

Abstract
Background Retrosigmoid transtentorial (RTT) and retrosigmoid intradural suprameatal (RISA) approaches have been used in the treatment of petroclival tumors.
Objective To compare the area of exposure of brainstem and petroclival region obtained through RTT and RISA in cadaveric specimens.
Methods Five cadaveric specimens with a total of 10 sides were analyzed. RTT and RISA were performed on five sides each. Brainstem and petroclival surface exposure were measured using both the approaches. These values were compared between the two approaches.
Results Brainstem area exposure with RTT was 441 ± 63 mm2 and that with RISA was 311 ± 61 mm2. Student's t-test revealed that the difference was significant (p = 0.01). The area of petroclival exposure medial to the Meckel cave through RTT was 696 ± 57 mm2, and that through RISA was 716 ± 51 mm2 (p = 0.69). The area of brainstem exposure between V and VII-VII complex through RTT and RISA was 387 ± 86 mm2 and 378 ± 76 mm2 (p = 0.87).
Conclusion The RTT approach is an excellent approach to ventrolateral brainstem and petroclival region. It provides greater superoventral exposure of the ventrolateral brainstem than RISA and provides similar petroclival exposure.
Keywords: petroclival meningioma, retrosigmoid, suprameatal, transtentorial
Introduction
Tumors located in the petroclival region pose a challenge to the neurosurgeon due to their multicompartmental extension, relatively large size at presentation, and their proximity to the brainstem. As many tumors in this region are benign, complete excision can potentially cure the patients. Consequently, several surgical approaches have been devised to approach these difficult-to-treat lesions. Due to their extension into the middle and the posterior cranial fossa, two-staged operations have been described to excise the middle fossa and posterior fossa components separately.1,2 The various approaches to the petroclival region include the retrosigmoid approach, retrosigmoid intradural suprameatal approach (RISA), middle fossa (Kawase) approach, and the modifications of transpetrosal approach.1,3,4,5,6,7,8,9,10 Given the benign nature of these tumors, the principles of neuro-oncology dictate complete resection of these tumors. The morbidity related to excision of tumors using these approaches has given rise to the concept of maximal safe resection with or without adjuvant radiosurgery.11,12,13 Hence, there is a need to maximize the exposure obtained during surgery while trying to reduce the morbidity related to the approach itself.
The RISA is a modification of the retrosigmoid approach to the cerebellopontine angle. The RISA was devised to access the tumors extending into the middle cranial fossa through the Meckel cave so as to be able to resect the entire tumor with one approach.14 The lateral supracerebellar transtentorial approach has been described earlier in patients with petroclival meningioma.15 In our study, we describe the retrosigmoid transtentorial approach (RTT) and compare the exposure of the brainstem and the petroclival area with that obtained by RISA in cadaveric models.
Materials and Methods
Five fixed and silicone-injected cadaveric heads without any known brain pathology were used to perform 10 approaches: 5 RISA and 5 RTT. The retrosigmoid intradural suprameatal approach was performed according to the technique described earlier.3,14,16 Cerebellar retraction was maintained equally in both the approaches to 1.5 cm.
Microsurgical Technique
Retrosigmoid Transtentorial Approach
The cadaver head was fixed with a Mayfield clamp with rotation of the head to the opposite side, anterior flexion, and lateral flexion so as to orient the long axis of the petrous bone along the operative visual axis. The lateral flexion helps to open up the occipitoatlantal space so as to be able to extend the bone removal up to the foramen magnum, when required. A linear incision was marked 2 cm behind the mastoid extending from just above the level of transverse sinus below. The skin was incised and underlying muscular layers were divided sequentially up to the bone. A bur hole was made just below the asterion and a 3 × 3 cm craniotomy was completed using a high-speed drill. The dura was incised and cut based on the transverse and sigmoid sinuses. For the purpose of our study, the entire dura in the operative field was excised. Greenberg retractor was fixed and the cerebellum was retracted to visualize the cerebellopontine angle. The arachnoid covering the cerebellomedullary cistern was dissected. The retractor over the cerebellum was placed over the superior half of the surface facing the petrous bone. The superior petrosal vein was identified and cut. Then, the VII-VIII cranial nerve complex was identified and the V cranial nerve was identified exiting from the pons and entering the Meckel cave. The trochlear nerve traversing under the tentorium was identified. The tentorium cerebelli was incised using a No.11 blade and the brainstem and petroclival surface measurements were made (Fig. 1).
