true-positive rate is the sensitivity of the current to detect CF participants, whereas the average-false positive rate (one-specificity) marks the cutoff whereby non-CF participants are falsely determined as CF. AUC values varied from 0.946-0.978 for the three CFTR-specific measurements (forskolin/IBMX (cAMP), carbachol (CCh), cAMP + CCh).
Figure 3. Partial CFTR function detected in F508del/F508del CF subject.
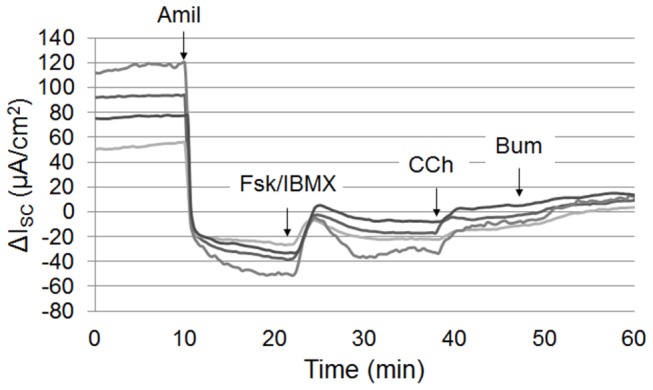
Representative tracing from an F508del/F508del subject with functional F508del CFTR. Adding forskolin/IBMX to raise cAMP increased the current > 30µA/cm2 which was further augmented by carbachol.
Based on the results of these pilot studies, we examined the power of ICM to detect increasing levels of CFTR function based on monitoring the ICM response to forskolin/IBMX, carbachol and forskolin/IBMX + carbachol. We compared this with the capacity of NPD to detect similar increases in CFTR activity (change in PD following perfusion with zero Cl- + 10 µM isoproterenol, a well-defined measure of CFTR activity used to successfully detect CFTR modulator activity in CF patients [14,15,18,20,41]. The NPD data was derived from qualification tracings submitted by 29 NPD study sites that were centrally interpreted at the Center for CFTR Detection at the University of Alabama at Birmingham (n = 144 non-CF tracings and 135 CF tracings) [12,18,20,42]. All subjects had a diagnosis of CF based on standard criteria (sweat Cl- > 60 mMol, organ manifestations of CF) and received CF care at the submitting study sites. Genotype information was not included with the NPD tracings. The results of these comparisons are summarized in Table 4. All three ICM parameters demonstrated substantially greater power than the NPD to detect low levels of CFTR function.
Table 4. Comparison of NPD and ICM power to detect increasing levels of CFTR function.
| CFTR Measurement | Mean Non-CF response | Mean CF response | Difference (SD) | Percent of non-CF response | Projected Treatment Effect | Estimated Effect Size | Number of Subjects |
|
|---|---|---|---|---|---|---|---|---|
| 80% Power | 90% Power | |||||||
| NPD: | ||||||||
| Zero Cl/Iso (mV) | -22.41 | 1.18 | 23.49 (3.94) | 10 | 2.35 | 0.59 | 19 | 26 |
| 20 | 4.70 | 1.19 | 6 | 8 | ||||
| 30 | 7.05 | 1.79 | 4 | 5 | ||||
| 40 | 9.40 | 2.39 | 3 | 4 | ||||
| 50 | 11.75 | 2.98 | 3 | 3 | ||||
| ICM: | ||||||||
| cAMP (µA/cm2) | -99.50 | -5.00 | 94.50 (12.67) | 10 | 9.45 | 0.75 | 13 | 17 |
| 20 | 18.90 | 1.49 | 5 | 6 | ||||
| 30 | 28.35 | 2.24 | 4 | 4 | ||||
| 40 | 37.80 | 2.98 | 3 | 3 | ||||
| 50 | 47.25 | 3.73 | 3 | 3 | ||||
| CCh (µA/cm2) | -102.20 | 5.90 | 108.10 (10.21) | 10 | 10.81 | 1.06 | 8 | 10 |
| 20 | 21.62 | 2.11 | 4 | 4 | ||||
| 30 | 32.43 | 3.18 | 3 | 3 | ||||
| 40 | 43.24 | 4.24 | 3 | 3 | ||||
| 50 | 54.05 | 5.29 | 3 | 3 | ||||
| 60 | 64.86 | 6.52 | 2 | 3 | ||||
| cAMP + CCh (µA/cm2) | -201.70 | 0.80 | 202.50 (14.66) | 10 | 20.25 | 1.38 | 5 | 7 |
| 20 | 40.50 | 2.76 | 3 | 4 | ||||
| 30 | 60.75 | 4.14 | 3 | 3 | ||||
| 40 | 81.00 | 5.53 | 3 | 3 | ||||
| 50 | 101.25 | 6.91 | 2 | 3 | ||||
Iso, isoproterenol; CCh, carbochol
CF patient tolerance of the rectal biopsy procedure was assessed during the study using a simple questionnaire. A total of eight CF subjects completed this questionnaire post-procedure. Seven of eight subjects chose to undergo the procedure without sedation. Subjects were asked to rate the different aspects of the procedure as ‘not unpleasant’, ‘sort of unpleasant’, or ‘very unpleasant’, including preparation (enema), sigmoidoscopy, biopsy, monitoring, and patient willingness to undergo a rectal biopsy as part of a future study. The majority of patients rated the enema and sigmoidoscopy as ‘sort of unpleasant’ (62% and 71%, respectively), while the majority rated the biopsy and monitoring as ‘not unpleasant’ (71% and 100%, respectively). None of the subjects rated any of the aspects of the procedure as ‘very unpleasant’, and all subjects responded that they were willing to undergo rectal biopsy as part of future CF studies.
