

Abstract
Background:
Body concerns and its health consequences such as eating disorders and harmful body change activities are mentioned in Asian countries. This study evaluates factors contributing to body image/shape changes in an Iranian population.
Methods:
In this cross-sectional study we focused on four main body change activity (diet, exercise, substance use, and surgery) and their risk factors such as demographic variables, Body Mass Index (BMI), Media, Body-Esteem, Perceived Socio-cultural Pressure, Body dissatisfaction and, Self-Esteem. Approximately, 1,200 individuals between 14-55 years old participated in this study. We used a multistage sampling method. In each region, the first household was selected at random. The probability of outcomes was estimated from logistic models.
Results:
About 54.3% of respondents were females. The mean (SD) of age was 31.06 (10.24) years. Variables such as gender, age, BMI, use of media and socio cultural factors as, body dissatisfaction, body-esteem and pressure by relatives were the main factors that influenced body change methods. In particular we have seen that male are 53% less likely to follow surgical treatments, but 125% were more likely to use substances.
Conclusions:
Investigation of body concern and its health related problem should be assessed in cultural context. For effectiveness of interventional programs and reducing harmful body image/shape changes activities, socio-cultural background should be noted.
Keywords: Body change activities, body concern, Iran
INTRODUCTION
Body image has been defined as a person's perception, feelings and thoughts about his or her body, usually conceptualized as incorporating body size estimation, evaluation of body attractiveness and emotions associated with body shape and size.[1] The discrepancy between the perception about body (current image) and the desired body (ideal body) can cause body dissatisfaction. This can lead to many health problems, such as low self-esteem, eating disorders and risky behaviors for body image/shape changes (e.g., severe dieting; intense exercise; the use of laxatives, diuretics, steroids; and invasive cosmetic surgery).[2]
One of the consequences and behavioral aspects of body dissatisfaction is the need to change one's body shape and weight. Neumark-Sztainer et al. (2003) found approximately 77% of unhealthy weight control behaviors among girls and 70% of such behaviors in boys are related to body and weight dissatisfaction.[3]
The frequency of using some form of body fitness or weight loss method can be as high as one-half in girls and one-third in boys.[4] The desire for thinness is greater among girls than among boys.[5] One example of a body changing activity is dieting behavior, which may include changes in eating patterns, unhealthy eating behaviors (i.e., low-calorie diets, diet pills, fad diets), associated harmful behaviors (i.e., vomiting and laxative use), and dieting to the extreme, resulting in conditions such as anorexia, bulimia nervosa or other eating disorders.[6] As previously stated, females wish to be thinner, and males wish to be more masculine. These desires can cause males to exercise excessively and engage in steroid use, and females prefer dieting strategies or surgery.[2] Cosmetic surgeries are one of the most invasive activities. The American Society of Plastic Surgeons (ASPS) reported that approximately 13.1 million cosmetic surgeries were performed in 2010 in USA.[7] Some researchers argue that body and appearance dissatisfaction are associated with cosmetic surgery.[8] Such behavior correlates with gender, as females and older persons are more inclined to pursue cosmetic surgeries.[8]
Various socio-cultural factors can also impact body dissatisfaction, eating disorders and decisions about body image/shape changes. Researchers argue that socio-cultural factors can affect individuals via cultural norms.[9,10]
Despite previous beliefs, body concerns and eating disorders are increasing in Asian countries, and in some of these societies, their prevalence is similar to that of western cultures. Body dissatisfaction score was estimated in South east Asia, East Asia, South and West Asia about 0.9, 1.1 and 0.5, respectively this score was about 1.1 in Scandinavia and 1.4 in North America.[11] The prevalence of bulimia nervosa is about 0.3% to 7.3% in females in Western countries and in non-Western countries is about 0.5% to 3.2% in females.[12] In Asian cultures, however, obesity symbolized health and wealth, whereas thinness was perceived as unhealthy and poor.[13] Exposure to western cultures has changed the traditional views and attitudes of many Eastern cultures.[14,15] Researchers contend that there are many cultural differences within east Asian countries. There are multiple differences between Asian cultures that can affect an individual's perceptions, attitudes and behaviors.[10] For example, in East Asia, Japanese women suffer more from eating disorders and body dissatisfaction than Taiwanese women.[16] There are, also significant differences between Eastern and Western Asian cultures, as the majority of west Asian countries are Muslim. These cultures stress the importance of Islamic law, such as requiring the covering of the body, especially in women. Covering of body may be results to better body satisfaction and reduce preoccupation with the body.[17]
However, there are few related studies about body dissatisfaction, body image/shape changes behavior, eating disorders and contributing factors in Iran. The aim of this study was providing a better understanding of body image and also exploring the factors that contribute to body change activities among Iranian populations, as an Asian culture. We anticipate that the findings of the study will provide relevant information for prevention programs, especially preventive programs planning for reduction of harmful body dissatisfaction consequences such as eating disorders.
