

Abstract
Background and Purpose Sphenoid bone fractures and sphenoid sinus fractures have a high morbidity due to its association with high-energy trauma. The purpose of this study is to describe individuals with traumatic injuries from different mechanisms and attempt to determine if there is any relationship between various isolated or combined fractures of facial skeleton and sphenoid bone and sphenoid sinus fractures.
Methods We retrospectively studied hospital charts of all patients who reported to the trauma center at Hospital de San José with facial fractures from December 2009 to August 2011. All patients were evaluated by computed tomography scan and classified into low-, medium-, and high-energy trauma fractures, according to the classification described by Manson.
Design This is a retrospective descriptive study.
Results The study data were collected as part of retrospective analysis. A total of 250 patients reported to the trauma center of the study hospital with facial trauma. Thirty-eight patients were excluded. A total of 212 patients had facial fractures; 33 had a combination of sphenoid sinus and sphenoid bone fractures, and facial fractures were identified within this group (15.5%). Gender predilection was seen to favor males (77.3%) more than females (22.7%). The mean age of the patients was 37 years. Orbital fractures (78.8%) and maxillary fractures (57.5%) were found more commonly associated with sphenoid sinus and sphenoid bone fractures.
Conclusions High-energy trauma is more frequently associated with sphenoid fractures when compared with medium- and low-energy trauma. There is a correlation between facial fractures and sphenoid sinus and sphenoid bone fractures. A more exhaustive multicentric case-control study with a larger sample and additional parameters will be essential to reach definite conclusions regarding the spectrum of fractures of the sphenoid bone associated with facial fractures.
Keywords: craniofacial trauma, sphenoid sinus, fracture, sphenoid bone, facial trauma, CT
Craniomaxillofacial trauma has been reported to occur in 20 to 30% of all trauma patients.1,2 Maxillofacial injuries traditionally have been treated as a separate entity, but clinical research has tried to establish a correlation between them and concomitant skull base injuries. The closeness of these bones to the cranium would suggest that there are chances of cranial injuries also occurring simultaneously, and except for a few studies, there is a general dearth of data trying to establish a correlation between them.
A classification based on the mechanism of the trauma was described by Manson et al. In this classification the mechanism of the trauma was divided into low-, middle-, and high-energy injuries according to the computed tomography (CT) findings such as degree of comminution and displacement of the bone.3
In type I fractures, there is minimal displacement of the bones and no comminution. In type II fractures, there is moderate displacement of the bones and a small degree of comminution. And finally, in type III fractures, there is severe displacement, with the major buttresses comminuted in multiple locations. This classification helps to determine the prognosis of the patient.3
Sphenoid bone and sphenoid sinus fractures have a high morbidity due to the complexity of trauma and soft tissue involved at the level of the brain. Skull base fractures are of high importance in neurotrauma. They occur in 3.5 to 24% of head injuries and are often related to brain injury (in 50% of the cases).4
Radiologic diagnosis of skull base fractures is usually obtained by a high-resolution CT scan.
The aim of this study is to describe individuals with traumatic injuries from different mechanisms and attempt to determine if there is any relationship between various isolated or combined fractures of facial skeleton and fractures of the sphenoid bone.
Materials and Methods
We retrospectively studied hospital charts of all patients who reported to the trauma center in the Hospital de San Jose, Bogota, Colombia with facial fractures (December 1, 2009, to August 30, 2011). All patients were evaluated by a CT scan. The complete medical record of each patient was reviewed, and the patients were classified according to Manson's classification into low-, middle-, and high-energy trauma.
Five categories of patients with facial fractures were excluded including:
Patients who, due to serious general conditions after severe injuries, had inadequate clinical and radiographic investigation
Patients younger than 12 years old
Patients with craniomaxillofacial syndromes
Patients with solitary fractures of the alveolar process (inferior or superior) or pure dental injuries (subluxation, luxation, avulsion)
Patients with a history of orthognathic surgery
We reviewed CT scans performed with General Electric (General Electric, Fairfield, CT) equipment using four-channel multislice, with cuts at 0.5 to 1.0 mm. The patients were divided according to the classification described by Manson of craniomaxillofacial trauma into high-, medium-, or low-energy trauma (Table 1).