Fig. 1.
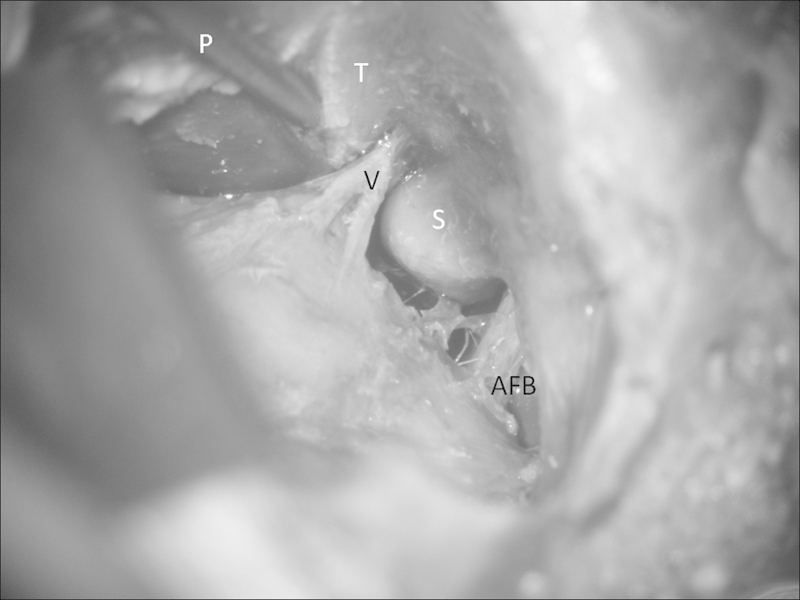
In the retrosigmoid transtentorial approach, the tentorium (T) is incised all along its length and a probe (P) is inserted between its incised margins. Other structures seen in the region of the cerebellopontine angle are the trigeminal nerve (V), acousticofacial bundle (AFB) and the suprameatal tubercle (S).
Retrosigmoid Intradural Suprameatal Approach
The cadaver head was positioned as for the RTT and a suboccipital retrosigmoid craniotomy was performed as described earlier. The dura was opened and the arachnoid over the cerebellomedullary cistern was dissected. The cerebellum was retracted using a Greenberg retractor. The suprameatal tubercle was identified. The tubercle is bounded posteriorly and inferiorly by the internal auditory canal and the VII-VIII cranial nerve complex and superiorly by the tentorium and the V cranial nerve. Laterally, the drilling was performed up to the posterior and superior semicircular canals. This facilitated opening of the Meckel cave and mobilization of the trigeminal nerve. Measurements of brainstem and petroclival exposures were performed (Fig. 2).
Fig. 2.
