

Abstract
Background:
Measurement of peak expiratory flow (PEF) is imperative for management and evaluation of asthmatic children. It is well-known that lung function parameters show wide variations with respect to regional, racial, and genetic factors.
Aim:
This study was conducted to measure PEF in healthy Punjabi children aged 7-14 years as only a few studies have evaluated the lung functions in North Indian children.
Materials and Methods:
A cross-sectional study was conducted in which PEF was measured in 366 healthy schoolchildren (186 boys and 180 girls) of Patiala district, using the Mini Wright Peak Flow Meter. Best of the three trials was recorded. All the subjects were tested in standing position after recording their age, height, and weight. SPSS v. 13 was used for the statistical analysis.
Results:
The present study showed that all the three independent variables (age, height, and weight) had a significant positive correlation with PEF, in both genders. Furthermore, height was maximally correlated with PEF in both boys (r = 0.970) and girls (r = 0.964). The mean PEF value in boys (249.34 ± 81.36 L/min) was significantly higher than girls (233.31 ± 67.06 L/min). Regression equations for PEF were also determined using age, height, and weight, separately for the genders.
Conclusion:
Equations derived from this study for estimation of expected PEF values would help the clinicians in assessing the airway obstruction in this population subset.
Keywords: Airway obstruction, lung function, peak expiratory flow, prediction equation, punjab, school children
INTRODUCTION
Peak expiratory flow (PEF) is the maximum flow rate generated during a forceful exhalation, starting from full lung inflation. It primarily reflects large airway flow and depends on the voluntary effort and muscular strength of the patient.[1] The Mini Peak Flow Meter is a useful instrument that is widely used for PEF measurement on an ambulatory basis.[2] This lung function parameter is quite useful as a screening tool to monitor the prevalence and severity of asthma in a community, especially, since the number of asthma and asthma related hospital admissions is continuously rising.[3] In 2007, an expert panel of the National Asthma Education and prevention program recommended periodic assessment of pulmonary function by spirometry or peak flow monitoring.[4]
It is a well-known fact that lung function parameters vary considerably between different regional and ethnic groups, residing within the same country.[5] Therefore, ideally speaking, all the Indian states and geographical regions as well as communities must have their own separate norms for these parameters.
Although, many studies have evaluated the PEF values in the children from various regions in India, but their results cannot be extrapolated to Punjabi children, since not only the environment, but also the customs, traditions, and life-style are altogether different in this part of the country.[6,7,8] Around 3 decades ago, Malik et al.[9,10] provided reference data for PEF in 5-16 year old Punjabi boys and girls. However, till date, no other similar study has been conducted in this region.
According to a recent report from a Government Agency, the air quality in the State of Punjab has undergone rapid deterioration over the last 30 years. This has been attributed mainly to rapid urbanization, mechanization of agriculture and excessive vehicular and industrial emissions.[11] Since air quality has a direct impact on lung function, hence the results of Malik et al. may not be relevant in the present day scenario. Thus, we felt the need to carry out a study to obtain newer reference values of PEF in Punjabi children aged 7-14 years.
MATERIALS AND METHODS
The study was conducted during March-August 2010 among a total of 366 school children, (186 boys and 180 girls) aged 7-14 years, studying in various schools in Patiala district, during their school hours. The study was approved by the ethical committee of the institute and was as per the Helsinki declaration. The prior permission of the school authorities was taken and written consent from the parents/guardians of all the children was also obtained after clearly explaining them the purpose of the study.
A detailed history, followed by a thorough clinical examination was carried out as per the criteria laid down by the American Thoracic Society.[12] All the available healthy children aged 7-14 years were included in the study except those with wheezing, visible bony and muscular deformities of chest wall and spinal cord, history of cardiac, renal and/or respiratory disease, history of medications like antiasthmatics, history of recurrent hospital admission or symptoms of respiratory tract infection within 3 weeks prior to the study, family history of asthma/allergy/chronic lung disease, clinically significant anemia, etc.