Table 1. Intensity of trauma and clinical characteristics according to Manson's classification.
| Intensity of trauma | Trauma features |
|---|---|
| Low energy | Incomplete or complete fractures without displacement or a minimum degree of displacement that generally do not require very large maneuvers for reduction and fixation |
| Medium energy | Fractures with a moderate degree of displacement, without further comminution and bone loss, requiring open reduction and fixation, following standard techniques with conventional exhibitions |
| High energy | High degree of fragmentation, displacement, and loss of bone tissue, with a disruption of geography that requires extensive exposure, careful reduction, use of bone grafts, and/or composite bone flaps for reconstruction of the pillars. |
The complete medical record of each patient was reviewed, recording the following in a standard format: age, gender, type of trauma, type of facial fractures, open or closed fractures, documented physical examination findings associated with eye injury, carotid sinus syndrome, cavernous syndrome, superior orbital fissure syndrome.
The database was created in Microsoft Excel 2007, and statistical analysis with Stata 10 (Stata Corp., College Station, TX) quantitative variables were summarized with measures of central tendency and the dispersion, and categorical variables are presented as proportions. The research protocol was approved by the Ethics Committee for Research and the Faculty of Medicine of the Fundación Universitaria de Ciencias de la Salud and was classified as an investigation without risk to the patient, so there was no need for informed consent.
Results
A total of 250 patients reported to the trauma center of the study hospital with facial trauma. Thirty-eight patients were excluded from the analysis (Fig. 1). A total of 212 patients had facial fractures; the ages of the patients ranged from 12 to 99 years, with a mean age of 37 years (standard deviation 18.5). Gender predilection was seen to favor males 77.3% (n = 164) more than females 22.7% (n = 48). Motor vehicle accidents were the most common cause of injury (49.5%), followed by falls from heights (21.7%) and street fights (20.8%; Table 2).
Figure 1.
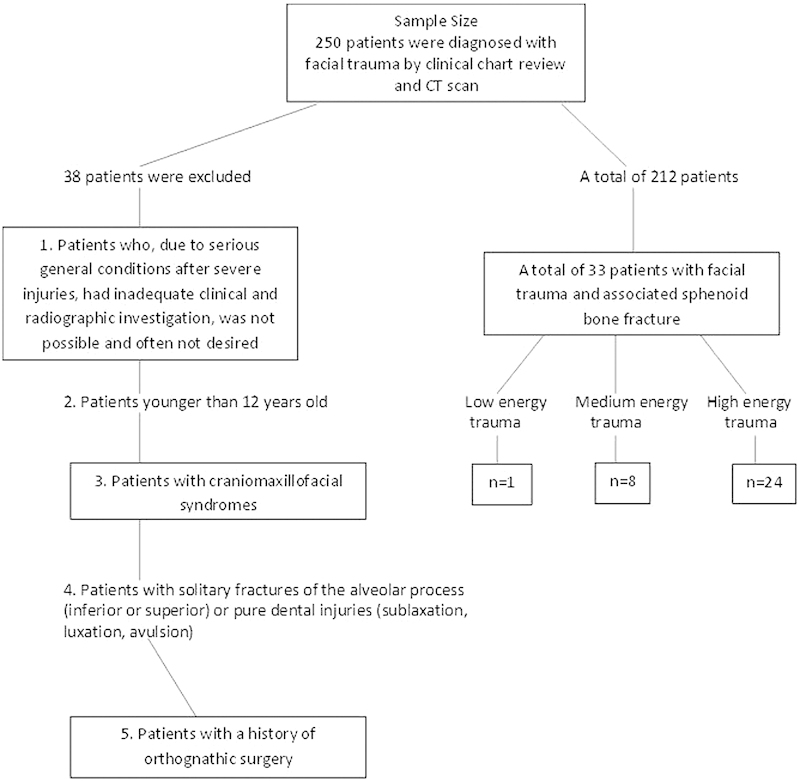
Distribution of the study population. Abbreviation: CT, computed tomography.
Table 2. Demographic characteristics of the population (n = 212) and etiology of the trauma.
| Age, y (SD) | 37 (18.5) |
| Minimum-maximum | 12 99 |
| Male, n (%) | 164 (77.3) |
| Female, n (%) | 48 (23.7) |
| Terms of trauma, n (%) | |
| Driver, car accident | 5 (2.3) |
| Occupant, car accident | 15 (7.0) |
| Pedestrian | 29 (13.6) |
| Motorcycle driver | 27 (12.5) |
| Total car accidents, n (%) | 105 (49.5) |
| Bike driver | 16 (7.5) |
| Street fight | 45 (20.8) |
| Self-inflicted/involuntary trauma | 23 (10.8) |
| Drop height | 46 (21.7) |
| No data | 6 (2.8) |
| Intensity of the trauma, n (%) | |
| High energy | 38 (17.9) |
| Medium energy | 71 (33.5) |
| Low energy | 103 (48.6) |
| Open fracture, n (%) | 17 (7.9) |
Abbreviation: SD, standard deviation.