Effects of cold tissue storage on ICM parameters
Since ICM performance requires significant onsite training and equipment, we examined whether the electrophysiologic aspects of ICM could be centralized. In preparation for these studies, we examined the effects of different storage conditions on tissue viability and CFTR activity in non-CF subjects. First, four separate media conditions for cold storage were compared (summarized in Figure S6 in File S1). The results indicated that biopsies stored at 4°C for 18 hours in RPMI 1640 media retained consistent CFTR dependent responses to agonists. Subsequently, 17 non-CF subjects underwent forceps-based biopsy, with half of the biopsies studied immediately and the other half studied after onsite storage at 4°C (RPMI media + antibiotics) for 18-24 hours. The results are summarized in Table 5. The responses to forskolin/IBMX (10/100 µM), carbachol (100 µM), and forskolin/IBMX + carbachol following cold storage were reduced relative to responses in fresh tissue (P = 0.026, 0.046, and 0.039, respectively). The responses after cold storage were 44%, 47.5%, and 47.3% of the fresh-tissue responses for the three respective stimulus conditions (forskolin/IBMX, carbachol, forskolin/IBMX + carbachol).
Table 5. Effects of cold storage on ICM parameters (single site).
| Change in Isc µA/cm2 – Least Square Means (Upper C.L., Lower C.L.) | |||
|---|---|---|---|
| Tissue | *cAMP | *CCh | *cAMP + CCh |
| Fresh | 65.29 (38.23, 102.81) | 88.07 (62.34, 120.06) | 155.85 (106.34, 218.75) |
| Stored | 28.70 (15.88, 47.04) | 41.91 (22.03, 71.16) | 73.80 (41.02, 120.58) |
cAMP, forskolin/ IBMX; CCh, carbochol
P < 0.05 for comparisons between fresh and stored for the different stimuli (n = 17 non-CF subjects)
Variance of ICM CFTR parameters measured in one subject at two study sites
Based on the observation that cold stored rectal biopsy tissue retained significant CFTR-dependent currents activity (Table 5), we examined the intrasubject variance of ICM parameters, testing biopsies from one non-CF subject studied at two ICM sites simultaneously. 14 non-CF subjects underwent forceps-based biopsy, with half of biopsies stored onsite (4-8°C) in RPMI 1640 media and the other half sent on ice overnight in RPMI media to a second ICM study site. Biopsies were then dissected and mounted in Ussing chambers at the two sites and studied simultaneously (range of 18-24 hours post-biopsy). The ICC coefficients for the three CFTR-dependent parameters (forskolin/IBMX, carbachol, and forskolin/IBMX + carbachol stimulated currents) were 0.403, 0.5144, and 0.494, respectively between the two sites. None of the parameters had differences between sites that reached statistical significance. Bland-Altman plots are shown in Figure 4A–C, demonstrating that the three ICM parameters had similar variance between sites independent of the magnitude of stimulated Isc.
Figure 4. Bland-Altman plots of ICM responses for biopsies from single subjects studied at two sites simultaneously after cold storage.
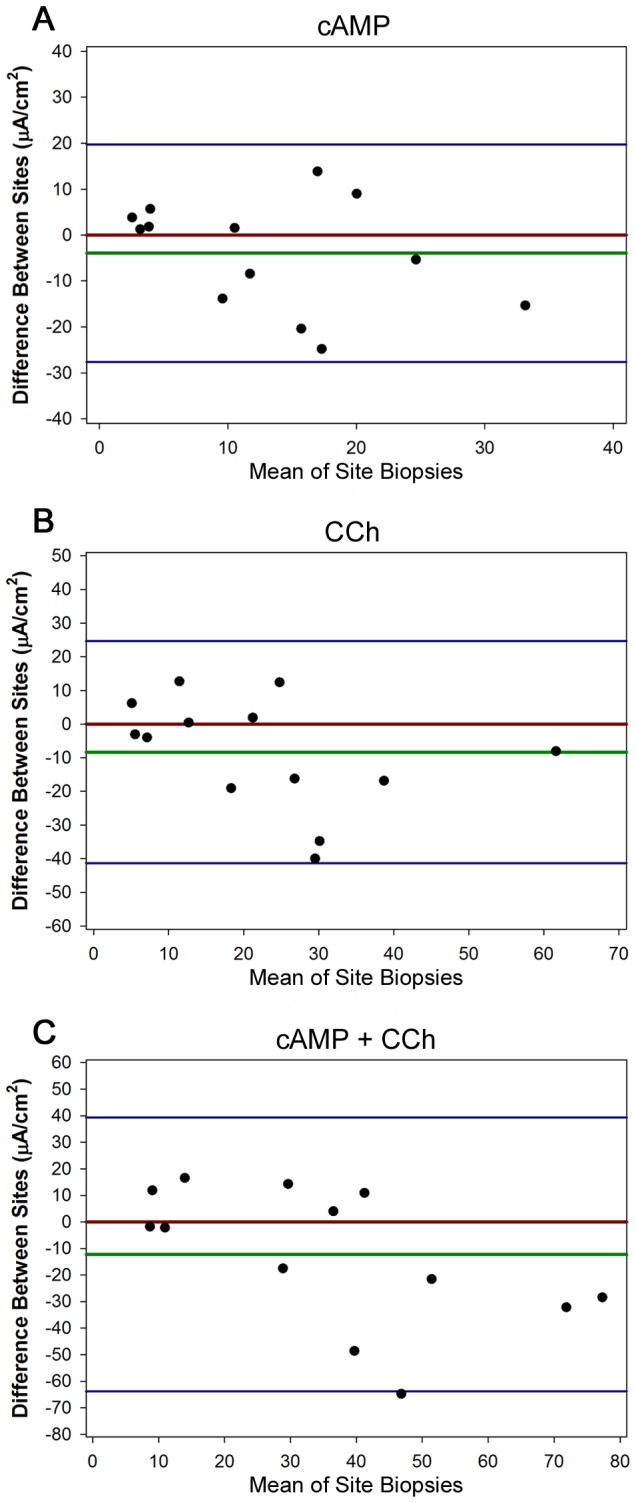
Difference between A. forskolin/IBMX (cAMP), B. carbachol, or C. forskolin/IBMX (cAMP + carbachol) responses at site of biopsy origin and test site. Each dot is the mean ICM response for one subject (both sites). The X axis is the mean of the response (both sites), and the Y axis is the difference between the means at the two sites. The red line is the hypothetical zero difference, and the green line is the actual mean difference. Blue lines are ± 2 SDs.