A total of 425 children were examined, out of which 59 children were excluded either due to exclusion criteria or due to unsatisfactory expiratory effort during the procedure. Reported age was confirmed from the school register. Weight was measured without shoes and with light clothing, on a standard calibrated bathroom scale. Height was measured with a standard portable stadiometer. It was ensured that all the participants belonged to comparable socio-economic status, which was determined as per modified Prasad's classification.[13]
The PEF values were then recorded in standing position, as per the standardized method, with the help of Mini Wright Peak Flow Meter (Clement Clarke International Limited, U.K.). The instrument was calibrated initially and also on all days during the study. Before testing, the procedure was explained and demonstrated to each child until full familiarity was achieved. Each child was told to take a deep breath and then blow into the peak flow meter as hard and fast possible. Every child was given two trial runs and encouraged to blow harder each time. The child then blew into the Mini Wright Peak Flow Meter thrice and the highest reading was accepted as the final PEF in each case. The mouthpiece was washed and sterilized for each subject.
Statistical analysis
The data obtained consisted of age, height, weight, and PEF values of all subjects, which were further processed for mean and standard deviation. Students’ unpaired t-test was used to compare the differences between the means. Age, height, and weight were the independent variables while PEF value was the dependent variable. Regression equations based on age, height, and weight were constructed separately for both boys and girls. Correlation between age, height, weight, and PEF was carried out using the Pearson's correlation. The statistical analysis was carried out with Statistical Package for Social Sciences (SPSS) version 13.0. P < 0.05 was considered statistically significant.
RESULTS
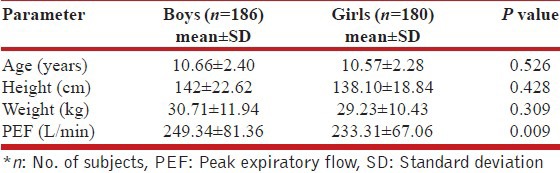
A total of 366 subjects (186 boys and 180 girls), in the age group of 7-14 years were studied. All of them belonged to urban areas. The mean anthropometric and PEF values are shown in Table 1. From this data it is clear that both boys and girls were comparable as regards to age, height, and weight. However, the mean PEF value of boys was significantly higher than girls (P = 0.009).
Table 1.
Comparison of anthropometric data and PEF values in study subjects
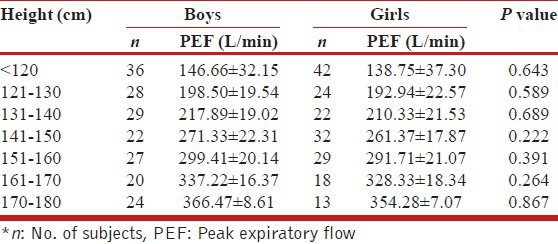
A comparison of mean PEF values of boys and girls belonging to various ages has been depicted in Table 2. It was seen that while the PEF values increased with age in both the genders, but the mean PEF of boys aged 12 years and above was significantly higher than girls. The mean PEF values according to weight have been illustrated in Table 3. It was observed that PEF showed a rise with weight in both the genders. However, the mean PEF value of boys weighing > 40 kg was significantly higher than girls, having similar weight. Table 4 compares the mean PEF values in study subjects according to various heights. It is clearly evident from the data obtained, that PEF values increase with the height and the mean PEF value of boys were comparable to girls at all heights.
Table 2.
Comparison of mean PEF values in study subjects according to age
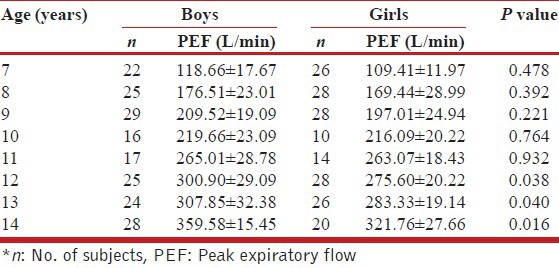
Table 3.
Comparison of mean PEF values in study subjects according to body weight
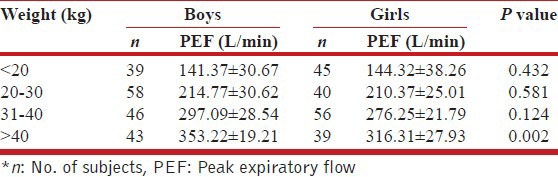
Table 4.