The frequency of the sphenoid sinus and sphenoid bone fractures was 15.5% (n = 33); 82% of these fractures occurred in the male population. One patient had sphenoid bone fracture without involvement of the sphenoid sinus, which corresponded to 0.5%, and the presence of the sphenoid sinus fracture without involvement of the sphenoid bone was recorded in 8% (n = 17) of cases. Finally, 7.1% (n = 15) had combined fractures of the sphenoid bone and the sphenoid sinus.
According to Manson's classification, 17.9% (n = 38) of the trauma in the group corresponded to high-energy trauma, followed by medium-energy trauma at 33.5% (n = 71) and low-energy trauma at 48.6% (n = 103). Among the patients with high-energy trauma, 31.5% (n = 12) had combined fractures of the sphenoid bone and sphenoid sinus and 31.5% (n = 12) had sphenoid sinus fractures only. In contrast, 1.4% (n = 3) of patients with middle-energy trauma had sphenoid bone fractures, 5.6% (n = 4) of the patients had sphenoid sinus fractures, and 4.2% (n = 3) of the patients had sphenoid bone and sphenoid sinus fractures. In the low-energy trauma group, only 1 patient presented sphenoid sinus fracture (0.97%; Table 3; Figs. 2, 3, 4).
Table 3. Frequency of fracture of the sphenoid sinus and sphenoid bone.
| Sphenoid bone fracture | 1 (0.5) |
| Sphenoid sinus fracture | 17 (8.0) |
| Sphenoid bone and sphenoid sinus fracture | 15 (7.1) |
Note: Results are n (%).
Figure 2.
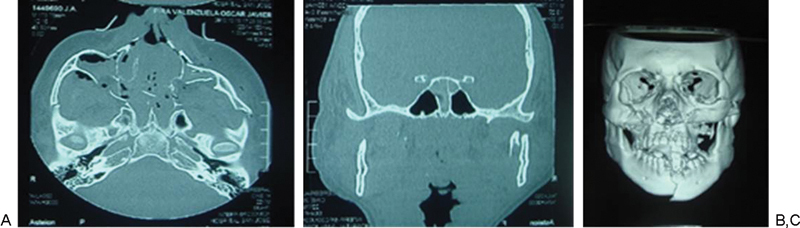
Patient 1: high-energy trauma and panfacial fractures. (A) Zygomatic arch, malar, and upper jaw fractures. (B) Sphenoid sinus fracture. (C) Computed tomography three-dimensional reconstruction showing the fractures at the middle third and jaw.
Figure 3.
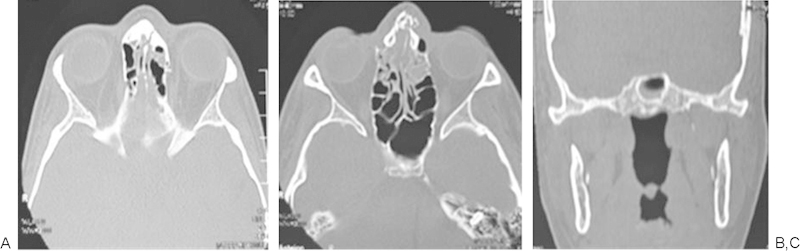
Patient 2: high-energy comminuted fracture of nasal bone (A and B), associated fracture of the sphenoid sinus.
Figure 4.
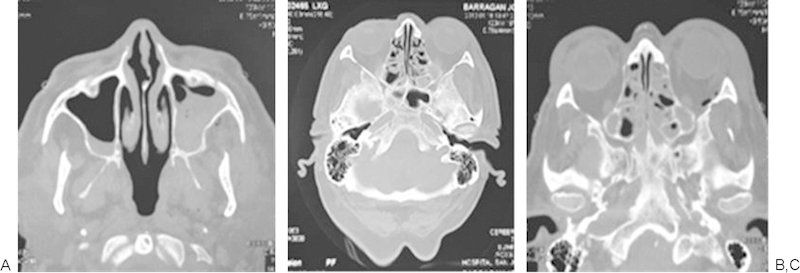
Patient 3: slightly displaced malar fracture in a patient with medium energy trauma, (A) presence of fracture at the level of the zygomatic arch, (B and C) fracture at the lateral wall of the sphenoid bone and orbital fracture associated.