Comparison of CFTR activity in forceps and suction biopsies
Three non-CF subjects underwent both forceps-based and suction-based biopsies simultaneously, with subsequent ICM performance onsite. The Isc responses to forskolin/IBMX, carbachol, and forskolin/IBMX + carbachol are shown in Figure S7 in File S1, including individual biopsy results and mean results for the three subjects (n = 12-14 biopsies per condition). No significant differences in CFTR dependent currents were observed based on the nature of biopsy for the three parameters, but there was a trend towards higher resistance in forceps biopsies relative to suction biopsies [22.82 ohm·cm2 (±8.85) vs 13.21 ohm·cm2 (±6.55) following subtraction of fluid resistance, P = 0.056].
Discussion
In this prospective study, we used common SOPs for multi-center ICM performance and tested their performance in CF and non-CF subjects. Our data indicated that multiple ICM parameters performed across three study sites clearly distinguished between the CF and non-CF condition. Most notably were changes in Isc produced by forskolin/IBMX, carbachol, forskolin/IBMX + carbachol, and bumetanide (Table 2). All of these parameters are dependent on CFTR at the apical plasma membrane. In addition, all of these electrophysiologic parameters appeared to have similar sensitivity to discriminate between CF subjects with severe mutations and non-CF subjects (ROC characteristics, Figure 2). This redundancy provided further assurance of discrimination by CFTR function, as numerous measures showed similar behavior by ROC analysis. The one exception was amiloride-sensitive currents, which were not particularly discriminatory between CF and non-CF subjects (see Figure 2A). This is not entirely unexpected since ENaC regulation varies throughout the large intestine and is dependent in part on local protease activity [43], as well as aldosterone and volume status. Our results using voltage-clamp conditions were in good agreement with results reported using open-circuit conditions, suggesting that the method of monitoring CFTR was not a major determinant of the measured CFTR dependent currents [25]. Due to the large difference in ICM responses between ‘severe’ CF and non-CF subjects with relatively low variance (Tables 2-4), the power of the assay to detect low levels of CFTR activity compared favorably with the NPD. Most of the variance observed in ICM represented differences within sites and not between sites (Figure 1 and Table 3). Intra-site variance for CFTR-dependent measures could be due to a number of contributors, including biologic variability between subjects, differences in biopsy depth, tissue injury during dissection, mucosal visualization during the biopsy procedure, and so on. To ensure optimal assay performance, standardization of those aspects of ICM that can be standardized is highly recommended (e.g., equipment, reagents, software), as are ongoing efforts to minimize the contributions of site variables (e.g., biopsy techniques, tissue integrity, dissection). In addition, other stimuli and ion transport blockers may be considered to reduce variability of CFTR dependent responses between subjects (e.g., histamine and DIDS to isolate CFTR activity).
Previous published work has demonstrated that low levels of murine F508del CFTR can be monitored by ICM, including ex vivo treatment with putative F508del corrective agents or conditions [35,36,44,45]. In addition, Bedwell and colleagues have shown that transgenic mice carrying the human G542X mutation in CFTR that are treated with suppressors of premature termination codons (aminoglycosides, ataluren) have detectable CFTR function in intestinal tissue studied by ICM [46–49]. These results in CF animal models support the notion that monitoring rectal biopsy current is a sensitive assay to detect restored CFTR function, either in response to ex vivo treatment of tissue with CFTR modulators (i.e., as a model system to test modulator activity) or following in vivo treatment (i.e., as an outcome measure for clinical trials). Future studies confirming the activity of CFTR modulators in rectal biopsies from CF patients (treated in vivo or ex vivo) will be necessary to determine definitively whether ICM is capable of detecting restored function of human CFTR carrying disease-causing mutations in human tissue. Rectal biopsies have been used to monitor F508del CFTR expression in one CFTR modulator trial (VX-809), using rectal biopsies to assess the maturation of F508del CFTR by immunoblot [12]. Thirty three of 89 enrolled subjects voluntarily underwent this optional endpoint in the VX-809 trial (biopsies prior to and during treatment), supporting the feasibility of incorporating rectal biopsies into interventional CF clinical studies. ICM was not included in the analysis of these biopsies, but evidence suggests that electrophysiologic measures are more sensitive than biochemical assays to detect low levels of mature F508del CFTR [29,50].