METHODS
This population-based study was carried out in Kerman, the capital of the largest province in Iran. This cross-sectional survey was conducted as a part of a larger study “Body satisfaction and related issues in Iran”. The main outcomes of this study focus on the approaches that people prefer to follow to change their body shape. We focused on four main methods: Diet, exercise, substance use and surgery.
Sample size and sampling approach
As we estimated, approximately 20 regression coefficients (such as demographic variables, body mass index, body dissatisfaction, body steam, comparison with others, social pressure for body change and self steam), at least 200 events were necessary. Performing a pilot study, we assumed that the rate of body management methods (i.e., diet, exercise, drug use, and surgery) would not be lower than 0.15. With Power of 80% and type one error of 5% we recruited approximately 1,200 subjects who ranged in age from 14 to 55 years.
We adopted a multistage sampling. In each household, only one subject was interviewed. This was done to ensure independency of samples, and to avoid similarity between subject's characteristics within households. This study was approved by the Medical Thesis and Ethical Committee of the Kerman Medical Sciences University. All of participants signed informed consent.
Outcomes
Body change activities included diet (food restriction, induced vomiting), exercise (heavy exercise for masculinity or weight reduction), substance use (steroids, muscle-enhancing products, such as creatine and weight reduction pills) and cosmetic surgery (rhinoplasty, breast augmentation, liposuction). The use of non-surgical procedures such as botox injections, were not considered.
RISK FACTORS
Demographics/characteristics
We collected demographic characteristics of subjects, including gender, age (<20, 20-40, >40 years old), and marital status (single, married, divorce or widowed).
Socio-economic status
These items included education (illiterate or elementary school, high school, and university degree), occupation, and economic status (low, medium, good and excellent). To assess the economic status, we simply asked respondents to select one of three options.
Body mass index
In addition, weight and height were measured by trained persons using standardized methods.[18] To assess the association between BMI level and gender in adults, applying cut-offs at 18.5, 24.9, and 29.9, subjects were categorized into four groups: BMI < 18.5 (thin), BMI = 18.5-24.9 (normal), BMI = 25-29.9(overweight), BMI > 30 (obese)[18] for adults. (only 3.8% of our sample was adolescents aged <19 years old).
Media
To evaluate the impact of media on body change strategies, we asked subjects that they used western satellite, television, magazines or the Internet. Therefore, responses were binary (yes, no).
Socio-cultural measures
Socio-cultural variables were evaluated using the following instruments.
Physical appearance comparison scale
This questionnaire is a five-item Likert-type scale instrument with responses ranging from never (0) to all the time (5). This scale assesses the tendency to compare one's body with those of others. This instrument has acceptable reliability and validity for body image assessment.[19]
For the assessment of psychometric properties of the Persian version of PACS, the following steps were performed
Translation-back-translation
The PACS questionnaire was translated into Persian by an Iranian translator and then back-translated to English by two native English speakers who were familiar with body image concerns. Any differences between the original English version and the translated form were resolved by an expert panel. Conceptual and linguistics equivalents of the items were approved by this panel.
Internal consistency
Internal consistency was assessed by Cronbach's alpha coefficient with an alpha level of 0.72. In an item-scale correlation, we realized that excluding anyone of items 1, 2, 3, or 5 reduced the alpha level. However, exclusion of item 4 resulted in an increase in the alpha level from 0.72 to 0.84. In addition, the correlation between item 4 and the scale (after correction for overlapping) was as low as 0.02. Therefore, it seemed that item 4 could be excluded. For a final check, a factor analysis was performed, and the results showed that item 4 was placed into a separate category. This result was also identified in other studies.[9,20] Therefore, the final analysis of PACS was conducted using 4 items (1, 2, 3, and 5), that was named PACS4.
Convergent validity
The correlation between self-esteem and body satisfaction is known, as research has established that women and men who are more secure with their body image have a higher self-esteem.[20] Therefore, we used the Persian version of Rosenberg self-esteem scale,[21] to assess the convergent validity of the PACS questionnaire.[22] The correlation between the two questionnaires was −0.28, P < 0.0001.