Comparison of mean PEF values in study subjects according to height
The prediction equations for PEF based on age, height and weight are given below for both boys and girls separately:
PEF (boys) = −150.38 + 9.19 × Age (years) + 1.75 × Ht (cm) +1.74 × Wt (kg)
R2 = 0.969, Standard Error of Estimate = ±14.43
PEF (girls) = −177.06 + 0.86 × Age (years) +2.59 × Ht (cm) +1.49 × Wt (kg)
R2 = 0.949, Standard Error of Estimate = ±15.66
DISCUSSION
The present study aimed at establishing the normal values of PEF in healthy Punjabi children, so that local reference standards are available for use by health-care professionals. This would prove beneficial in detecting early asthmatic changes and in providing a quantitative measure of improvement in response to treatment in asthmatic children, thereby improving their quality of life. From the prediction equations given by us, it will also be possible to calculate the PEF in Punjabi children.
In the present study, PEF showed a significant positive correlation (P < 0.001) with age, height, and weight. However, the highest correlation was obtained with height in both boys (r = 0.970) and girls (r = 0.964). Similar to our study results, many other authors have also found a significant positive correlation of PEF with age, height, and weight, out of which height has been maximally correlated with PEF.[14,15,16,17]
In the early 1980's, Malik et al.[9,10] had conducted a similar study in 5-16 year old Punjabi boys (n = 473) and girls (n = 132). The following prediction equations for PEF were given by them:
PEF (males) = −368.89 + 4.92 × Height (cm)
R2 = not available, Standard Error of Estimate = ±42.1
PEF (females) = −371.80 + 4.90 × Height (cm)
R2 = not available, Standard Error of Estimate = ±43.8
The above equations were applied on a small random sample of 50 children (26 boys and 24 girls), aged 7-14 years to calculate the predicted PEF values, which were then compared with their actual PEF values. None of the subjects had identical values of actual and predicted PEF. Furthermore, the differences between these values were within 10% in only 8 subjects, and in excess of 20-30% in rest of the subjects. Moreover, R2 (i.e., multiple correlation coefficient) values, which could have helped in establishing the statistical validity of these equations, were not made available by the authors. As per the American Thoracic Society recommendations,[18] a given regression equation can be considered suitable for a particular population only when the actual values of the lung function variables fall within 10% of the values predicted from that equation. The statistical approach to the equation generation also needs to be adequately described, for establishing its validity. The variation in actual PEF values obtained by us and those calculated by equations of Malik et al. could be due to the change in the air quality and life-style patterns of people in Punjab, over the last 3 decades. Therefore, due to the above considerations, we felt the need to provide newer reference values for PEF in Punjabi children.
We admit that forced expiratory volume over 1 s (FEV1), which is a dynamic measure of flow, is a better indicator of airway obstruction, as compared to PEF. However, the ease of measuring the PEF with an inexpensive portable device has made it preferable over FEV1. Moreover, as per the data available from previous studies carried out world-wide, PEF was found to have a significant positive correlation with FEV1.[19,20] Therefore, we feel that PEF may also be considered as a suitable alternative measure of airway obstruction in instances where FEV1 is unavailable.
CONCLUSION
In the present study, age, height, and weight have been used both alone as well as in combination to predict PEF values in North Indian Punjabi children. We hope that these prediction equations would prove useful for both the physiologists and clinicians of this region. There is a compelling need to conduct more similar studies among growing children in India, as the mosaic of Indian population, spreading over such a varying geography is quite complex.