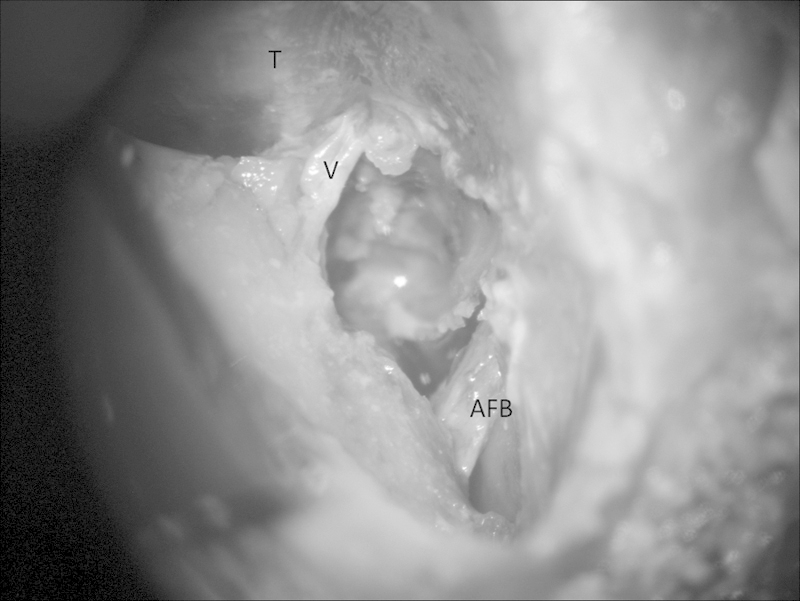
In the retrosigmoid intradural suprameatal approach, the suprameatal tubercle has been drilled to free the trigeminal nerve (V) as it enters the Meckel cave. AFB, acousticofacial bundle; T, tentorium.
Measurement of Area of Exposure
The area of exposure of brainstem was defined by the quadrangle of area anterior to a straight line joining the origins of the V cranial nerve and the VII-VIII cranial nerve complex from the brainstem. The maximum superoventral point of exposure above the origin of the V cranial nerve and the maximum inferoventral point of exposure through the gap between the origin of the V and VII-VIII cranial nerves was noted. The measurements for clival area of exposure were measured by noting the maximum superoventral and inferoventral point medial to the Meckel cave.
Statistical Analysis
All the measurements were analyzed using the SPSS software (v 21 IBM Inc., Armonk, New York, USA) and the areas of brainstem exposure and petroclival exposure through both the approaches were compared. Student's t-tests were done to compare the areas of exposure and a p value of less than 0.05 was considered significant.
Results
Brainstem Exposure
The mean area of exposure of the ventrolateral brainstem through RTT was 441 ± 63.3 mm2 and that through RISA was 311 ± 61 mm2. Student's t-test revealed that the area of brainstem exposure through RTT was significantly more than that through RISA (p = 0.01). The mean areas of ventrolateral brainstem exposure when measurements were made through the gap between the origin of the trigeminal nerve and the origin of the VII cranial nerve were not different through both the approaches (387 ± 86.9 mm2 in case of RTT and 378 ± 76.9 mm2 through RISA). The difference was not significant (p = 0.87). The RTT approach provided a more superoventral area of exposure when compared with the RISA. This resulted in increased maximal brainstem area of exposure through RTT when compared with that through RISA. The origin of the posterior inferior cerebellar artery was seen in both the approaches (Figs. 3, 4).
Fig. 3.
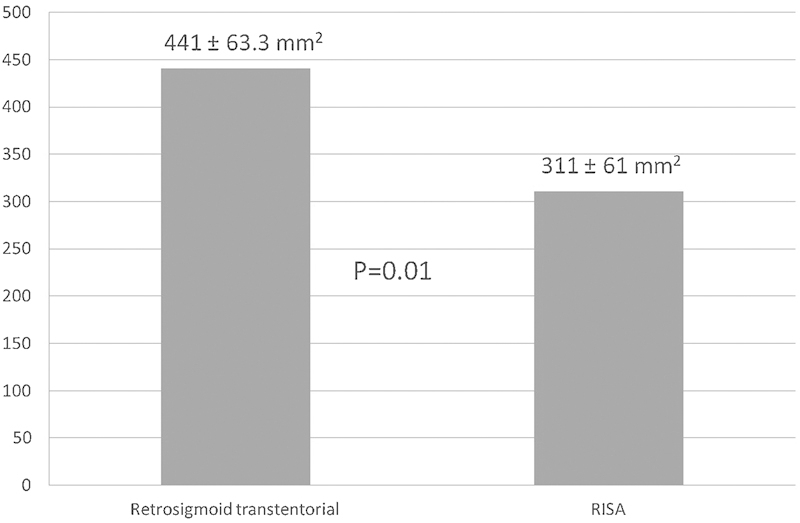
The mean area of brainstem surface exposed following the retrosigmoid transtentorial approach was 441 ± 63.3 mm2 and that following the retrosigmoid intradural suprameatal approach was 311 ± 61 mm2. The difference was significant (p = 0.01). RISA, retrosigmoid intradural suprameatal approach.