Body-esteem scale for adolescents and adults
This self-reported, Likert-type scale consists of 23 items that evaluated three subscales: BE-Appearance (general feeling about self), BE-Weight (satisfaction) and BE-Attribution (judgment of other's view). The subscales have high internal consistency and 3-month test-retest reliability.[22]
After the translation and back-translation were performed, psychometric properties of the Persian version were assessed. Internal consistency and item-scale correlation were acceptable. The alpha value was 0.88. The item-scale correlation after correction for overlapping ranged from 0.18 to 0.70.
Perceived socio-cultural pressure scale
This inventory includes 10 items that assess the role of friends, media, dating partner and family on one's decision to change physical appearance.[23]
For this study, psychometric properties of the Persian version of Perceived Socio-Cultural Pressure Scale (PSPS) were assessed. The Persian version of this questionnaire had acceptable reliability (α = 0.92). To assess the convergent validity, Rosenberg's self-esteem scale was used. The Pearson's correlation coefficient was −0.26, P < 0.0001.
Body dissatisfaction
In this study, we applied a figure rating scale,[24] which has been used for assessment of body image.[25] This scale includes nine silhouettes (male and female) that are numbered from 1 (very thin) to 9 (severely obese). The subjects were asked to identify the image that is most similar to their own current size and shape. They were also asked which image they would most prefer to be (ideal body type). Body Dissatisfaction (BD) was assessed by calculating the absolute difference between the current and the ideal size.[25] Psychometric properties of the figure rating scale have been used in Persian.[26]
The subjects were classified into three groups: No body dissatisfaction (i.e., BD = 0), mild dissatisfaction (BD = 1), and severe dissatisfaction (BD > 1). BD of zero indicates that subjects’ current and ideal shapes were the same. Cut off of 1 was selected to ensure adequate sample size in mild and severe BD groups.
Rosenberg self-esteem scale
To assess self-esteem, the Rosenberg Self-Esteem Scale (RSE) was used. This questionnaire includes 10 global statements that are scored 1= “strongly disagree” to 4= ” strongly agree”. The psychometric properties of the Persian version of the questionnaire were assessed.[21]
Statistical analysis
Descriptive statistics were used to summarise the data. A series of multifactorial logistic regression models were applied to identify the factors that influence each of the outcomes or body management methods (i.e., diet, exercise, drug, surgery). The results are presented in terms of the odds ratio (OR), associated confidence intervals (CI), and P value.
In addition, the probability of outcomes was estimated from developed logistic models. The probability estimation were and then compared with the observed individual's status to calculate the correct classification proportion.
RESULTS
About 54.3% (652) of participants were female. The mean age was 31.06 ± 10.24 years with a minimum of 14 years. Nearly two-thirds of the participants were in the middle age group and approximately half of them had a university education. The mean (SD) for weight for males and females were 69.09 (10.83) Kg and 60.30 (12.58) Kg, respectively, P < 0.0001. Corresponding figures for height were 173.48 (6.63) cm and 162.56 (7.7) cm, P < 0.0001. Characteristics of respondents are shown in Table 1.
Table 1.
Characteristics of participants
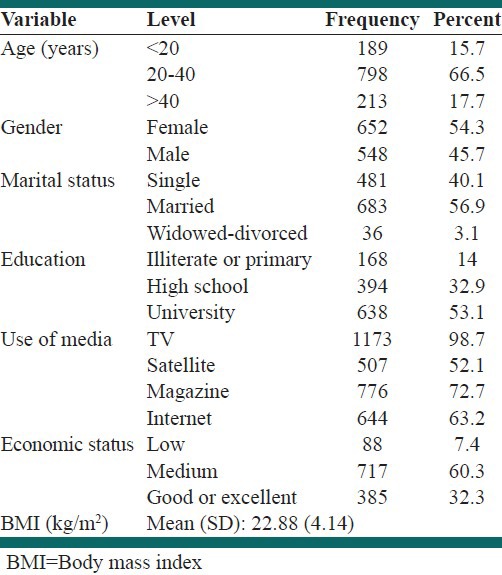
The mean for BMI was 22.88 ± 4.14 kg/m2. A significant difference between the BMI levels of males and females was found (P < 0.0001). Focusing on the two extreme BMI groups (i.e., thin and obese), we found that nearly three-forth and two-thirds of the subjects were female, respectively. We have observed that gender and age, BMI, media, body dissatisfaction, eating disorders, and scores on social pressures to engage in body change activities (PSPS), various aspects of body steam (BEA, BEAT, BEW), and comparison with others (PACS4) are all factors that persuade or dissuade subjects to manage their body shape.