The general description of facial fractures is presented in Table 4. Orbit fractures (52.3%; n = 111) and nasal fractures (43.9%; n = 93) were the most frequent facial bone fractures associated with sphenoid bone and sphenoid sinus fractures, followed by fractures of the mandible (32.1%; n = 68). Panfacial fractures occurred in 7.5% (n = 16) of cases, and skull base fractures were presented in 2.8% (n = 6) of the patients.
Table 4. Sphenoid bone and sphenoid sinus fracture frequency depending on the intensity of the trauma (Manson's classification).
| High energy (n = 38) | Medium energy (n = 71) | Low energy (n = 103) | |
|---|---|---|---|
| Sphenoid bone fracture | - | 1 (1.4) | - |
| Sphenoid sinus fracture | 12 (31.5) | 4 (5.6) | 1 (0.9) |
| Sphenoid bone and sphenoid sinus fracture | 12 (31.5) | 3 (4.2) | - |
Note: Results are n (%).
The relationship of the sphenoid bone fractures and other fractures of the craniomaxillofacial complex was found in 33 patients who presented sphenoid bone and sphenoid sinus fractures (78.8%; n = 33). From this group, 57.6% (n = 19) of the patients had orbital and mandibular fracture (Table 5).
Table 5. Description of craniofacial fractures (n = 212).
| Nasal | 93 (43.9) |
| Orbit | 111 (52.3) |
| Malar | 23 (10.5) |
| Zygomatic arch | 29 (13.7) |
| Frontal | 34 (16.0) |
| Maxilla | 68 (32.1) |
| Mandibular | 29 (13.7) |
| Sphenoid | 16 (7.5) |
| Sphenoid sinus | 32 (15.1) |
| Panfacial fracture | 16 (7.5) |
| Basilar skull fracture | 6 (2.8) |
Note: Results are n (%). A patient may have more than one fracture.
We also found that skull base fractures were present in 18.1% (n = 6) of the patients (Table 6). In the population studied, 1 patient had amaurosis caused by direct eye injury, there were no cases of superior orbital fissure syndrome or orbital apex syndrome, 2 patients had otorrhagia, and 1 of these patients had basilar skull fracture. Two patients with basilar skull fracture presented a relevant clinical sign: cerebrospinal fluid rhinorrhea. None of the patients presented carotid sinus syndrome or cavernous sinus syndrome.
Table 6. Fractures most frequently associated with sphenoid sinus fractures and/or sphenoid bone fractures (n = 33).
| Nasal | 13 (39.4) |
| Orbit | 26 (78.8) |
| Malar | 9 (27.2) |
| Zygomatic arch | 8 (24.2) |
| Frontal | 12 (36.3) |
| Maxilla | 19 (57.5) |
| Mandibular | 2 (6.0) |
| Panfacial fracture | 9 (27.2) |
| Skull base | 6 (18.1) |
Note: Results are n (%).
Discussion
Several studies describing a large series of facial fractures have been reported.5,6 There is, however, a general lack of literature specifically with regard to maxillofacial trauma pertaining to associated injuries in general and fracture of the sphenoid bone and sphenoid sinus in particular.7,8,9
The literature shows associated skull fractures in varied ranges, with several studies reporting 19% associated skull fractures. In all of these studies, however, skull fractures were addressed generally. Unger et al found a higher frequency of sphenoid bone fractures in patients with craniofacial fractures (70%) than in patients with complex facial fractures.10
Lee et al reported that facial fractures are associated with a decreased risk of traumatic brain injury.11 They theorized that the facial bones act as a protective cushion for the brain to explain why injuries that crush the facial bones frequently cause no apparent brain damage. Davidoff et al, however, found facial fractures to be highly associated with traumatic brain injury.12 Chang et al stated that in central craniofacial fractures, the maxilla is not only important for functional, physiologic, and esthetic reasons, but with other bones of the central area, it forms a structure capable of absorbing considerable impact energy, thus protecting the brain from direct collision.13 They concluded that there should be a direct correlation between the severity of maxillary fracture (in the central craniofacial) and that of the initial head injury.
The literature shows a few descriptions of the relationship between sphenoid sinus and sphenoid bone fractures and high-, medium-, or low-energy facial trauma. In our study the association between sphenoid bone and sphenoid sinus fractures with high-energy trauma was important, whereas in the medium-energy trauma group, we found only two patients with associated sphenoid bone and sphenoid sinus fractures. In the low-energy trauma group, only one patient had sphenoid bone and sphenoid sinus fracture due to the transmission of the vibratory forces through the craniomaxillofacial skeleton.14,15,16
The orbital fractures were the most frequently associated with sphenoid bone and sphenoid sinus fractures, followed by midface fractures due to transmission of forces through the pterygoid process to structures of the orbit, especially the lateral wall and roof.16
There is an important relationship between the high-energy trauma and the increased frequency of sphenoid bone and sphenoid sinus fractures.