Fig. 4.
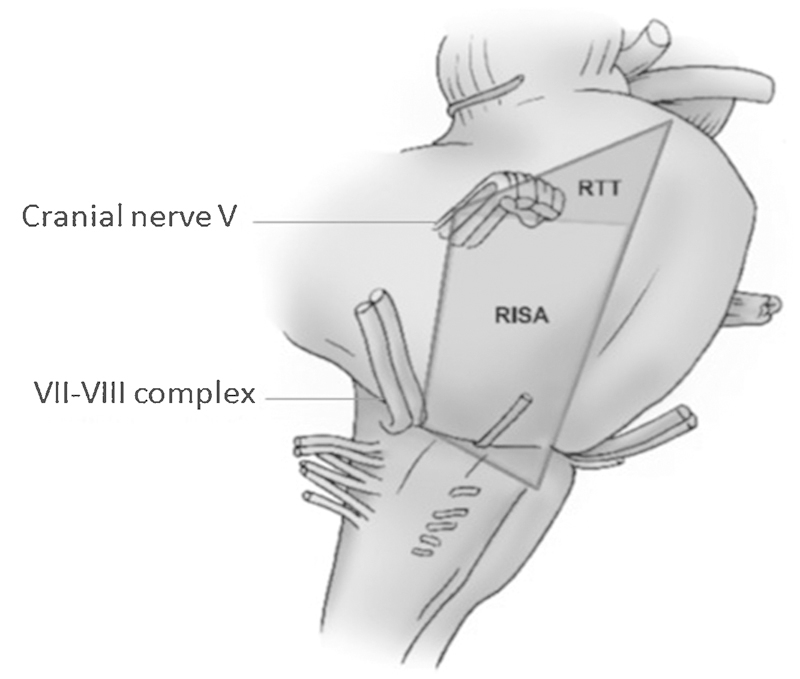
Schematic representation of the brainstem surface exposed using the retrosigmoid transtentorial (RTT) approach and the retrosigmoid intradural suprameatal approach (RISA).
Petroclival Exposure
Both the approaches provided exposure to the petroclival region medial to the Meckel cave. The maximum petroclival area of exposure through the retrosigmoid transtentorial approach was 696 ± 57.7 mm2, and that through the retrosigmoid intradural suprameatal approach was 716.7 ± 51.4 mm2. Student's t-test did not reveal any difference between the petroclival area of exposure obtained by the two approaches (p = 0.57). The degree of surgical freedom at the Meckel cave was more with the RISA than with RTT as is expected, although formal measurements were not made (Figs. 5, 6).
Fig. 5.
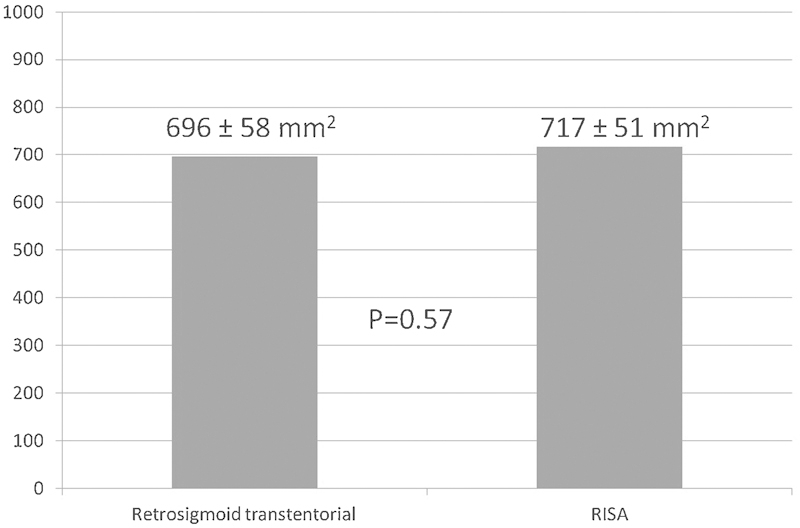
The mean petroclival surface area exposed using the retrosigmoid transtentorial approach and the retrosigmoid intradural suprameatal approach (RISA) was 696 ± 57.7 mm2 and 716.7 ± 51.4 mm2 respectively. The difference was not significant (p = 0.57).