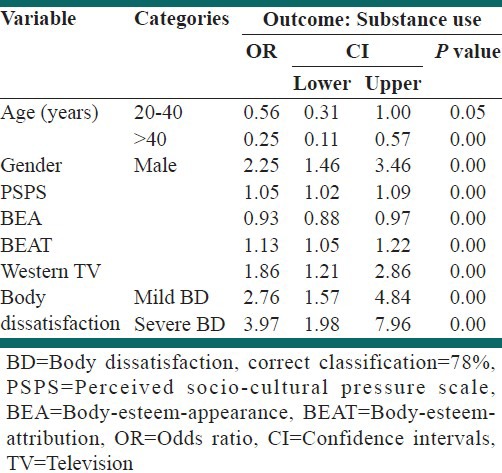
Regarding the factors that encourage people to manage their body shape through substance use, we find that age, gender, watching western television, body dissatisfaction, social pressures to engage in body change activities (PSPS), some aspects of body steam (BEA, and BEAT) are all influencing variables. Males were 2.25 (95% CI: 1.46, 3.46) times more likely to use substances than females (P < 0.001). Those who were severely dissatisfied with their body shape were nearly 4 times (95% CI: 1.98, 7.96) more likely to use substances than people who were satisfied with their body shape (P < 0.001). Other factors that persuade subjects to change body shape were watching western television, social pressures to engage in body change activities (PSPS score), and one aspect of body steam (BEAT score). Furthermore, older people and those with higher one aspect of body steam (BEA scores) were less likely to use substances [Table 2].
Table 2.
Identification of factors that encourage people to use substances use to manage their body shape through a multi factorial logistic regression
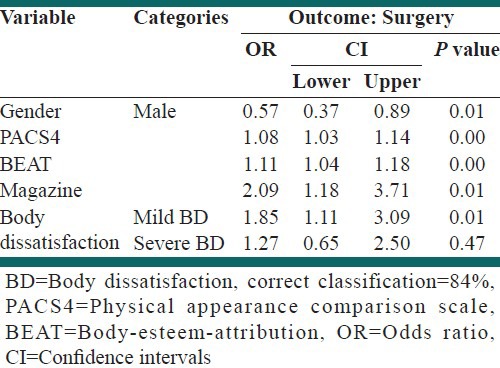
We also found that males were approximately 40% less likely to obtain surgical treatments than females. A one unit increase in one aspect of body steam (BEAT) and comparison with others (PACS4 scores) was associated with 11% and 9% increase, respectively, in the tendency to undergo surgery. Furthermore, the OR for surgery for those with mild body dissatisfaction, relative to satisfied subjects, was 1.86 (95% CI: 1.12, 3.09) (P < 0.001). The impact of magazines was remarkable: Participants who read magazines were 2.1 times (95% CI: 1.81, 3.72) more likely to manage their body shape through surgery (P < 0.001) [Table 3].
Table 3.
Identification of factors that encourage people to follow surgical treatment to manage their body shape through a multi factorial logistic regression
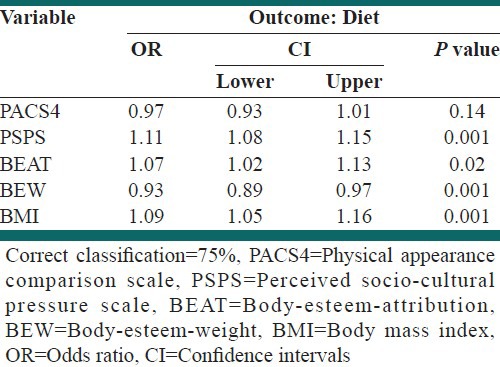
With respect to diet, we find that BMI, but not gender, was an important factor. One unit increase in BMI was associated with 9% increase in use of diet (95% C.I: 5%, 15%) with a P < 0.001. In addition to scores for some aspects of body steam (BEAT, BEW), and social pressures to engage in body change activities (PSPS), there were other influencing factors [Table 4].
Table 4.