The studies examining CFTR responses following cold storage demonstrated that this maneuver reduced currents substantially (Table 5), but still provided CFTR-dependent currents that were outside the CF range for fresh tissue (Table 2). Biopsies from single subjects studied after cold storage at two sites demonstrated moderate correlation between sites and similar variance over a wide range of detected CFTR activity (Figure 4A–C), supporting the hypothesis that centralized performance of the electrophysiologic aspects of ICM may be potentially feasible. To optimize centralized ICM performance, minimizing the time between biopsy and electrophysiologic measurements at the second site are likely critical, including time between biopsy and transport, and the nature of sample transportation (e.g., next morning delivery). Finally, the method of biopsy (suction or forceps) did not clearly influence the capacity to detect CFTR-dependent currents (Figure S7 in File S1). Although these studies are limited in number, they do suggest that sites have flexibility in the nature of rectal biopsy performance.
Previous studies have helped to define stimuli that reflect CFTR in the colon, including ENaC blockade with amiloride, stimulation with cAMP-elevating agents to activate CFTR, and stimulation of basolateral muscarinic receptors that activate basolateral K+ channels to hyperpolarize the cell and drive Cl- exit across the colonocyte apical membrane [23–25,27,51]. Increasing transepithelial Cl- flux via stimulation of basolateral K+ channels is a unique feature of ICM compared with other CFTR biomarkers (e.g., sweat Cl- or NPD), providing an example of how access to the basolateral membrane increases the flexibility in reagent use to optimize CFTR detection.
The protocol developed in the current study was based on features previously established by leading laboratories in intestinal physiology, incorporating aspects from different practices into the described ICM SOP. Based on communications with expertise in the field, onsite experience, and the need to standardize equipment, all sites utilized common voltage clamps, Ussing chambers, tissue sliders, and software from a single source. The recirculating chambers (as opposed to continuous volume-exchange chambers) were selected based on the availability of standardized equipment and servicing. Data generated at sites could then be sent directly to the central reading site for interpretation in a blinded fashion without concerns of software incompatibilities or conversion. Our results compare favorably with two recent studies examining ICM in CF in non-CF subjects. Hirtz and colleagues demonstrated that ICM was capable of clearly segregating non-CF subjects from CF patients with either partial or non-functional CFTR mutations [25]. The cAMP-stimulated currents reported in non-CF controls and patients with non-functional CFTR mutations were similar to those reported here (monitored under open circuit conditions). In a more recent study reported by Derichs and colleagues, currents were measured in 309 biopsies from 130 subjects with pancreatic insufficient CF, pancreatic sufficient CF, an unclear CF diagnosis, and healthy controls [30]. A cutoff of -34 µA/cm2 was described to discriminate between a CF and non-CF diagnosis. In agreement with this report, our results defined 95% CI surrounding the CF response to forskolin/IBMX + carbachol of -30.3 to +31.9 µA/cm2.
Another goal of the project was to develop conditions and a reagent sequence that would maximize detection of CFTR activity in a rapid fashion. The results described in Figures S1-S5 in File S1 support SOPs that include the pretreatment of samples with indomethacin, that CFTR dependent currents were similar when using either RPMI or Ringer’s buffer, and that sequential stimulation with reagents enhanced CFTR detection. While the durability of modulator drug effects on mutant CFTR in biopsied rectal tissue are unknown, preclinical studies with F508del CFTR correctors indicate that the half-life of F508del CFTR at the airway cell membrane is several hours [52–54]. Thus, the timeline for ex vivo assessment of CFTR developed in these studies seems unlikely to limit the capacity of ICM to detect corrected F508del CFTR at the colonocyte cell membrane. Unfortunately, neither CFTRinh172 nor GLYH101 were consistently effective blockers of CFTR currents in our studies (Figure S2 in File S1). The only anion channel that has been shown to play a major role in the colonocyte apical membrane to date is CFTR ( [55]). We speculate that mucus (or other molecules) on the apical surface of the colonic epithelium may bind the lipophilic blockers or limit access to CFTR through other molecular interactions. In addition, CFTR expression in the colon is highest in the base cells of the colonic crypts, which may limit accessibility of channel blockers [56]. The Na+/K+/2Cl- cotransporter blocker bumetanide was thus chosen to inhibit the stimulated currents, although its blockade also was incomplete. The direction of Isc inflection following bumetanide differed between the CF and non-CF subjects, likely reflecting the nature of the dominant operative ion transport pathway that was sensitive to bumetanide (CFTR-dependent Cl- secretion in non-CF subjects, K+ secretion in CF). This feature, coupled with the direction of inflection following amiloride (which defines the apical membrane of both CF and non-CF subjects) helped provide assurance of tissue mounting and underlying diagnosis. An example of this is shown in Figure 3, in which the data support the hypothesis that this subject has detectable F508del CFTR at the colonic cell membrane. The ICM shows a strong downward deflection with amiloride (confirming correct orientation), a significant upward deflection in response to forskolin/IBMX, and a mixed response to carbachol. Limitations of this study include the relatively small number of CF subjects enrolled, the lack of CF patients with pancreatic sufficiency and/or partial function mutations, and the lack of pediatric subjects. As this study was performed solely for the purpose of assay development across three sites and was not designed to provide diagnostic information to the study population, enrollment of large numbers of adult or pediatric CF patients was not thought to be ethical. In addition, insufficient numbers of adult patients with pancreatic sufficiency or partial function mutations were available to draw conclusions regarding ICM performance in this CF subpopulation. In addition, the lack of acute efficacy of CFTR blockers (CFTRinh172 and GLYH101, Figure S2 in File S1) and inconsistent increases in sodium absorption in CF biopsies (Figure 2, Table 2, Figure S1 in File S1) could be limitations to use of ICM as a CFTR biomarker in modulator trials. Despite these limitations, our multi-center results demonstrate good agreement in ICM parameters with single center studies that have included larger numbers of both adult and pediatric CF patients and support the hypothesis that multi-center ICM may be a feasible endpoint for future clinical trials.