In our study half of the patients presented low-energy trauma and the other half presented medium- and high-energy trauma.
In our study we identified four major fracture patterns of transsphenoidal basilar skull fractures, which were: anterior transverse (AT), lateral frontal diagonal (LFD), posterior transverse (PT), and mastoid diagonal (MD), which matches Clark's descriptions of the transsphenoidal basilar skull fractures.17
AT Pattern
The key to the identification of the AT pattern is the demonstration of a coronal fracture through the sphenoidal plane at the base of the anterior clinoid processes. The exact position across the anterior sphenoid body varies slightly from the sphenoidal limbus to the roof of the extreme posterior ethmoid air cells. Most fractures pass through the roof of the sphenoid sinus anteriorly. The fracture typically begins in the squamous portion of the temporal bone, courses anteriorly to the sphenotemporal buttress, and then proceeds medially along the orbital surface (vertical plate) or the anterior cerebral surface (horizontal plate) of the sphenoid bone. The fracture intersects the sphenoid body at or slightly posterior to the junction, with the ethmoid bone producing the characteristic transverse fracture across the posterior aspect of the floor of the anterior cranial fossa. The fracture exits the sphenoid body through a similar pathway involving the contralateral greater wing along the orbital surface (horizontal plate) or the anterior cerebral surface (vertical plate). In severe fractures, the fracture will continue to propagate into the contralateral squamous portion of the temporal bone (Fig. 5).
Figure 5.
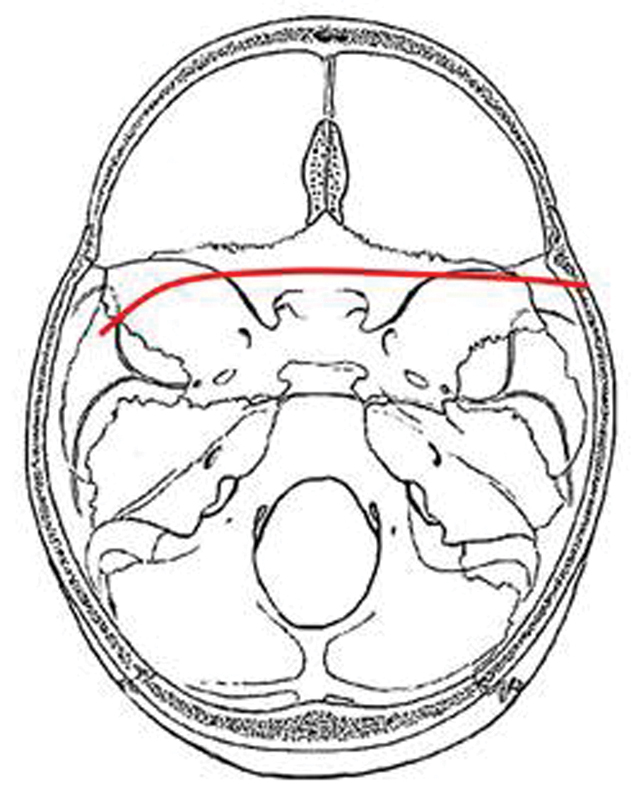
Composite drawing of the anterior transverse fracture pattern (left impact).
LFD Pattern
The LFD fracture pattern occurs as the result of impact to the lateral frontal region or the anterior malar eminence. Force appears to be transmitted along the lateral orbital and/or lateral maxillary sinus wall to the sphenotemporal buttress. From the sphenotemporal buttress, the force is transmitted along the ipsilateral sphenoid sinus wall to the posterior wall of the sphenoid sinus. The fracture may cross the sphenoid body in a transverse plane or in a diagonally plane. The fracture continues through or immediately anterior to the contralateral carotid canal into the sphenopetrosal synchondrosis. The fracture may then continue through the tympanic portion of the temporal bone (Fig. 6).
Figure 6.