Identification of factors that encourage people to diet as a way to manage their body shape through a multi factorial logistic regression
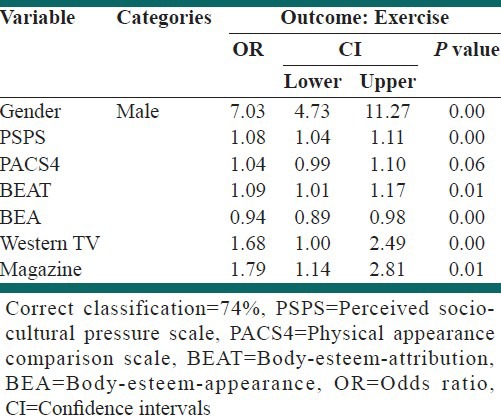
With respect to exercise, we found that the OR for males relative to females was 7.03 (95% CI: 4.74, 11.27) giving a P < 0.001. Furthermore, the impact of magazine reading and television watching on eating disorders was noticeable. These variables approximately increase the likelihood of doing exercise 70%. Other influencing factors were scores for social pressures to engage in body change activities (PSPS), some aspects of body steam (BEAT, BEW), and comparison with others (PACS4) [Table 5].
Table 5.
Identification of factors that encourage people to exercise and manage their body shape through a multi factorial logistic regression
DISCUSSION
This study explores the various body image/shape changes activities and the factors that contribute to the desire to achieve the ideal body among the Iranians. To achieve ideal body, individuals frequently use various methods such as dieting, food supplements, steroids and body building techniques.[4] Researches regarding substance use to induce body image/shape changes are inconsistent, which may be due to unreliable data concerning steroids and similar products.[5] Body concerns are important during adolescence. Pubertal changes are identified as predictors of body image/shape changes strategies that could induce biologic or psychological changes during adolescence.[27] Our findings are consistent with previous studies, and adolescents, especially boys, are more prone to use substances to induce body image/shape changes than girls. In recent years, Iran has experienced a considerable increase in body building clubs and advertisements that enhance the harmful physical and mental health side effects of nonstandard body-building techniques. Body dissatisfaction in men is a good predictor of extreme exercise and substance use including steroids and supplementary products.
Other than age, gender serves as a contributing factor in body satisfaction and in the choice of body image/shape changes methods. In contrast to other studies, gender had no effect on dieting attempts in this study. This finding may be due to the stronger effects of other variables that contributed to dieting, which could negate the effects of gender.
Body mass index (BMI) is considered a strong predictor of body image/shape changes in both sexes (R2 = 0.12 for girls and R2 = 0.26 for boys P < 0.001).[28] In some of societies, when considering BMI as a contributing factor to body image/shape changes activities, individuals who perceive themselves as overweight are at greater risk for eating disorders, as they attempt to lose weight (β = 0.24, P <.0001).[29] In our study, BMI is a predictive factor of strict dieting. There is evidence that a correlation between BMI and body dissatisfaction in women is higher than men [correlation between BMI and self-dissatisfaction was r = 0.256 for males (P < 0.0001) and r = 0.281 females (P < 0.0001)].[10] In men, BMI is an important factor in predicting heavy exercise for weight loss. Heavier women who are dissatisfied with their bodies attempt to lose weight, whereas men attempt to gain weight and increase muscle mass. Several Asian studies, however, found a greater BMI correlation with body dissatisfaction and weight loss in men.[10]
One of studies shows that low self-esteem is associated with body dissatisfaction,[29] young girls who perceived themselves as overweight had lower levels of self-esteem. In addition, self-esteem is negatively correlated with dieting [r= −0.20 (P < 0.001) and r= −0.18 in girls and boys, respectively, P < 0.001].[30] The some of inconsistent findings in our study may be due to the fact that these effects are mediated by other variables. These variables were comparisons between self and others or acceptance of pressure from others to be thin. Iranian women were determined to be vulnerable to pressure from their community to achieve the ideal body because they feared their acceptance would be negatively affected by their body.
As mentioned above, various socio-cultural factors have important role in body dissatisfaction, eating disorders and decisions about body image/shape changes. Social comparison is the process by which a person evaluates his/her own body image in comparison to others and is considered to be one of the predictors of body dissatisfaction and eating disorders.[31] Comparing one's own body with that of an ideal body image could be forced by other factors, such as family or peers, and result in body dissatisfaction.[5,9] Peer groups have a significant effect on body satisfaction and body image/shape changes activities. Although, this comparison appears higher in females, peer effect on body satisfaction and decisions about body image/shape changes were found to be higher in boys than girls (Mean score of Perceived pressure from peers to lose weight were 8.93 (4.05) vs. 7.95 (2.85) P <.01).[28] As family is one of the first institutions to teach values, behaviors and attitudes to individuals. It has direct (pressure for thinness) and indirect (modelling) effects on one's desire to be thin, a factor that can lead to body dissatisfaction, body image/shape changes activities and eating problems, especially among girls.[5,32] Encouragement to be thin by parents, to promote dieting have found that these factors can induce eating disorders in their both daughters and sons, equally [1.51 (1.04) and 1.45 (0.95) in daughters and sons, respectively, P > 0.05].[33]
Our findings show that socio-cultural factors, especially perceived pressure from others and comparison of oneself with others, are prominent variables in all body image/shape changes activities. In the Iranian culture, family is an important institution. Consequently, family members influence many aspects of an individual's life decisions. The role of the family is important in both preventing and treating eating disorders. Identifying the role of the family and its effects on body dissatisfaction and eating disorders in Iran are the subjects for future studies.