Fig. 6.
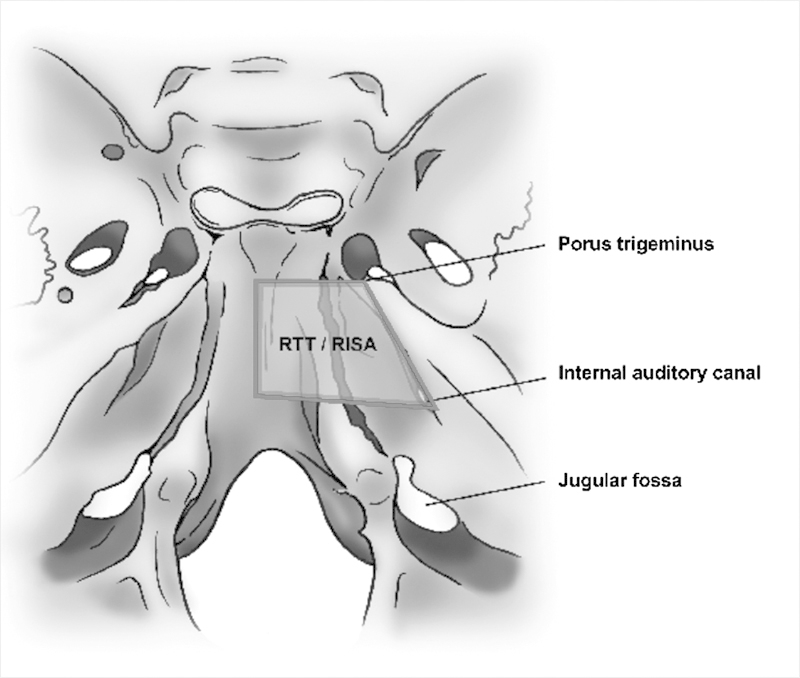
Schematic representation of the petroclival surface area exposed using the retrosigmoid transtentorial approach (RTT) and the retrosigmoid intradural suprameatal approach (RISA).
Discussion
Petroclival meningiomas constitute approximately 2% of all intracranial meningiomas and are one of the most difficult tumors to treat in neurosurgery. Management of these tumors has ranged from no treatment at all to gross total resection to subtotal resection combined with radiosurgery and radiosurgery alone.17,18,19,20 The large size of these tumors and their multicompartmental nature, adherence to the brainstem, compression of the brainstem, encasement of major arteries and perforator arteries, encasement of cranial nerves and hyperostosis, or erosion of the petrous bone makes surgery for these tumors difficult. The high morbidity and mortality associated with resection of these tumors has led to the concept of maximal safe resection with or without adjuvant radiosurgery.12,21 Selection of the surgical approach for these tumors should take into consideration the size of the tumor, its extension into the posterior fossa and middle fossa, and the extent of brainstem compression.
The lateral supracerebellar transtentorial approach for petroclival meningiomas was described by Kawamata and Katayama in 2006.15 They subsequently described this approach in 26 patients with petroclival meningioma with a gross total resection rate of 42% and postoperative permanent morbidity in 15% patients.22 The RTT approach is a slight modification of the lateral supracerebellar transtentorial approach and provides exposure to the ventrolateral brainstem and petroclival area while minimizing the complications associated with additional bone drilling. Incising the tentorium allows additional exposure of the superior portion of ventrolateral brainstem when compared with that obtained by the RISA. The major advantage of this approach is avoidance of extensive bone drilling of the suprameatal area. In addition, if suprameatal tubercle drilling is required, incising the tentorium provides additional space to the surgeon. Two structures should be taken care of before incising the tentorium. The superior petrosal vein should be identified and either mobilized or coagulated and cut to avoid inadvertent injury and bleeding. The fourth nerve should be identified and, if required, mobilized away to prevent injury while incising the tentorium.