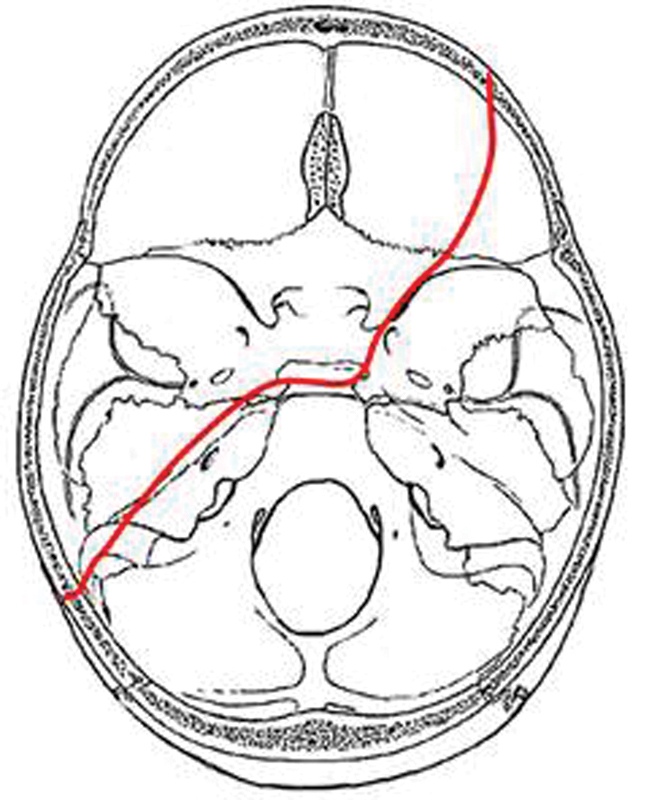
Composite drawing of the lateral frontal diagonal pattern (left impact).
PT Pattern
PT fractures usually have a characteristic inverted u shape, with fractures extending from one temporal bone, across the middle cranial fossa to the posterior sphenoid body and clivus, then to opposite middle cranial fossa, and then on to the opposite temporal bone. The hallmark of this fracture pattern is the demonstration of a transverse fracture through the posterior sphenoid sinus or clivus. The exact location of this fracture occurs most frequently at the posterior wall of the sphenoid sinus but sometimes a few millimeters anterior or posterior to this location. The fracture usually results from lateral impact to the skull and enters the skull base in the tympanic portion of the temporal bone anterior to the external auditory canal and inferoposterior to the mandibular fossa of the temporal bone (Fig. 7).
Figure 7.
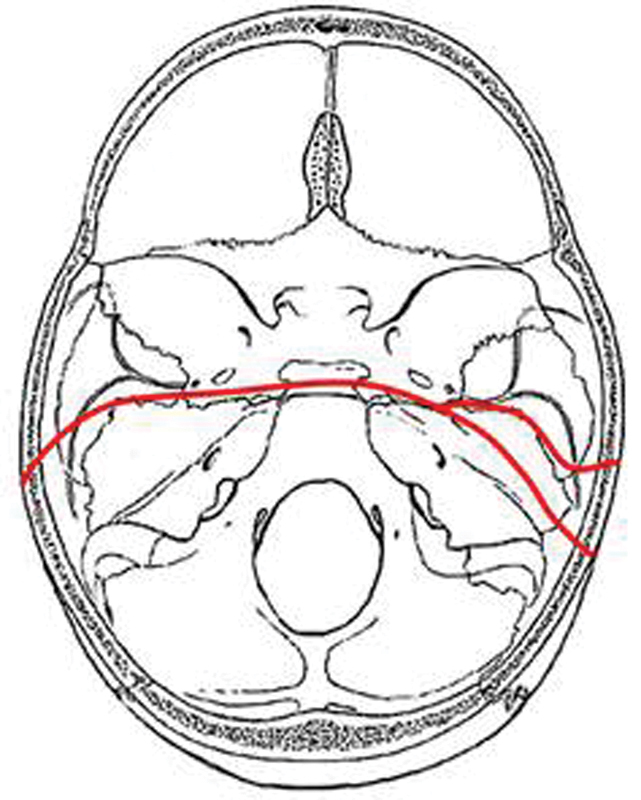
Composite drawing of the posterior transverse pattern (left impact).
MD Pattern
These fractures occur in patients with mastoid impact and who had diagonal fractures extending from the ipsilateral occipital bone at the occipitomastoid suture across the jugular foramen to the petro-occipital fissure and into the sphenoid body. The fractures cross the sphenoid sinus diagonally and exit it anteriorly across the sphenoidal plane. There are ipsilateral temporal bone fractures with associated diastasis of the ipsilateral sphenopetrosal sincondrosis. The MD fracture crosses the sphenoid body diagonally from posterior to anterior. Also the MD fracture terminates in the contralateral anterior cranial fossa (Fig. 8).
Figure 8.