Among the factors that contribute to body image/shape changes activities, the role of the media must be mentioned. The media, for example, can play a significant role in body dissatisfaction as an ideal body image is promoted through the media that suggests thinness is the sign of attractiveness, beauty, social acceptance and success.[23] The internalization of the media's portrayal of the ideal body image may result in attempts to achieve the ideal body. Studies indicate that body dissatisfaction is greatest among adolescent girls that read more magazines and watch more television thin-ideal Commercials [M (SE)=32.7 (0.86)] and those viewing the non appearance commercials [M (SE)=27.7 (0.84)] and, respectively, P < 0.001).[34] The ideal male body, as promoted by the media, can cause males to strive to be lean and masculine.[34] The changes in body dissatisfaction in Asian societies could be the consequence of exposure to western ideal body images that promote thinness for women and masculinity for men.[9,35] In women, decisions regarding dieting are associated with the frequency of images about fitness, dieting and exercise that are viewed on television or in magazines.[34,35] The media images have been found to affect an individual's desire for cosmetic surgery. Xie et al., (2006) in one study that performed in China suggested that the influence of the Asian media on body dissatisfaction is in fact stronger than that of western media. They believed the reason of this findings was similarities between Asian media and Chinese culture.[36] In Iran however, while models in women's fashion magazines wear the traditional Islamic covering, which is found in men's magazines, formal dresses are advertised, thus introducing, albeit indirectly, the ideal body image. Furthermore, in Iranian movies, successful, intelligent and attractive actors and actresses especially young persons have the ideal body shapes and have often undergone cosmetic surgery, especially rhinoplasty. One area we focused on was cosmetic surgery, which was based on unofficial statistics and our experiences. We found that the rate of rhinoplasty in Iran is high, although additional studies are needed to confirm these findings.
Limitation
In current study, we present one of the few studies on body image, body satisfaction and body image/shape changes strategies and their contributing factors in Iran. Therefore, it is not surprising that there are several limitations in this study. One such limitation is the use of self-reported instruments, as more objective measures have better reliability. A qualitative study may be helpful in identifying future issues with respect to body image in Iran. Another contributing factor is religion, as its role in west Asian cultures is important. Although religion is not addressed in this study, a study by Rastmanesh et al., (2009) found that religious Iranian women who wear the traditional Islamic dress have a higher level of body satisfaction than non-religious Iranian women Mean ± SD of body dissatisfaction was about 65.3 ± 27.1 vs 107.5 ± 33.4 in religious and non-religious women, respectively, P < 0.001).[17]
CONCLUSIONS
Finally, Body image disturbances and eating disorders are new issues in Iran. It seem socio-cultural factors are predictive factors for body change strategies. Therefore, it is important that these contributing factors are identified for better interventional program planning in various cultures.
ACKNOWLEDGMENT
The authors sincerely thank Dr. Beverly K. Mendelson, Dr. Eric Stice and Dr. J. Kevin Thompson for giving us the opportunity of using questionnaires and their cooperation. Also, we thank Dr. Neuzar Nakhaee for his guidance and cooperation.