The RISA provides additional exposure and mobilization of the trigeminal nerve and visualization of the structured medial to internal auditory canal, petrous apex, Meckel cave, and the posterior end of the cavernous sinus.3,10,14 In our previous study, we observed that although suprameatal drilling facilitated the view of structures medial to the internal auditory canal, the depth of exposure, and the visualization of the clivus did not differ from that obtained by the retrosigmoid approach.3
In the present study, we observed a greater exposure of the ventrolateral brainstem using the RTT. Exposure of the petroclival area did not differ significantly between the two approaches. In our opinion, the RTT approach should be used initially before drilling the suprameatal tubercle. This reduces the extent of bone resection and, in a few cases, drilling may not be required at all. We however note that suprameatal drilling may be required in some cases when the tumor extends to the posterior cavernous sinus and the middle cranial fossa. The RTT approach goes in line with the evolving concept of maximizing tumor resection while minimizing the morbidity associated with cranial base surgery.
Our study has certain limitations. The use of frameless navigation for measuring the area of exposure and degree of surgical freedom improves accuracy and the objective nature of measurements. The study may not reflect the distortions produced by the tumor and its relation to the brainstem. Nevertheless, it is helpful to appreciate the extent of additional exposure obtained by incising the tentorium without drilling the suprameatal tubercle.
Conclusions
The RTT approach provides a simple and safe method of approaching tumors in the petroclival region. It provides greater exposure of the ventrolateral brainstem and petroclival surface. This approach can be used as a standalone or in conjunction with suprameatal drilling during surgery for petroclival meningioma.
Source of Funding
Nil.
References
- 1.Samii M, Ammirati M. The combined supra-infratentorial pre-sigmoid sinus avenue to the petro-clival region. Surgical technique and clinical applications. Acta Neurochir (Wien) 1988;95(1-2):6–12. doi: 10.1007/BF01793075. [DOI] [PubMed] [Google Scholar]
- 2.Spetzler R F, Daspit C P, Pappas C T. The combined supra- and infratentorial approach for lesions of the petrous and clival regions: experience with 46 cases. J Neurosurg. 1992;76(4):588–599. doi: 10.3171/jns.1992.76.4.0588. [DOI] [PubMed] [Google Scholar]
- 3.Chanda A Nanda A Retrosigmoid intradural suprameatal approach: advantages and disadvantages from an anatomical perspective Neurosurgery 200659101ONS1–ONS6., discussion ONS1-ONS6 [DOI] [PubMed] [Google Scholar]
- 4.House W F, De la Cruz A, Hitselberger W E. Surgery of the skull base: transcochlear approach to the petrous apex and clivus. Otolaryngology. 1978;86(5):ORL-770–ORL-779. doi: 10.1177/019459987808600522. [DOI] [PubMed] [Google Scholar]
- 5.Hsu F P, Anderson G J, Dogan A. et al. Extended middle fossa approach: quantitative analysis of petroclival exposure and surgical freedom as a function of successive temporal bone removal by using frameless stereotaxy. J Neurosurg. 2004;100(4):695–699. doi: 10.3171/jns.2004.100.4.0695. [DOI] [PubMed] [Google Scholar]
- 6.Kanzaki J, Kawase T, Sano K, Shiobara R, Toya S. A modified extended middle cranial fossa approach for acoustic tumors. Arch Otorhinolaryngol. 1977;217(1):119–121. doi: 10.1007/BF00453899. [DOI] [PubMed] [Google Scholar]
