

Otosclerosis is a disorder of the bony labyrinth characterized by an active metaplastic process within the endochondrial layer of the temporal bone, which normally undergoes very little bone remodeling after development. This bone remodeling is a highly regulated process that involves a simultaneous and continuing perivascular bone resorption (otospongiosis) and a deposition of immature and collagen-deficient bone (otosclerosis) (1). In the Caucasian population, the incidence of clinical otosclerosis is approximately 0.1%, but the histologic otosclerosis can reach 12%.
To our knowledge, there are only a few references to cavity formation in otosclerotic foci, one described by Schucknecht (1) and one in a pericochlear cavity case report describing a pathologic “third window” (2).
Pathologic third-window lesions may be anatomically discrete and, thus, classified by location (semicircular canals, bony vestibule or cochlea) or diffuse like in Paget disease. Clinically, these lesions are unique in that they have differing effects on air versus bone conduction and also may result in vestibular manifestations by making the vestibular sense organ sensitive to sound or mechanical stimulation (3).
This is the first case of a third window effect because of a cavity in an otosclerotic focus in contact with the superior semicircular canal.
CASE REPORT
A 68-year-old man with a 50-year history of tinnitus and progressive bilateral hearing impairment thought to be caused by otosclerosis underwent right stapedectomy surgery (1960), followed by left stapedectomy 2 years later. After some improvement on the right side, he complained of hearing fluctuation and increasing tinnitus on both sides and could not wear his left hearing aid because of a Tulio effect. Audiometric tests revealed an air-bone gap on both sides, leading to a revision stapes surgery on the right and then on the left in 1990 and 1992, respectively. The hearing results were good, but the patient still had dizziness. Subsequently the patient had 2 sudden hearing loss events affecting both ears, resistant to parenteral treatment. The patient underwent cochlear implantation on the left side in 1992, with good results.
HISTOPATHOLOGY
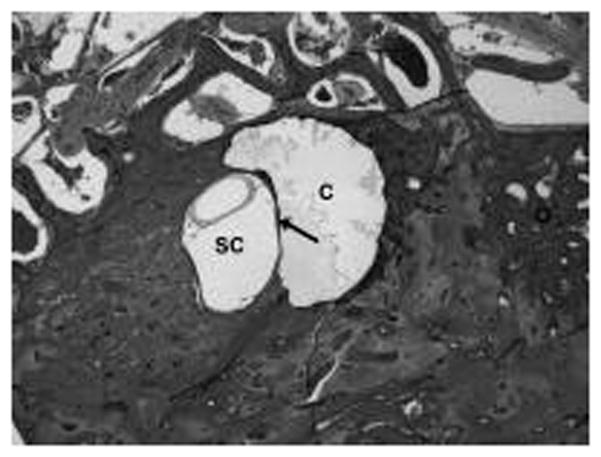
The left temporal bone shows a very severe advanced otosclerosis with areas of sclerosis and spongiosis and with cavities of various sizes (Fig. 1). One cavity (C) is in contact with the endosteum of the superior semicircular canal (SC), from its middle part to its ampula, and consequently creates a “third window” (Fig. 2).
Fig. 1.
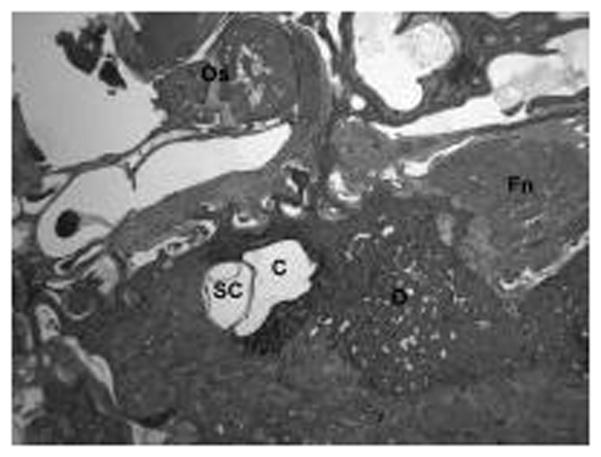
Fig. 2.
Acknowledgments
This study was supported by the following: 1) National Institutes of Health grant number: U 24 DC 011962 HO 1; and 2) Grant Perspectives ORL 2010, Sanofi-Aventis.
Footnotes
The authors disclose no conflicts of interest.
References
- 1.Schuknecht HF. Pathology of the ear. Vol. 2. New York, NY: Lea and Febiger; 1993. [Google Scholar]
- 2.Makarem A, Linthicum FH. Cavitating otosclerosis. Otol Neurotol. 2008;29:730–1. doi: 10.1097/MAO.0b013e3181799763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Merchant SN, Rosowski JJ. Conductive hearing loss caused by third-window lesions of the inner ear. Otol Neurotol. 2008;29:282–9. doi: 10.1097/mao.0b013e318161ab24. [DOI] [PMC free article] [PubMed] [Google Scholar]