In summary, our results indicate that SOPs for ICM performance can be developed across three centers, that multi-center ICM can discriminate between CF patients with severe CFTR mutations and non-CF subjects, and that ICM (performed with common SOPs) can detect partial CFTR function in CF patients. The power of multi-center ICM to detect low levels of CFTR activity compares favorably with that of multi-center NPD. CFTR activity was detectable several hours post-biopsy with moderate correlation between study sites, suggesting that the electrophysiologic aspects of ICM can potentially be centralized in the future. The assay expands upon available CFTR biomarkers by isolating CFTR currents, providing flexibility in reagents, and offering numerous CFTR-specific features that discriminate between CF and non-CF subjects. Together, these data demonstrate that ICM is a feasible biomarker for CFTR and that further development is warranted for application to clinical trials.
Supporting Information
Contains Figures S1-S7. Figure S1, Examples of ICM tracings for (A) non-CF and (B) CF patients. Figure S2, Representative examples of CFTR inhibitor effects on CFTR currents in rectal biopsies. Figure S3, Effects of indomethacin on ICM parameters. Figure S4, Comparison of ICM parameters in Ringer’s buffer and RPMI + 25 mM HCO3 buffer. Figure S5, Comparison of sequential vs simultaneous agonist addition on CFTR detection by ICM. Figure S6, Comparison of four cold storage conditions on rectal biopsy performance. Figure S7, Comparison of CFTR-dependent ICM responses from forceps and suction biopsies in non-CF subjects.
(DOC)
Acknowledgments
The study team is indebted to the research coordinators involved in the study (Gina Sabbatini and Valerie Eubanks-Tarn at UAB, Nadia Bendahmane and Jessica Hores at UNC, Mary Teresi at Univ. of Iowa, Lorrie Duan at CCHMC) and the collaborating gastroenterologists (Sajan Peters at UAB, Evan Dellon at UNC, Jeff Fields at Univ. of Iowa, Joseph Palermo at CCHMC).
We also would like to thank experts in the field for their candid input regarding ICM performance, including Dr. Margarida Amaral and Marisa Sousa (University of Lisbon), Dr. Marcus Mall (University of Heidelberg), Dr. Burkhard Tümmler (University of Hannover), and Dr. Hugo de Jonge (Erasmus University). The authors are grateful to J. Denise Wetzel, CCHMC Medical Writer, for critical review of the manuscript.
Funding Statement
This study was supported by the National Institutes of Health (grants P30 DK065988 to SHD, SEG, and NLQ, P30 DK072482 and U UL1025777 to LF and SMR, and U01 HL102288 to DBH, PHK, and TDS) and the Cystic Fibrosis Foundation and Cystic Fibrosis Foundation Therapeutics (grants AMIN09YO and R457-CR11 to JPC, CLANCY05Y0 to SMR and LF, and GABRIE08AO to SHD, SEG, and NLQ). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Rowe SM, Miller S, Sorscher EJ (2005) Cystic fibrosis. N Engl J Med 352: 1992-2001. doi:10.1056/NEJMra043184. PubMed: 15888700. [DOI] [PubMed] [Google Scholar]
- 2. Kerem B, Rommens JM, Buchanan JA, Markiewicz D, Cox TK et al. (1989) Identification of the cystic fibrosis gene: genetic analysis. Science 245: 1073-1080. doi:10.1126/science.2570460. PubMed: 2570460. [DOI] [PubMed] [Google Scholar]
- 3. Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R et al. (1989) Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA [published erratum appears in Science 1989 Sep 29; 245(4925):1437]. Science 245: 1066-1073. doi:10.1126/science.2475911. PubMed: 2475911. [DOI] [PubMed] [Google Scholar]
- 4. Rommens JM, Iannuzzi MC, Kerem B, Drumm ML, Melmer G et al. (1989) Identification of the cystic fibrosis gene: chromosome walking and jumping. Science 245: 1059-1065. doi:10.1126/science.2772657. PubMed: 2772657. [DOI] [PubMed] [Google Scholar]
- 5. Boucher RC (2002) An overview of the pathogenesis of cystic fibrosis lung disease. Adv Drug Deliv Rev 54: 1359-1371. doi:10.1016/S0169-409X(02)00144-8. PubMed: 12458149. [DOI] [PubMed] [Google Scholar]
- 6. Boucher RC (2004) New concepts of the pathogenesis of cystic fibrosis lung disease. Eur Respir J 23: 146-158. doi:10.1183/09031936.03.00057003. PubMed: 14738247. [DOI] [PubMed] [Google Scholar]
- 7. Boucher RC (2007) Airway surface dehydration in cystic fibrosis: pathogenesis and therapy. Annu Rev Med 58: 157-170. doi:10.1146/annurev.med.58.071905.105316. PubMed: 17217330. [DOI] [PubMed] [Google Scholar]
- 8. Riordan JR (2008) CFTR function and prospects for therapy. Annu Rev Biochem 77: 701-726. doi:10.1146/annurev.biochem.75.103004.142532. PubMed: 18304008. [DOI] [PubMed] [Google Scholar]