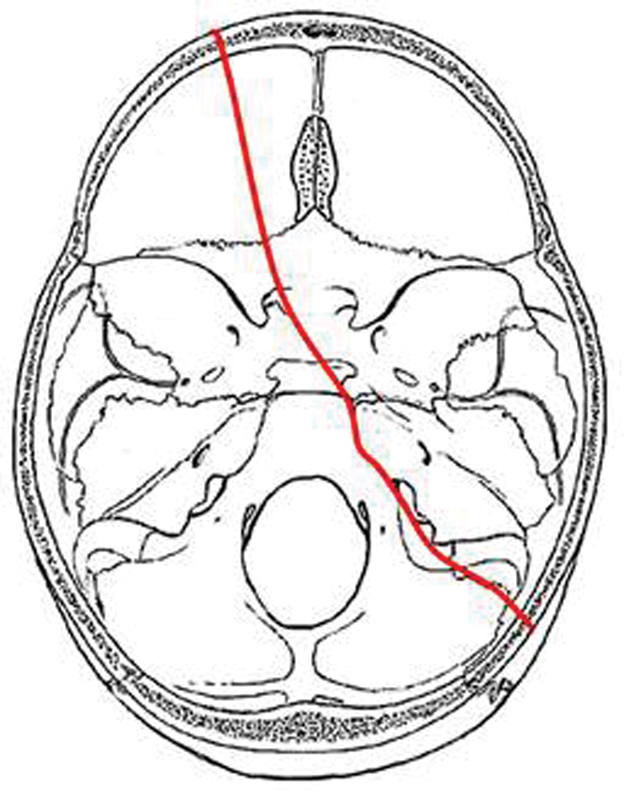
Composite drawing of the mastoid diagonal pattern (left impact).
These results indicate that transsphenoidal basilar skull fractures occur along reproducible lines of weakness, including a coronal plane through the anterior sphenoid body and clivus and the sphenopetrosal sincondrosis. The location of these fractures is not surprising, because the anterior and posterior walls of the sphenoid sinus are points of transition. Anteriorly, this transition is from the well-reinforced ethmoid air cells to the relatively unsupported lateral walls of the sphenoid sinus. Posteriorly, the transition is from the solid cancellous bone of the clivus to the thin plates of cortical bone that compose the lateral walls of the sphenoid sinus.
According to a study, of 290 patients with frontobasal fractures, 86 had naso-orbitoethmoid fractures (41%).18 In their study, the naso-orbitoethmoid fractures were associated more frequently with frontobasal fractures. The concomitant midfacial fractures (naso-orbitoethmoid and Le Fort II/III) represented a higher-energy injury, leading to increased complications. They established that nasoethmoidal fractures are frequently accompanied by anterior base fractures in the region of the cribriform plate and are more likely to produce a complication than a Le Fort II/III fracture. They also found that facial bones absorb sufficient energy such that cranial structures are protected.
In another article, the authors proposed that force transmission resulting in bilateral zygomatic arch fractures results from movement of the petrous portion of the temporal bone.19 They described a triangle, which consists of the lateral skull portion as its base, the petrosphenoid junction as the anterior arm, and the petro-occipital junction as the posterior arm, with the apex consisting of a junction with the body of the sphenoid. The forces applied during a trauma exert a rotational or a translational movement causing compression and distraction fractures. If the zygomatic arch is fractured, it may prevent force transmission into the midface or periorbital bones. This important concept reinforces why isolated bilateral zygomatic arch fractures can occur with no other facial bone fractures. In our study 24.2% patients presented zygomatic arch fracture in combination with sphenoid sinus and sphenoid bone fractures. In their study a total of five patients presented true bilateral zygomatic arch fractures with complete absence of Le Fort fracture patterns or any other facial fractures but were associated with severe concomitant injuries. Therefore, the authors recommend raising strong suspicion for the presence of basilar skull fractures, intracranial hemorrhage, and neurologic injury in patients with bilateral zygomatic arch fractures.
Conclusions
High-energy trauma is more frequently associated with sphenoid fractures when compared with medium- and low-energy trauma. There is a correlation between facial fractures and sphenoid sinus and sphenoid bone fractures.
A more exhaustive multicentric case-control study with larger sample and additional parameters will be essential to reach definite conclusions regarding the spectrum of sphenoid bone and sphenoid sinus fractures associated with facial fractures.