Footnotes
Source of Support: This research was financially supported by Neurosciences Research Center of Kerman University of Medical Sciences
Conflict of Interest: None declared
REFERENCES
- 1.Grogan S. Body image and health: Contemporary perspectives. J Health Psychol. 2006;11:523–30. doi: 10.1177/1359105306065013. [DOI] [PubMed] [Google Scholar]
- 2.Stice E, Hayward C, Cameron R, Killen JD, Taylor CB. Body image and eating related factors predict onset of depression in female adolescents: A longitudinal study. J Abnorm Psychol. 2000;109:438–44. [PubMed] [Google Scholar]
- 3.Neumark-Sztainer D, Wall M, Story M, Perry CL. Correlates of unhealthy weight control behaviours among adolescent girls and boys: Implications for the primary prevention of disorderedeating. Health Psychol. 2003;22:88–98. doi: 10.1037//0278-6133.22.1.88. [DOI] [PubMed] [Google Scholar]
- 4.Neumark-Sztainer D, Wall M, Eisenberg ME, Story M. Obesity and eating disorders in older adolescents: Does early dieting make things better or worse? J Adolesc Health. 2005;36:152–3. [Google Scholar]
- 5.McCabe MP, Ricciardelli LA, James T. A longitudinal study of body change strategies of fitness centre attendees. Eat Behav. 2007;8:492–6. doi: 10.1016/j.eatbeh.2007.01.004. [DOI] [PubMed] [Google Scholar]
- 6.Breitkopf CR, Berenson AB. Correlates of weight loss behaviours among low-income African-American, Caucasian, and Latina women. Obstet Gynecol. 2004;103:231–9. doi: 10.1097/01.AOG.0000110244.73624.b1. [DOI] [PubMed] [Google Scholar]
- 7.American Society of Plastic Surgeons. Report of the 2010 of plastic surgery statistics. Retrieved from March 8. 2011. http://www.plasticsurgery.org .
- 8.Henderson-King D, Henderson-King E. Acceptance of cosmetic surgery: Scale development and validation. Body Image. 2005;2:137–49. doi: 10.1016/j.bodyim.2005.03.003. [DOI] [PubMed] [Google Scholar]
- 9.Jackson T, Chen H. Sociocultural predictors of physical appearance concerns among adolescent girls and young women from China. Sex Roles. 2008;58:402–11. [Google Scholar]
- 10.Yates A, Edman J, Aruguete M. Ethnic differences in BMI and body/self-dissatisfaction among Whites, Asian subgroups, Pacific Islanders, and African-Americans. J Adolesc Health. 2004;34:300–7. doi: 10.1016/j.jadohealth.2003.07.014. [DOI] [PubMed] [Google Scholar]
- 11.Swami V, Frederick DA, Aavik T, Alcalay L, Allik J, Anderson D, et al. The attractive female body weight and female body dissatisfaction in 26 countries across 10 world regions: Results of the international body project I. Pers Soc Psychol Bull. 2010;36:309–25. doi: 10.1177/0146167209359702. [DOI] [PubMed] [Google Scholar]
- 12.Makino M, Tsuboi K, Dennerstein L. Prevalence of eating disorders: A comparison of western and non-western countries. Med Gen Med. 2004;6:49. [PMC free article] [PubMed] [Google Scholar]
- 13.Luo Y, Parish WL, Laumann EO. A population-based study of body image concerns among urban Chinese adults. Body Image. 2005;2:333–45. doi: 10.1016/j.bodyim.2005.09.003. [DOI] [PubMed] [Google Scholar]
- 14.Abdollahi P, Mann T. Eating disorder symptoms and body image concerns in Iran: Comparisons between Iranian women in Iran and in America. Int J Eat Disord. 2001;30:259–68. doi: 10.1002/eat.1083. [DOI] [PubMed] [Google Scholar]
- 15.Gunewardene A, Huon GF, Zheng R. Exposure to westernization and dieting: A cross-cultural study. Int J Eat Disord. 2001;29:289–93. doi: 10.1002/eat.1020. [DOI] [PubMed] [Google Scholar]
- 16.Shih M, Kubo C. Body shape preference and body satisfaction in Taiwanese college students. Psychiatry Res. 2002;111:215–28. doi: 10.1016/s0165-1781(02)00138-5. [DOI] [PubMed] [Google Scholar]
- 17.Rastmanesh R, Gluck ME, Shadman Zh. Comparison of body dissatisfaction and cosmetic rhinoplasty with levels of veil practicing in Islamic women. Int J Eat Disord. 2009;42:339–45. doi: 10.1002/eat.20613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Al-Sendi AM, Shetty P, Musaiger AO. Prevalence of overweight and obesity among Bahraini adolescents: A comparison between three different sets of criteria. Eur J Clin Nutr. 2003;57:471–4. doi: 10.1038/sj.ejcn.1601560. [DOI] [PubMed] [Google Scholar]