- 9. Harrington MA, Kopito RR (2002) Cysteine residues in the nucleotide binding domains regulate the conductance state of CFTR channels. Biophys J 82: 1278-1292. doi:10.1016/S0006-3495(02)75484-2. PubMed: 11867445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kopito RR (1999) Biosynthesis and degradation of CFTR. Physiol Rev 79: S167-S173. PubMed: 9922380. [DOI] [PubMed] [Google Scholar]
- 11. Ward CL, Omura S, Kopito RR (1995) Degradation of CFTR by the ubiquitin-proteasome pathway. Cell 83: 121-127. doi:10.1016/0092-8674(95)90240-6. PubMed: 7553863. [DOI] [PubMed] [Google Scholar]
- 12. Clancy JP, Rowe SM, Accurso FJ, Aitken ML, Amin RS et al. (2012) Results of a phase IIa study of VX-809, an investigational CFTR corrector compound, in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation. Thorax 67: 12-18. doi:10.1136/thoraxjnl-2011-200393. PubMed: 21825083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Rowe SM, Accurso F, Clancy JP (2007) Detection of cystic fibrosis transmembrane conductance regulator activity in early-phase clinical trials. Proc Am Thorac Soc 4: 387-398. doi:10.1513/pats.200703-043BR. PubMed: 17652506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kerem E, Hirawat S, Armoni S, Yaakov Y, Shoseyov D et al. (2008) Effectiveness of PTC124 treatment of cystic fibrosis caused by nonsense mutations: a prospective phase II trial. Lancet 372: 719-727. doi:10.1016/S0140-6736(08)61168-X. PubMed: 18722008. [DOI] [PubMed] [Google Scholar]
- 15. Sermet-Gaudelus I, Boeck KD, Casimir GJ, Vermeulen F, Leal T et al. (2010) Ataluren (PTC124) induces cystic fibrosis transmembrane conductance regulator protein expression and activity in children with nonsense mutation cystic fibrosis. Am J Respir Crit Care Med 182: 1262-1272. doi:10.1164/rccm.201001-0137OC. PubMed: 20622033. [DOI] [PubMed] [Google Scholar]
- 16. Rubenstein RC, Zeitlin PL (1998) Use of protein repair therapy in the treatment of cystic fibrosis. Curr Opin Pediatr 10: 250-255. doi:10.1097/00008480-199806000-00005. PubMed: 9716885. [DOI] [PubMed] [Google Scholar]
- 17. Rubenstein RC, Zeitlin PL (1998) A pilot clinical trial of oral sodium 4-phenylbutyrate (Buphenyl) in deltaF508-homozygous cystic fibrosis patients: partial restoration of nasal epithelial CFTR function. Am J Respir Crit Care Med 157: 484-490. doi:10.1164/ajrccm.157.2.9706088. PubMed: 9476862. [DOI] [PubMed] [Google Scholar]
- 18. Accurso FJ, Rowe SM, Clancy JP, Boyle MP, Dunitz JM et al. (2010) Effect of VX-770 in persons with cystic fibrosis and the G551D-CFTR mutation. N Engl J Med 363: 1991-2003. doi:10.1056/NEJMoa0909825. PubMed: 21083385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ahrens RC, Standaert TA, Launspach J, Han SH, Teresi ME et al. (2002) Use of nasal potential difference and sweat chloride as outcome measures in multicenter clinical trials in subjects with cystic fibrosis. Pediatr Pulmonol 33: 142-150. doi:10.1002/ppul.10043. PubMed: 11802252. [DOI] [PubMed] [Google Scholar]
- 20. Solomon GM, Konstan MW, Wilschanski M, Billings J, Sermet-Gaudelus I et al. (2010) An international randomized multicenter comparison of nasal potential difference techniques. Chest 138: 919-928. doi:10.1378/chest.10769. PubMed: 20472865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Knowles MR, Paradiso AM, Boucher RC (1995) In vivo nasal potential difference: techniques and protocols for assessing efficacy of gene transfer in cystic fibrosis. Hum Gene Ther 6: 445-455. doi:10.1089/hum.1995.6.4-445. PubMed: 7542031. [DOI] [PubMed] [Google Scholar]
- 22. Schüler D, Sermet-Gaudelus I, Wilschanski M, Ballmann M, Dechaux M et al. (2004) Basic protocol for transepithelial nasal potential difference measurements. J Cyst Fibros 3 Suppl 2: 151-155. doi:10.1016/j.jcf.2004.03.009. PubMed: 15463949. [DOI] [PubMed] [Google Scholar]
- 23. Hug MJ, Derichs N, Bronsveld I, Clancy JP (2011) Measurement of ion transport function in rectal biopsies. Methods Mol Biol 741: 87-107. doi:10.1007/978-1-61779-117-8_7. PubMed: 21594780. [DOI] [PubMed] [Google Scholar]
- 24. Barreto C, Mall M, Amaral MD (2004) Assessment of CFTR function in native epithelia for the diagnosis of cystic fibrosis. Pediatr Pulmonol Suppl 26: 243 PubMed: 15029663. [DOI] [PubMed] [Google Scholar]
- 25. Hirtz S, Gonska T, Seydewitz HH, Thomas J, Greiner P et al. (2004) CFTR Cl- channel function in native human colon correlates with the genotype and phenotype in cystic fibrosis. Gastroenterology 127: 1085-1095. doi:10.1053/j.gastro.2004.07.006. PubMed: 15480987. [DOI] [PubMed] [Google Scholar]