References
- 1.Cantini J. 2008. Principios basicos en el manejo de las fracturas del esqueleto facial. [Google Scholar]
- 2.Cantini J. Manejo de las fracturas del tercio medio facial, de la region frontal y de las Fracturas panfaciales. Cirugia Craneofacial. 2011;1(1):341–415. [Google Scholar]
- 3.Manson P N Markowitz B Mirvis S Dunham M Yaremchuk M Toward CT-based facial fracture treatment Plast Reconstr Surg 199085202–212., discussion 213-214 [PubMed] [Google Scholar]
- 4.Hayter J P, Ward A J, Smith E J. Maxillofacial trauma in severely injured patients. Br J Oral Maxillofac Surg. 1991;29:370–373. doi: 10.1016/0266-4356(91)90003-n. [DOI] [PubMed] [Google Scholar]
- 5.Rowe N L, Killey H C. Edinburgh, London: Livingstone; 1968. Fractures of the Facial Skeleton; p. 857. [Google Scholar]
- 6.Murray J F, Hall H C. Fractures of the mandible in motor vehicle accidents. Clin Plast Surg. 1975;2:131–142. [PubMed] [Google Scholar]
- 7.Haug R H, Prather J, Indresano A T. An epidemiologic survey of facial fractures and concomitant injuries. J Oral Maxillofac Surg. 1990;48:926–932. doi: 10.1016/0278-2391(90)90004-l. [DOI] [PubMed] [Google Scholar]
- 8.Haug R H, Savage J D, Likavec M J, Conforti P J. A review of 100 closed head injuries associated with facial fractures. J Oral Maxillofac Surg. 1992;50:218–222. doi: 10.1016/0278-2391(92)90315-q. [DOI] [PubMed] [Google Scholar]
- 9.Haug R H, Adams J M, Conforti P J, Likavec M J. Cranial fractures associated with facial fractures: a review of mechanism, type, and severity of injury. J Oral Maxillofac Surg. 1994;52:729–733. doi: 10.1016/0278-2391(94)90488-x. [DOI] [PubMed] [Google Scholar]
- 10.Unger J M, Gentry L R, Grossman J E. Sphenoid fractures: prevalence, sites, and significance. Radiology. 1990;175:175–180. doi: 10.1148/radiology.175.1.2315477. [DOI] [PubMed] [Google Scholar]
- 11.Lee K F, Wagner L K, Lee Y E. et al. The impact absorbing effects of facial fractures in closed head injury. J Neurosurg. 1987;66:542. doi: 10.3171/jns.1987.66.4.0542. [DOI] [PubMed] [Google Scholar]
- 12.Davidoff G, Jakubowski M, Thomas D, Alpert M. The spectrum of closed-head injuries in facial trauma victims: incidence and impact. Ann Emerg Med. 1988;17:6–9. doi: 10.1016/s0196-0644(88)80492-x. [DOI] [PubMed] [Google Scholar]
- 13.Chang C J, Chen Y R, Noordhoff M S, Chang C N. Maxillary involvement in central craniofacial fractures with associated head injuries. J Trauma. 1994;37:807–811. doi: 10.1097/00005373-199411000-00017. [DOI] [PubMed] [Google Scholar]
- 14.Galán R. Balística y manejo integral de la mano severamente traumatizada por arma de fuego. Rev Colomb Cir Plast Reconstruc. 1999;5:86–91. [Google Scholar]
- 15.Kretschmer H. Stuttgart, Germany: Thieme; 1978. Neurotraumatologie. [Google Scholar]
- 16.Franz-J K. Intra- and perioperative complications of the Lefort I osteotomy: a prospective evaluation of 1000 patients. J Craniofac Surg. 2004;31:971–977. doi: 10.1097/00001665-200411000-00016. [DOI] [PubMed] [Google Scholar]
- 17.West O C, Mirvis S E, Shanmuganathan K. et al. Transsphenoid basilar skull fractures: CT patterns. Radiology. 1993;188:329–338. doi: 10.1148/radiology.188.2.8327674. [DOI] [PubMed] [Google Scholar]
- 18.Manson P N, Stanwix M G, Yaremchuk M J, Nam A J, Hui-Chou H, Rodriguez E D. Frontobasal fractures: anatomical classification and clinical significance. Plast Reconstr Surg. 2009;124:2096–2106. doi: 10.1097/PRS.0b013e3181bf8394. [DOI] [PubMed] [Google Scholar]
- 19.Kelamis J A, Mundinger G S, Feiner J M, Dorafshar A H, Manson P N, Rodriguez E D. Isolated bilateral zygomatic arch fractures of the facial skeleton are associated with skull base fractures. Plast Reconstr Surg. 2011;128:962–970. doi: 10.1097/PRS.0b013e3182268cf3. [DOI] [PubMed] [Google Scholar]