- 19.Thompson JK, Heinberg L, Tantleff S. The Physical Appearance Comparison Scale (PACS) Behav Ther. 1991;14:174–162. [Google Scholar]
- 20.Keery H, Kerri B, van den Berg P, Thompson JK. The impact of appearance-related teasing by family members. J Adolesc Health. 2005;37:120–7. doi: 10.1016/j.jadohealth.2004.08.015. [DOI] [PubMed] [Google Scholar]
- 21.Shapurian R, Hojat M, Nayerahmadi H. Psychometric characteristics and dimensionality of a Persian version of the Rosenberg Self-Esteem Scale. Percept Mot Skills. 1987;65:27–34. doi: 10.2466/pms.1987.65.1.27. [DOI] [PubMed] [Google Scholar]
- 22.Mendelson BK, Mendelson MJ, White DR. Body-esteem scale for adolescents and adults. J Pers Assess. 2001;76:90–106. doi: 10.1207/S15327752JPA7601_6. [DOI] [PubMed] [Google Scholar]
- 23.Stice E, Bearman K. Body-image and eating disturbances prospectively predict increases in depressive symptoms in adolescent girls: A growth curve analysis. Dev Psychol. 2001;37:597–607. doi: 10.1037//0012-1649.37.5.597. [DOI] [PubMed] [Google Scholar]
- 24.Stunkard AJ, Sorensen T, Schulsinger F. Use of the Danish adoption register for the study of obesity and thinness. Res Publ Assoc Res Nerv Ment Dis. 1983;60:115–20. [PubMed] [Google Scholar]
- 25.Fallon AE, Rozin P. Sex differences in perceptions of desirable body shape. J Abnorm Psychol. 1985;94:102–5. doi: 10.1037//0021-843x.94.1.102. [DOI] [PubMed] [Google Scholar]
- 26.Zanjani Z, Goodarzi MA. Reliability and validity of Figure Rating Scale in Shiraz students. Mental Health Principles. 2007;10:149–55. In Persian. [Google Scholar]
- 27.Jones DC. Social comparison and body image: Attractiveness comparison to models and peers among adolescent girls and boys. Sex Roles. 2001;45:645–64. [Google Scholar]
- 28.Mellor D, McCabe M, Ricciardelli L, Yeow J, Daliza N, Hapidzal NF. Sociocultural influences on body dissatisfaction and body change behaviors among Malaysian adolescents. Body Image. 2003;6:121–8. doi: 10.1016/j.bodyim.2008.11.003. [DOI] [PubMed] [Google Scholar]
- 29.Lee AM, Lee S. Disordered eating in three communities of China: A comparative study of female high school students in Hong Kong, Shenzhen and rural Hunan. Int J Eat Disord. 2000;27:317–27. doi: 10.1002/(sici)1098-108x(200004)27:3<317::aid-eat9>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 30.Friestad C, Rise J. A longitudinal study of the relationship between body image, self esteem and dieting among 15-21 year olds in Norway. Eur Eat Disord Rev. 2004;12:247–55. [Google Scholar]
- 31.van den Berg P, Thompson JK, Obremski BK, Coovert M. The tripartite influence model of body image and eating disturbance: A covariance structure modelling investigation testing the meditational role of appearance comparison. J Psychosom Res. 2002;53:1007–20. doi: 10.1016/s0022-3999(02)00499-3. [DOI] [PubMed] [Google Scholar]
- 32.Abramovitz BA, Birch LL. Five-year-old girls’ ideas about dieting are predicted by their mothers’ dieting. J Am Diet Assoc. 2000;100:1157–63. doi: 10.1016/S0002-8223(00)00339-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Vincent MA, McCabe MP. Gender differences among adolescents in family, and peer influences on body dissatisfaction, weight loss, and binge eatingbehaviours. J Youth Adolesc. 2000;29:205–21. [Google Scholar]
- 34.Hargreaves DA, Tiggemann M. The effect of ‘thin ideal’ television commercials on body dissatisfaction and schema activation during early adolescence. J Youth Adolesc. 2003;32:367–73. [Google Scholar]
- 35.Muris P, Meesters C, van den Blom W, Mayer B. Biological, psychological, and socio cultural correlates of body change strategies and eating problems in adolescent boys and girls. Eat Behav. 2005;6:11–22. doi: 10.1016/j.eatbeh.2004.03.002. [DOI] [PubMed] [Google Scholar]
- 36.Xie B, Chou C, Spruijt-Metz D, Reynolds K, Clark F, Palmer PH. Weight perception and weight-related socio-cultural and behavioural factors in Chinese adolescents. Prev Med. 2006;42:229–34. doi: 10.1016/j.ypmed.2005.12.013. [DOI] [PubMed] [Google Scholar]