- 26. Mall M, Kreda SM, Mengos A, Jensen TJ, Hirtz S et al. (2004) The DeltaF508 mutation results in loss of CFTR function and mature protein in native human colon. Gastroenterology 126: 32-41. doi:10.1053/j.gastro.2003.10.049. PubMed: 14699484. [DOI] [PubMed] [Google Scholar]
- 27. De Jonge HR, Ballmann M, Veeze H, Bronsveld I, Stanke F et al. (2004) Ex vivo CF diagnosis by intestinal current measurements (ICM) in small aperture, circulating Using chambers. J Cyst Fibros 3 Suppl 2: 159-163. doi:10.1016/j.jcf.2004.05.034. PubMed: 15463951. [DOI] [PubMed] [Google Scholar]
- 28. Bronsveld I, Mekus F, Bijman J, Ballmann M, de Jonge HR et al. (2001) Chloride conductance and genetic background modulate the cystic fibrosis phenotype of Delta F508 homozygous twins and siblings. J Clin Invest 108: 1705-1715. doi:10.1172/JCI200112108. PubMed: 11733566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bronsveld I, Mekus F, Bijman J, Ballmann M, Greipel J et al. (2000) Residual chloride secretion in intestinal tissue of deltaF508 homozygous twins and siblings with cystic fibrosis. The European CF Twin and Sibling Study Consortium. Gastroenterology 119: 32-40. doi:10.1053/gast.2000.8524. PubMed: 10889152. [DOI] [PubMed] [Google Scholar]
- 30. Derichs N, Sanz J, Von Kanel T, Stolpe C, Zapf A et al. (2010) Intestinal current measurement for diagnostic classification of patients with questionable cystic fibrosis: validation and reference data. Thorax 65: 594-599. doi:10.1136/thx.2009.125088. PubMed: 20627915. [DOI] [PubMed] [Google Scholar]
- 31. Meyerholz DK, Stoltz DA, Pezzulo AA, Welsh MJ (2010) Pathology of gastrointestinal organs in a porcine model of cystic fibrosis. Am J Pathol 176: 1377-1389. doi:10.2353/ajpath.2010.090849. PubMed: 20110417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Stoltz DA, Meyerholz DK, Pezzulo AA, Ramachandran S, Rogan MP et al. (2010) Cystic fibrosis pigs develop lung disease and exhibit defective bacterial eradication at birth. Sci Transl Med 2: 29ra31 PubMed: 20427821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Scholte BJ, Davidson DJ, Wilke M, De Jonge HR (2004) Animal models of cystic fibrosis. J Cyst Fibros 3 Suppl 2: 183-190. doi:10.1016/j.jcf.2004.05.039. PubMed: 15463956. [DOI] [PubMed] [Google Scholar]
- 34. Charizopoulou N, Wilke M, Dorsch M, Bot A, Jorna H et al. (2006) Spontaneous rescue from cystic fibrosis in a mouse model. BMC Genet 7: 18. doi:10.1186/1471-2156-7-18. PubMed: 16571105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Robert R, Carlile GW, Liao J, Balghi H, Lesimple P et al. (2010) Correction of the Delta phe508 cystic fibrosis transmembrane conductance regulator trafficking defect by the bioavailable compound glafenine. Mol Pharmacol 77: 922-930. doi:10.1124/mol.109.062679. PubMed: 20200141. [DOI] [PubMed] [Google Scholar]
- 36. French PJ, van Doorninck JH, Peters RH, Verbeek E, Ameen NA et al. (1996) A delta F508 mutation in mouse cystic fibrosis transmembrane conductance regulator results in a temperature-sensitive processing defect in vivo. J Clin Invest 98: 1304-1312. doi:10.1172/JCI118917. PubMed: 8823295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Mall M, Bleich M, Schürlein M, Kühr J, Seydewitz HH et al. (1998) Cholinergic ion secretion in human colon requires coactivation by cAMP. Am J Physiol 275: G1274-G1281. PubMed: 9843763. [DOI] [PubMed] [Google Scholar]
- 38. Sousa M, Servidoni MF, Vinagre AM, Ramalho AS, Bonadia LC et al. (2012) Measurements of CFTR-mediated Cl- secretion in human rectal biopsies constitute a robust biomarker for Cystic Fibrosis diagnosis and prognosis. PLOS ONE 7: e47708. doi:10.1371/journal.pone.0047708. PubMed: 23082198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Bartko JJ (1966) The intraclass correlation coefficient as a measure of reliability. Psychol Rep 19: 3-11. doi:10.2466/pr0.1966.19.1.3. PubMed: 5942109. [DOI] [PubMed] [Google Scholar]
- 40. Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1: 307-310. PubMed: 2868172. [PubMed] [Google Scholar]
- 41. Wilschanski M, Yahav Y, Yaacov Y, Blau H, Bentur L et al. (2003) Gentamicin-induced correction of CFTR function in patients with cystic fibrosis and CFTR stop mutations. N Engl J Med 349: 1433-1441. doi:10.1056/NEJMoa022170. PubMed: 14534336. [DOI] [PubMed] [Google Scholar]
- 42. Liu B, Hathorne H, Hill A, Hovick G, Cohen M et al. (2010) Normative values and receiver operating characteristics of NPD for diagnostic measurements. Pediatr Pulmonolology 303: A247. [Google Scholar]