ACKNOWLEDGMENTS
We would like to thank all the children without whose active co-operation; This study would have not been possible. We also extend our warm gratitude to the all the parents and school authorities for their much needed help and support.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Enright PL, Linn WS, Avol EL, Margolis HG, Gong H, Jr, Peters JM. Quality of spirometry test performance in children and adolescents: Experience in a large field study. Chest. 2000;118:665–71. doi: 10.1378/chest.118.3.665. [DOI] [PubMed] [Google Scholar]
- 2.Agaba PA, Thacher TD, Angyo IA, Agaba EI. Peak expiratory flow rates in healthy Nigerian children. J Trop Pediatr. 2003;49:157–9. doi: 10.1093/tropej/49.3.157. [DOI] [PubMed] [Google Scholar]
- 3.Enright P, McCormack M. Assessing the airways. Chron Respir Dis. 2008;5:115–9. doi: 10.1177/1479972308091578. [DOI] [PubMed] [Google Scholar]
- 4.United States Department of Health and Human Services: National Institutes of Health, National Heart, Lung and Blood Institute; [Updated 2012 April; Last Cited 2012 Dec 11]. Expert Panel Report 3 (EPR3): Guidelines for the diagnosis and management of asthma. Available from: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm . [Google Scholar]
- 5.Paramesh H. Normal peak expiratory flow rate in urban and rural children. Indian J Pediatr. 2003;70:375–7. doi: 10.1007/BF02723608. [DOI] [PubMed] [Google Scholar]
- 6.Vijayan VK, Reetha AM, Kuppurao KV, Venkatesan P, Thilakavathy S. Pulmonary function in normal south Indian children aged 7 to 19 years. Indian J Chest Dis Allied Sci. 2000;42:147–56. [PubMed] [Google Scholar]
- 7.Prasad R, Verma SK, Agrawal GG, Mathur N. Prediction model for peak expiratory flow in North Indian population. Indian J Chest Dis Allied Sci. 2006;48:103–6. [PubMed] [Google Scholar]
- 8.Chhabra SK, Vijayan VK, Rahman M, Mittal V, Singh PD. Regression equations for spirometry in children aged 6 to 17 years in Delhi region. Indian J Chest Dis Allied Sci. 2012;54:59–63. [PubMed] [Google Scholar]
- 9.Malik SK, Jindal SK, Sharda PK, Banga N. Peak expiratory flow rate of healthy schoolboys from Punjab. Indian Pediatr. 1981;18:517–21. [PubMed] [Google Scholar]
- 10.Malik SK, Jindal SK, Sharda PK, Banga N. Peak expiratory flow rates of school age girls from Punjab (Second report) Indian Pediatr. 1982;19:161–4. [PubMed] [Google Scholar]
- 11.Ministry of Environment and Forests, Govt. of India; [Last cited 2012 Dec 12]. State of Environment Punjab-2007 report. Available from: http://www.moef.nic.in/soer/state/SoE%20report%20of%20Punjab.pdf . [Google Scholar]
- 12.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 13.Sogi GM, Bhaskar DJ. Dental caries and oral hygiene status of school children in Davangere related to their socio-economic levels: An epidemiological study. J Indian Soc Pedod Prev Dent. 2002;20:152–7. [PubMed] [Google Scholar]
- 14.Mohammadzadeh I, Gharagozlou M, Fatemi SA. Normal values of peak expiratory flow rate in children from the town of Babol, Iran. Iran J Allergy Asthma Immunol. 2006;5:195–8. [PubMed] [Google Scholar]
- 15.Raju PS, Prasad KV, Ramana YV, Ahmed SK, Murthy KJ. Study on lung function tests and prediction equations in Indian male children. Indian Pediatr. 2003;40:705–11. [PubMed] [Google Scholar]
- 16.Sharma M, Sharma RB, Choudhary R. Peak expiratory flow rates in children of western Rajasthan, 7-14 years of age. Pak J Physiol. 2012;8:45–8. [Google Scholar]
- 17.Taksande A, Jain M, Vilhekar K, Chaturvedi P. Peak expiratory flow rate of rural school children from Wardha district, Maharashtra in India. World J Pediatr. 2008;4:211–4. doi: 10.1007/s12519-008-0039-1. [DOI] [PubMed] [Google Scholar]
- 18.American Thoracic Society. Lung function testing: Selection of reference values and interpretative strategies. American Thoracic Society. Am Rev Respir Dis. 1991;144:1202–18. doi: 10.1164/ajrccm/144.5.1202. [DOI] [PubMed] [Google Scholar]
- 19.Gibson PG. Monitoring the patient with asthma: An evidence-based approach. J Allergy Clin Immunol. 2000;106:17–26. doi: 10.1067/mai.2000.108307. [DOI] [PubMed] [Google Scholar]
- 20.Slieker MG, van der Ent CK. The diagnostic and screening capacities of peak expiratory flow measurements in the assessment of airway obstruction and bronchodilator response in children with asthma. Monaldi Arch Chest Dis. 2003;59:155–9. [PubMed] [Google Scholar]