- 7.Kawase T, Toya S, Shiobara R, Mine T. Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg. 1985;63(6):857–861. doi: 10.3171/jns.1985.63.6.0857. [DOI] [PubMed] [Google Scholar]
- 8.Malis L I. The petrosal approach. Clin Neurosurg. 1991;37:528–540. [PubMed] [Google Scholar]
- 9.Quiñones-Hinojosa A Chang E F Lawton M T The extended retrosigmoid approach: an alternative to radical cranial base approaches for posterior fossa lesions Neurosurgery 200658402ONS-208–ONS-214., discussion ONS-214 [DOI] [PubMed] [Google Scholar]
- 10.Koerbel A, Kirschniak A, Ebner F H, Tatagiba M, Gharabaghi A. The retrosigmoid intradural suprameatal approach to posterior cavernous sinus: microsurgical anatomy. Eur J Surg Oncol. 2009;35(4):368–372. doi: 10.1016/j.ejso.2008.02.011. [DOI] [PubMed] [Google Scholar]
- 11.Mathiesen T Gerlich A Kihlström L Svensson M Bagger-Sjöbäck D Effects of using combined transpetrosal surgical approaches to treat petroclival meningiomas Neurosurgery 2007606982–991., discussion 991-992 [DOI] [PubMed] [Google Scholar]
- 12.Nanda A, Javalkar V, Banerjee A D. Petroclival meningiomas: study on outcomes, complications and recurrence rates. J Neurosurg. 2011;114(5):1268–1277. doi: 10.3171/2010.11.JNS10326. [DOI] [PubMed] [Google Scholar]
- 13.Natarajan S K Sekhar L N Schessel D Morita A Petroclival meningiomas: multimodality treatment and outcomes at long-term follow-up Neurosurgery 2007606965–979., discussion 979-981 [DOI] [PubMed] [Google Scholar]
- 14.Samii M, Tatagiba M, Carvalho G A. Retrosigmoid intradural suprameatal approach to Meckel's cave and the middle fossa: surgical technique and outcome. J Neurosurg. 2000;92(2):235–241. doi: 10.3171/jns.2000.92.2.0235. [DOI] [PubMed] [Google Scholar]
- 15.Kawamata T, Katayama Y. [Lateral supracerebellar transtentorial approach for petroclival lesions] No Shinkei Geka. 2006;34(6):567–575. [PubMed] [Google Scholar]
- 16.Seoane E, Rhoton A L Jr. Suprameatal extension of the retrosigmoid approach: microsurgical anatomy. Neurosurgery. 1999;44(3):553–560. doi: 10.1097/00006123-199903000-00065. [DOI] [PubMed] [Google Scholar]
- 17.Campbell E, Whitfield R D. Posterior fossa meningiomas. J Neurosurg. 1948;5(2):131–153. doi: 10.3171/jns.1948.5.2.0131. [DOI] [PubMed] [Google Scholar]
- 18.Russell J R, Bucy P C. Meningiomas of the posterior fossa. Surg Gynecol Obstet. 1953;96(2):183–192. [PubMed] [Google Scholar]
- 19.Park C K Jung H W Kim J E Paek S H Kim D G The selection of the optimal therapeutic strategy for petroclival meningiomas Surg Neurol 2006662160–165., discussion 165-166 [DOI] [PubMed] [Google Scholar]
- 20.Zentner J, Meyer B, Vieweg U, Herberhold C, Schramm J. Petroclival meningiomas: is radical resection always the best option? J Neurol Neurosurg Psychiatry. 1997;62(4):341–345. doi: 10.1136/jnnp.62.4.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Natarajan S K Sekhar L N Schessel D Morita A Petroclival meningiomas: multimodality treatment and outcomes at long-term follow-up Neurosurgery 2007606965–979., discussion 979-981 [DOI] [PubMed] [Google Scholar]
- 22.Watanabe T, Katayama Y, Fukushima T, Kawamata T. Lateral supracerebellar transtentorial approach for petroclival meningiomas: operative technique and outcome. J Neurosurg. 2011;115(1):49–54. doi: 10.3171/2011.2.JNS101759. [DOI] [PubMed] [Google Scholar]