- 43. Farkas K, Yeruva S, Rakonczay Z Jr., Ludolph L, Molnár T et al. (2011) New therapeutic targets in ulcerative colitis: the importance of ion transporters in the human colon. Inflamm Bowel Dis 17: 884-898. doi:10.1002/ibd.21432. PubMed: 20722063. [DOI] [PubMed] [Google Scholar]
- 44. Xiao F, Li J, Singh AK, Riederer B, Wang J et al. (2012) Rescue of epithelial HCO3- secretion in murine intestine by apical membrane expression of the cystic fibrosis transmembrane conductance regulator mutant F508del. J Physiol 590: 5317-5334. doi:10.1113/jphysiol.2012.232124. PubMed: 22802588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Wilke M, Buijs-Offerman RM, Aarbiou J, Colledge WH, Sheppard DN et al. (2011) Mouse models of cystic fibrosis: phenotypic analysis and research applications. J Cyst Fibros 10 Suppl 2: S152-S171. doi:10.1016/S1569-1993(11)60020-9. PubMed: 21658634. [DOI] [PubMed] [Google Scholar]
- 46. Du M, Jones JR, Lanier J, Keeling KM, Lindsey JR et al. (2002) Aminoglycoside suppression of a premature stop mutation in a Cftr-/- mouse carrying a human CFTR-G542X transgene. J Mol Med 80: 595-604. doi:10.1007/s00109-002-0363-1. PubMed: 12226741. [DOI] [PubMed] [Google Scholar]
- 47. Du M, Keeling KM, Fan L, Liu X, Kovaçs T et al. (2006) Clinical doses of amikacin provide more effective suppression of the human CFTR-G542X stop mutation than gentamicin in a transgenic CF mouse model. J Mol Med 84: 573-582. doi:10.1007/s00109-006-0045-5. PubMed: 16541275. [DOI] [PubMed] [Google Scholar]
- 48. Du M, Liu X, Welch EM, Hirawat S, Peltz SW et al. (2008) PTC124 is an orally bioavailable compound that promotes suppression of the human CFTR-G542X nonsense allele in a CF mouse model. Proc Natl Acad Sci U S A 105: 2064-2069. doi:10.1073/pnas.0711795105. PubMed: 18272502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Du M, Keeling KM, Fan L, Liu X, Bedwell DM (2009) Poly-L-aspartic acid enhances and prolongs gentamicin-mediated suppression of the CFTR-G542X mutation in a cystic fibrosis mouse model. J Biol Chem 284: 6885-6892. PubMed: 19136563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Van Goor F, Hadida S, Grootenhuis PD, Burton B, Stack JH et al. (2011) Correction of the F508del-CFTR protein processing defect in vitro by the investigational drug VX-809. Proc Natl Acad Sci U S A 108: 18843-18848. doi:10.1073/pnas.1105787108. PubMed: 21976485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Kunzelmann K, Mall M (2002) Electrolyte transport in the mammalian colon: mechanisms and implications for disease. Physiol Rev 82: 245-289. PubMed: 11773614. [DOI] [PubMed] [Google Scholar]
- 52. Varga K, Goldstein RF, Jurkuvenaite A, Chen L, Matalon S et al. (2008) Enhanced cell-surface stability of rescued DeltaF508 cystic fibrosis transmembrane conductance regulator (CFTR) by pharmacological chaperones. Biochem J 410: 555-564. doi:10.1042/BJ20071420. PubMed: 18052931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Bebök Z, Tousson A, Schwiebert LM, Venglarik CJ (2001) Improved oxygenation promotes CFTR maturation and trafficking in MDCK monolayers. Am J Physiol Cell Physiol 280: C135-C145. PubMed: 11121385. [DOI] [PubMed] [Google Scholar]
- 54. Collawn JF, Bebok Z, Matalon S (2009) Search and rescue: finding ways to correct deltaF508 CFTR. Am J Respir Cell Mol Biol 40: 385-387. doi:10.1165/rcmb.2008-0006ED. PubMed: 19293344. [DOI] [PubMed] [Google Scholar]
- 55. Greger R (2000) Role of CFTR in the colon. Annu Rev Physiol 62: 467-491. doi:10.1146/annurev.physiol.62.1.467. PubMed: 10845099. [DOI] [PubMed] [Google Scholar]
- 56. Umar S, Scott J, Sellin JH, Dubinsky WP, Morris AP (2000) Murine colonic mucosa hyperproliferation. I. Elevated CFTR expression and enhanced cAMP-dependent. p. Cl(-) secretion. Am J Physiol Gastrointest Liver Physiol 278: G753-764. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Contains Figures S1-S7. Figure S1, Examples of ICM tracings for (A) non-CF and (B) CF patients. Figure S2, Representative examples of CFTR inhibitor effects on CFTR currents in rectal biopsies. Figure S3, Effects of indomethacin on ICM parameters. Figure S4, Comparison of ICM parameters in Ringer’s buffer and RPMI + 25 mM HCO3 buffer. Figure S5, Comparison of sequential vs simultaneous agonist addition on CFTR detection by ICM. Figure S6, Comparison of four cold storage conditions on rectal biopsy performance. Figure S7, Comparison of CFTR-dependent ICM responses from forceps and suction biopsies in non-CF subjects.
(DOC)